Transcription
SBIRTIn Medical SettingsJim Winkle, MPHUpdated May, 2022
OutlineI. Why SBIRT? Categories of usePrevalence and morbidityRelevance to medical careII. Screening Brief screen, AUDIT, DAST, CRAFFT,5PsIII. Reimbursement and EHR toolsIV. Brief intervention Styles of communicationBrief intervention modelRole play practiceV. Referral to treatment Harm ReductionTreatment
Website: sbirtoregon.org Demonstration videos Screening forms Reimbursement information Pocket cards and tools Training curriculum Screening app
SBIRTScreeningBriefInterventionReferral toTreatment“A public health approach to the delivery of early interventionand treatment services for people with substance use disordersand those at risk of developing these disorders.”SAMHSA
egnancyCRAFFT5PsPopulationsCommon screening tools
I. Why SBIRT?
SBIRT vs. business as usualSBIRT implementedNo SBIRTRoutine and universal screening,regardless of medical complaintInconsistent, selective screeningValidated screening toolsNon-systemized narrative questionsSubstance use defined as a continuumSubstance use defined as dichotomousInterventions: evidence-based, patientdriven discussionIneffective, directive, or no discussionRecognizes patient is more than theirsubstance usePatient is defined by their use
Relevance to medical settings Significant prevalence of unhealthysubstance use among pts Substantial associated morbidity,mortality, and health care cost Valid screening instruments Interventions are effective,inexpensive, and feasible
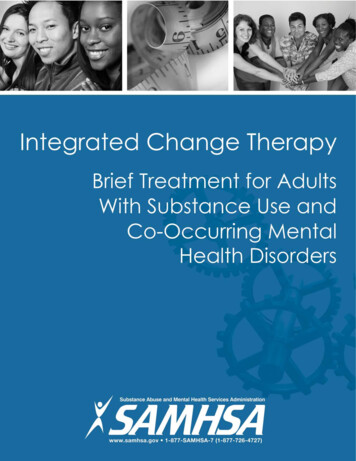
Categories of substance use, U.S.Number of consequencesDisorder (4%)Risky (21%)Frequency of useLow orno risk: 71%
Low riskDefined by: No use, or Adult alcohol use under riskylimitsLow-risk limits do not (yet) applyto cannabis or other drug use
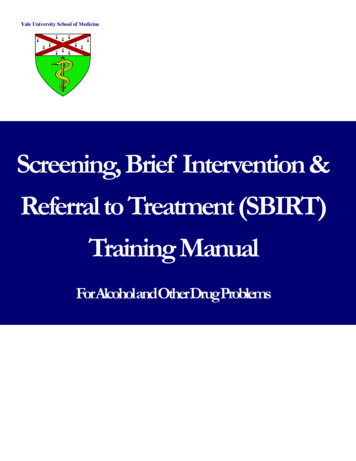
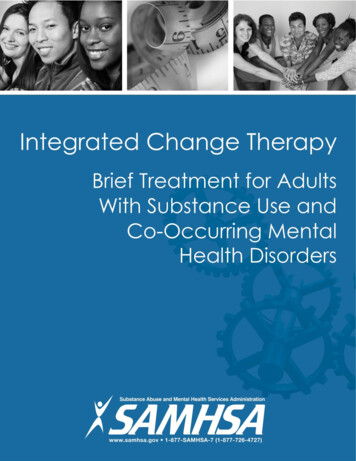
Adult limits for alcohol use, U.S.ModeratedrinkingBingedrinkingWomenNo more than1 drink per day4 drinks peroccasionMenNo more than2 drinks per day5 drinks peroccasionStandard drink in theU.S. defined as: 0.6 fluid ounces ofpure ethanol, or 14gramsDaily limits are “not intended as an average over several days, but rather the amountconsumed on any single day.”U.S. Department of Agriculture. NIAAA
Gender and alcohol limitsDrinking guidelines in Australia, U.K.,Portugal, and South Africa don’tdistinguish between men and women.Among 33 countries that do, low risk limitsrange from: 10 – 42g a day for women 84 – 140g a week for women 10 – 56g a day for men 100 – 280g a week for menKalinowski and Humphreys, 2016
Drawbacks of using only cisgender categoriesMissed opportunity to screen: 1.2 million people in the U.S. whoidentify as non-binary Reported higher rates of alcohol usethan cis gender people Study: 26% of trans people haveused substances to cope withmistreatmentCoulter et al, 2015. Keuroghlian et al, 2015. Wilson and Meyer, 2021.Williams et al, 2021. Grant et al, 2011
More factors correlated with risky drinking levelsDrinking on a full orempty stomachRaceToleranceVariations inself reportPeople more orless likely tounder reportEthnicityCertainmedicationsCountry of originRisk factors foralcoholcomplicationsFamily history ofcancer, heartdiseaseYoung versus olderadultsHistory of AUDor treatmentPeople currently inrecoveryBody MassIndexGeneticsContext/environmentStockwell, 2012
Standard drinks in the U.S.BeerMaltliquorVolume12 ozStandard drinks116 oz1.322 oz240 oz3.312 oz1.516 oz222 oz2.540 oz4.5NIAAA
Standard drinks, cont.WineLiquor(80 proof)VolumeStandard drinks5 oz1750-mL bottle51.5 liter bottle95 liter box301 mixed drink11 pint (16 oz.)11One fifth (25 oz.)171.75 liters (59 oz)39NIAAA
Disagreement over protective effects ofmoderate drinking Meta studies show J-shaped curvetowards mortality But studies involve selection bias andconfounders National Cancer Institute: even onedrink a day increases the risk ofbreast, esophageal and oral cancer.Xi et al, 2017
Low-risk alcohol limit for adolescents: 0 Even first use can result in tragicconsequences. Adolescence is a period ofneurodevelopmental vulnerability Earlier use increases chance of lateraddiction.AAP, 2016
RiskyRisky use defined as: Adult alcohol use that exceedsrisky limits Any adolescent use Any recreational drug use But not experiencing relatedconsequences
Disorder “Abuse”, “dependence” or“alcoholism” are terms no longer used Official term: Substance Use Disorder Criteria: 11 consequences experiencedin last 12 months 2 - 3 symptoms: mild4 - 5 symptoms: moderate6 symptoms: severeAmerican Psychiatric Association, 2013
11 criteria that define SUDs1.Taking the substance in larger amounts orfor longer than you're meant to.7.Giving up important social, occupational, orrecreational activities because of substance use.2.Wanting to cut down or stop using thesubstance but not managing to.8.Using substances again and again, even when itputs you in danger.3.Spending a lot of time getting, using, orrecovering from use of the substance.9.4.Cravings and urges to use the substance.Continuing to use, even when you know you havea physical or psychological problem that couldhave been caused or made worse by thesubstance.5.Not managing to do what you should atwork, home, or school because ofsubstance use.10.Needing more of the substance to get the effectyou want (tolerance).11.Development of withdrawal symptoms, which canbe relieved by taking more of the substance.6.Continuing to use, even when it causesproblems in relationships.American Psychiatric Association, 2013
Categories: prevalence and morbidityAdultsAdolescents Alcohol Cannabis Other drugsPregnancyXi et al, 2017
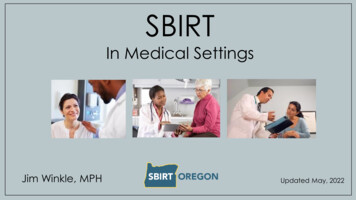
Estimated prevalence of unhealthy alcohol useamong adolescents and adults, 2020, U.S.Any drinkingin last 30 days(2019)Binge drinkingin last 30 daysHeavy drinkingin last 30 daysAUD inlast 12 monthsAge 12 - 179.4%4.1%0.6%2.8%Age 18 - 2554.3%31.4%8.6%15.6%Age 26 55.0%22.9%6.7%10.3%Binge drinking defined for males as drinking five or more drinks on the same occasion. Forfemales, four or more drinks. Heavy alcohol use is defined as binge drinking on 5 or more days inthe past 30 days.SAMHSA, 2021
Morbidity associated with risky adult drinking
Drinking among young adultsLarge, prospective cohortstudy: Heavy drinking duringearly adulthood raisesrisk for alcohol-relatedcancers Even after drinking stopsor decreases in middleageBassett et al, 2022
Morbidity associated with adolescentdrinking Altered braindevelopment Arrests &Incarceration Depressed cognitivefunctioning Injuries Premature death Alcohol poisoning Psychiatric disorders STDs, pregnancy Physical and sexualassaultsRyan and Kokotailo, 2019
Percent experiencing dependence in lifetime,based on age of first use, U.S.1009080706050403020100AlcoholMarijuana 1314151617Age started using18192021 Hingson et al 2006, SAMHSA 2010
Leading causes of adolescent death Alcohol majorcontributor to 74% ofpremature deathamong adolescentsNational Vital Statistics Reports, 2017
Prevalence of drinking alcohol among pregnantpatients in the last 30 days by age, 2015-201740302010018-2425-29Binge drank30-3435-44DrankBinge drinking defined as having four or more drinks on one occasion.Denny et al, 2019
Risks associated with alcohol use duringpregnancy Fetal alcohol spectrum disorders Miscarriage Premature birth Low birthweight Learning difficulties andbehavioral problems as a childNational Health Service, UK. 2020
Estimated prevalence of past-yearcannabis use, adolescents and adults, U.S.706050%Age 12-17Age 18-25Age 26 40302010004 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20SAMHSA, 2021
Correlations of heavy cannabis use during adulthoodInfrequent use: Car accidentsFrequent, long term use: Cannabis Use Disorder study:almost 20% of lifetime users Anxiety and depression Psychoses Respiratory problemsHasin DS, 2018. Volkow et al, 2014.
Correlations of heavy cannabis use during adolescence Reduced memory, attention andlearning abilities Poorer school performance Greater risk of addiction (1out of 6) Increased risk of psychosis orschizophrenia Increased risk of criminal behavior Increased risk of car accidentsU. of Washington, 2020
Estimated prevalence of past-monthcannabis use, pregnancyUnlike the generalpopulation,cannabis useamong peoplewho arepregnant hasalmost doubledsince 2002Volkow et al, 2019
Increased health risks associated withcannabis use during pregnancy Premature birth Fetal growth restriction Neural tube defects Anemia Problems with brain development StillbirthMarch of Dimes
Estimated prevalence of past-year drug use,adolescents and adults, 2017, U.S.2018%16Age 12-1714Age 18-2512Age 26 1086420SAMHSA
Opioid and Amphetamine use diagnosed at delivery“Amphetamine andopioid use affectingbirth representworsening publichealth crises.”Admon, et al, 2019
Missed opportunities with adult ptsCDC, 2014
Missed opportunities with adolescent ptsHammond et al 2021
Missed opportunities with pregnant ptsKo et al, 2020
Clinic-wide barriers to implementing SBIRTSurvey of 102 SBIRTproviders and 221SBIRT stakeholdersand staff.Scale used: 1 to a very little extent, 3 to some extent, 5 to a very great extent. (standard deviation)Vendetti et al 2017
Keys to sustainably implementing SBIRT Secure buy-in from leadership Identify workflow Train all staff and implementongoing training Identify champions Optimize EMR Use clinic tools
Beware: when implementing SBIRT Many states consider drug use duringpregnancy to be child abuse Pts identified with drug use facegreater stigma when receiving heathcare Efficacy of brief intervention dependson fidelity and quality – easier toensure during trials compared topractice.Saitz, JAMA, 2020
Meta studies: primary care interventions forunhealthy alcohol useSAdultsAdolescentsPregnancySBISBIRTfor balance of benefitsversus harmsfor reducing useor negative outcomesfor patient receipt ofspecialty treatmentModerate certainty:“small to no harm”Moderate evidenceInsufficient evidenceInsufficient evidence?Moderate certainty:“small to no harm”Moderate evidence?Evidence fornull effect*USPSTF, 2018. *Glass et al, 2015
Meta studies: primary care interventions forillicit drug useSfor balance of benefitsversus harmsAdultsAdolescentsPregnancy“No evidence”(USPSTF, 2020)“Moderate net benefitwhen treatment can beoffered”(Jin, 2020)SBIfor reducing useor negative outcomesSBIRTfor patient receipt ofspecialty treatment?Moderate evidence fornull effect(USPSTF, 2020)?
II. Screening
Common in-person clinic workflowsCRAFFTBrief screenAUDIT / DASTBriefintervention
Common ED in-person workflowsCRAFFTBrief screenAUDIT / DASTBriefintervention
Video:sbirtoregon.org
Adult screening toolssbirtoregon.org
Brief screenOne alcohol questionOne drug questionwww.sbirtoregon.org
Single alcohol questionInformed by: McNeely , et al. 2015. Flente et al, 2020.
Single drug question Sens: 93% Spec: 94% for past year, self-reported drug use.McNeely , et al. 2015
Full screens
Full screens in the emergency room Typically delivered via interview withbehavioral health specialist When there’s a “break in the action” waiting for x-rays, labs or ready fordischarge Best case scenario: warm handoff Pts may be more receptive to BHS thanmedical clinician and answer morehonestly than in triage
AUDIT Alcohol Use Disorders IdentificationTest Created by WHO, accurate acrossmany cultures/nations 10 questions - multiple choice Addresses alcohol onlyWHO, 2001
Scoring the AUDIT Each question has five answer choices Answers correlate with points, totaled for score
Suggested AUDIT zones and scores
Circling the zone of use
Case study: Clark 68yo male, never married, retired,lives alone Mild hypertension and diabetessince 2017, not obese Presents twice a year for follow up,usually no medical complaints Latest visit: discloses drinking 10beers a night at local bar
ExerciseTake a minute to fill out an AUDIT, circling whatyou think might be Clark’s responses.
Clark’s (real) AUDIT answers:Questions0123Monthly 2-4 times 2-3 timesor lessa month a week1. How often do you have a drink containing alcohol?Never2. How many drinks do you have on a typical day when drinking?1 or 23 or 45 or 67 to 93. How often do you have six or more drinks on one occasion?NeverLess thanmonthlyMonthlyWeeklyNeverLess thanmonthlyMonthlyWeeklyNeverLess thanmonthlyMonthlyWeeklyNeverLess thanmonthlyMonthlyWeeklyNeverLess thanmonthlyMonthlyWeeklyNeverLess thanmonthlyMonthlyWeekly4. How often during the last year have you found that you were notable to stop drinking once you had started?5. How often during the last year have you failed to do what wasnormally expected of you because of drinking?6. How often during the last year have you needed a first drink in themorning to get yourself going after a heavy drinking session?7. How often during the last year have you had a feeling of guilt orremorse after drinking?8. How often during the last year have you been unable to rememberwhat happened the night before because of your drinking?9. Have you or someone else been injured because of your drinking?No10. Has a relative, friend, doctor, or other health care worker beenconcerned about your drinking or suggested you cut down?NoYes, butnot in thelast yearYes, butnot in thelast year44 or moretimes aweek10 ormoreDaily oralmostdailyDaily oralmostdailyDaily oralmostdailyDaily oralmostdailyDaily oralmostdailyDaily oralmostdailyYes, duringthe lastyearYes, duringthe lastyear
Clark’s AUDIT score: 15
Full screen: DAST Drug Abuse Screening Test DAST-10 version Validated for adults Cut-off score of 3 has highvalidity for drug “abuse”Skinner, 1982.Yudko 2007.
Scoring the DAST Each question has yes or no answer Yes answers get one point
DAST zones and scoresSevereHarmfulRiskyIVIIIIII6 3-51-2
Circling the zone of use
Questions added to the DAST Types of drugs used Frequency of use Injection drug use Status of drug treatmentwww.sbirtoregon.org
DAST and CannabisBrief intervention may not be necessarywhen: No daily use of any substance No weekly use of opioids, cocaine, ormeth No injection drug use in the past 3months. Not currently in treatment.
Case study: Stacey 30yo female, single, works atrestaurant, lives with housemate Takes Aderall for ADHD past twoyears Presents every few months for inperson follow up, usually no medicalcomplaints. Uses a “bump” of cocaine mostweekends
Exercise:Take a minute to fill out a DAST, circlingwhat you think might be Stacey’sresponses.
xxxxStacey’spossibleDASTanswers
CRAFFT screening tool Validated for ages 12 – 21 Widely implemented Self administered or delivered viainterview Number of “Yes” answerscorrelate with SUD
CRAFFT questions #1 - 4 John R. Knight, MD, Boston Children’s Hospital
CRAFFT questions #5 - 10 John R. Knight, MD, Boston Children’s Hospital
Interpreting the CRAFFTAnswersRiskAction“No” to questions 1-4No riskPositive reinforcement“Yes” to Car questionRiding riskDiscuss alternatives to riding with impaireddrivers (Contract for Life)CRAFFT score 0Low riskBrief adviceCRAFFT score 1Medium riskBrief interventionCRAFFT score 2High riskBrief intervention(offer options that include treatment)
CAR question Car accidents leading cause of accidentaldeath among teens Study: 17% of students report having riddenin a vehicle in the last 30 days driven bysomeone who had been drinking alcohol Discuss safer alternatives Option: Ask teen to take home the“Contract For Life” to discuss with parent(s)or adult. Offer to facilitate conversation.CDC, 2018
5Ps tool Designed for patients who arepregnant Asks about use by Parents, Peers,Partner, pt’s Past, and during pt’sPregnancy Also screens for tobacco, emotionalhealth, and intimate partner violence. Administered through interview
Other screening tools CAGE: poor sensitivity for riskydrinking ASSIST: covers alcohol as well as druguse, but too complex for manysettings MAST: poor sensitivity for riskydrinking; long; outdated terminology
Screening via patient portalPros: Can be completed before visit Questions answered withoutconversation with clinicianCons: Results may get lost in EHR Can’t ensure pt privacy Proxy accounts for younger teens breakconfidentiality
Screening via online interviewPros: Can clarify questions in real timeResults entered in EHR immediatelyAn opportunity to build rapport, setthe stage for BICons: Takes up time during visit Pt has to answer questions directly toclinician
Tips on screening via online interview Try to confirm that pt is in privatespace and can't be overheard Can be done during any portion ofthe visit Explain reason behind screening Raise the subject and ask permission Read validated questions as written
III. Reimbursement and EHR tools
Screening-only billing CPT96160G0442DescriptionAdministration and interpretationof a health risk assessmentinstrument.Screening for alcohol misuse inadults once per year. Codes above should be appended to E/M service with modifier 25 ICD-10 diagnosis codes are poorly suited for most SBIRT patient scenarios and can break confidentiality. Twooptions: Z13.89: “Encounter for screening for other disorder” Z13.9: “Encounter for screening, unspecified”
Screening BI codesServicePayerCodeDescriptionMedicareG2011 5-14 minutes of aggregate clinic time spentadministrating and interpreting a validatedalcohol or drug screening tool, plus performing aface-to-face brief intervention the same day. MedicaidCPT 99408briefinterventionMedicareG0396MedicaidCPT 99409Full screen Same as above, 15 – 29 minutes. Same as above, 30 minutes.MedicareG0397 Codes above should be appended to E/M service with modifier 25 ICD-10 diagnosis codes are poorly suited for most SBIRT patient scenarios and can break confidentiality. Twooptions: Z13.89: “Encounter for screening for other disorder” Z13.9: “Encounter for screening, unspecified”
Documentation supporting screening-onlywith adult pts (CPT 96160)www.sbirtoregon.org
Documentation supportingscreening-only with adolescent pts (CPT 96160)www.sbirtoregon.org
Documentation supporting SBI with adultswww.sbirtoregon.org
Documentation supporting SBI with adolescentswww.sbirtoregon.org
Who’s allowed to independentlybill for SBIOregon MedicaidMedicarePhysicians (MD, DO, ND)Physicians (MD, DO)Physician AssistantsPhysician AssistantsNurse PracticionersNurse PracticionersLicensed Clinical PsychologistsLicensed Clinical PsychologistsLicesned Clinical Social WorkersLicesned Clinical Social WorkersLicensed Professional CounselorsCertified Nurse MidwivesLicensed Marriage and Family TherapistsClinical Nurse Specialists
Incident-to billingAny clinic employee under supervisioncan bill for SBI. Examples:–CADCs, Health Educators, RegisteredNurses, Clinical Nurse Specialist,Students or Graduates enteringmedical profession, Community HealthWorkers–Some limitations apply to certain clinicsettingsOHA, 2014
Oregon CCO metric: SBIRTRATE 1:Patients with either a negativebrief screen or a full screen.Pts 12 years visit in last yearRATE 2:Pts who received a brief intervention, orreferral to treatment within 48 hoursPts with a positive full screen.OHA
Oregon CCO metric: IETInitiation and Engagement of Alcohol and Other Drug Abuse orDependence TreatmentInitiation rate:Engagement rate:Pts who received AODTreatment within 14 daysPts who received 1 or 2 AOD treatmentswithin 34 days of initiating treatmentPts 13 years with a new AOD dxPts 13 years with a new AOD dxA brief intervention with a BHS counts as satisfying the numerator in both ratesOHA
IV. Brief intervention
Large brief intervention study Study question: is BI associated withtreatment for AUD? Analysis of VA pt records 2009-2013 830,825 outpatients screened positive forunhealthy alcohol use, 74% haddocumented BI within 0-14 days Result: BI was associated with lowerlikelihood of receiving specialty treatmentFrost MC, Glass JE, Bradley KA, Williams EC. “Documented brief intervention associated with reduced linkage to specialty addictions treatment in a national sample of VA patients withunhealthy alcohol use with and without alcohol use disorders”. Addiction. 2019 Oct 22.
Table: Percent of VA pts who received treatment within 365 daysAdjusted*%95%CIRateratioP-value.84 0.001.83 0.001Overall sample: (N 1,172,606 positive screens)No documented BI12.6(12.5-12.7)Documented BI10.5(10.4-10.6)AUD diagnosis in the past year: (N 421,244 positive screens)No documented BI19.9(19.7-20.1)Documented BI16.5(16.4-16.6)*“Adjusted for sex, age, race/ethnicity, marital status, VA eligibility status, mental health and drug use disorderdiagnoses, tobacco use, AUDIT-C category, alcohol use disorder diagnosis, alcohol-specific condition, and fiscal yearin which positive AUDIT-C screen occurred.”Frost, et al. Addiction. 2019
Study takeaways BIs in the VA were defined asonly giving information andadvice Conclusion: poor BIs may causeharm with pts with SUDs. The quality of the BI matters!Frost, et al. Addiction. 2019
How do you discuss behaviorchange with your patients?
Video:The Ineffective Clinicianhttps://www.youtube.com/watch?v cSBsgmgYm8oUniversity of Florida, Psychiatry Dept.
Characteristics of a directive style ofcommunicationRollnick and Miller, 2008
Common patient reactions to thedirective pless, overwhelmedAshamedTrappedDefensiveJustifyingNot understoodDisengagedNot come back – avoidUncomfortableProcrastinateNot heardRollnick and Miller, 2008
Characteristics of a guidingstyle of communication Respect for patient’s autonomy,own goals, values Gauge readiness to change Comfort with ambivalence Recognize pts expertise Empathy, non-judgment, respect
Some reasons people use substancesEscape from griefEscape from stressPeer pressureTo fit inTo experimentTo relaxTo deal with boredomNot ready to quitAvoid withdrawalEnjoyment of feeling highEscape fromnegative thoughtsEnhanceperformanceCareer pressuresEscape feelings oflonelinessFeeling of controlInstant gratificationFamilydemands
Brief Interventions in medical settings Should employ motivationalinterviewing (evidence-based) Even three minutes can haveeffect Can be performed by any trainedclinic employee 2 hours of training can makedifferenceHumeniuk et al, 2010. Cunningham et al, 2014. Whitlock et al, 2004.
Textbook definition ofmotivational interviewingA person-centered counseling style foraddressing the common problem ofambivalence about change.-Miller and Rollnick, 2012.
Two central goals of MI “To create and amplify, from the client’sperspective, a discrepancy betweenpresent behavior and broader goals andvalues.” “To evoke statements indicating reasons for,desire to, or intent to change (changetalk)”Lozano, et al, 2010
How MI works Eliciting and affirming change talk helpspts move towards resolving ambivalence People become more committedtowards change when they hearthemselves give voice to change Respect, collaboration and empathycreate conditions for change to occur
Motivational interviewing towardsother health behaviorsMorton, et al, 2015.
Warm introduction principles In-person introduction tobehavioral health specialist Refer to as “colleague” or“specialist” Brief intervention deliveredduring same visit Avoid “counseling” label
Steps of the brief ivationIdentifyplan
Steps of the brief intervention Ask permission to discuss patient’sRaisesubjectsubstance use Convey transparency about yourrole
Transparency exampleThank you for giving me permission to discuss your substance usewith you. Just so you know, I will not ask or advise you to stop orchange your use in any way you do not want to. Instead, myfocus is to understand what your goals or visions for your futureare. I can share information with you so you can improve yourquality of life on your own terms and on your own timeline.How does that sound to you?HaRRT Center
Steps of the brief intervention Ask permission to discuss patient’sRaisesubjectsubstance use Convey transparency about yourrole Ask the patient to describe theiruse
Steps of the brief interventionShare info about:Shareinformation The pt’s score on the screening tool Any association between use andhealth complaint General risks of useAsk pt what they think about theinformation shared
Pitfalls of giving advice or recommendations Implies judgement, risks furthering stigma Clinician-driven rather than patient-driven Patients with SUDs may already feeltrapped Giving advice is different thanbrainstorming options
Steps of the brief intervention Elicit and summarize pros and consEnhancemotivation- What pt likes and doesn’t like about their use
Pros and cons example“So on one hand, I hear you say that your cannabis use makesyou feel relaxed after a day of work, and it reduces your anxietyin the short term. On the other hand, you wonder sometimes ifyou’re becoming addicted to cannabis, and you don’t like itwhen your partner nags you about smoking pot. Is that correct?”HaRRT Center
Steps of the brief intervention Elicit and summarize pros and consEnhancemotivation- What pt likes and doesn’t like about their use Elicit goal(s)- What change the pt would like to see
Questions that elicit patient goals “Over the next few (weeks, months)what would you like to see happen foryourself?” “What would you like to do about youruse?” “Where would you like to go with yourdrinking/drug use?”
Goals are more achievable when they are: Well defined Focused on reducing harmor improving quality of life Doable in a timeframe Patient-drivenHaRRT Center
Helping pts with abstract, or large goalsPatient: “I want to livehealthier.”?Livinghealthier?Clinician: “That’s a great goal. It’s also a big goal. So, let’s put thatup here on the top step. What could be the first step towards livinghealthier?”Slide: HaRRT Center
Some examples of pt-driven goals: alcohol Reducing or abstaining Counting drinks Eating before drinking, and during Spacing drinks Accepting meds for AUD or other treatment Avoid mixing drugs with alcohol Drinking in a safe place Choosing periodic abstinence Choosing lower-alcohol content beverages
Some examples of pt-driven goals: drugs Injecting more safely Minimizing sharing works orneedles Carrying Naloxone Using less Accept MOUD or other treatment Learning abscess care Getting more regular medicalcare and/or mental health care
Steps of the brief intervention Elicit and summarize pros and cons- What pt likes and doesn’t like about their useEnhancemotivation Elicit goal(s)- What change the pt would like to see Gauge readiness/confidence to achievegoal- Use readiness ruler
Readiness Ruler “On a scale of 0 to 10 . . .” “Why not a lower number?” Gauges level of motivation Answering the question enhanceexisting motivation
Steps of the brief intervention If patient sounds ready, ask: “WhatIdentifyplanwould a plan of reaching your goallook like for you?” Affirm pt’s readiness to change Ask to schedule follow-up
Follow upA continuing cycle of: Collaborative tracking of patientselected goals Sharing information about risks Eliciting new pt-driven harmreduction goalsHaRRT Center
Remember:Defer to thepatient’s wisdomThe more responsibility, autonomy andrespect people feel they have, the more theywill step up and forge their own pathway.HaRRT Center
Raise thesubject “Thanks for filling out this form – is it okay if we briefly talk about your substance use?” “My role is to help you assess the risks so you can make your own decisions. I want to help youimprove your quality of life on your own timeline.” “What can you tell me about your substance use?”Shareinformation Explain any association between the patient’s use and their health complaint, then ask, “Do youthink your use has anything to do with your [anxiety, insomnia,, etc,]?” Share information about the risks of using alcohol, drugs, and misusing prescription drugs. Askthe patient: “What do you think of this information?”Enhancemotivation Ask pt about perceived pros and cons of their use, then summarize what you heard. “Where do you want to go from here in terms of your use? What’s your goal or vision? Gauge patient’s readiness/confidence to reach their goal. If using Readiness Ruler: “Why do didyou pick on a scale of 0-10 instead of [lower number]?”Identifyplan If patient is ready, ask: “What steps do you think you can take to reach your goal?” Affirm the patient’s readiness/confidence to meet their goal and affirm their plan. “Can we schedule an appointment to check in and see how your plan is going?”
Adultreferencesheet(front & back)Available atsbirtoregon.org
Adolescentreferencesheet(front & back)Available atsbirtoregon.org
Pregnancyreferencesheet(Front & back)Available atsbirtoregon.org
Patient handouts Download at sbirtoregon.org English and Spanish Separate handouts based onsubstance and population Should reinforce, not replacebrief interventionswww.sbirtoregon.org
Case study: “Barbara” 60-year old female visiting anew PCP to discuss her antidepression meds Drinks 4x a week, 3-4 glassesof wine per occasion Lives alone Completed the AUDIT andscored 14
Video demonstration: “Barbara”
Case study: “Miguel” 35-year old presenting for atelehealth visit Complains of migraines Injects heroin 2-3 days perweek Completed the DAST andscored 4
Practice: “Miguel”Groups of three: Clinician Patient Observer
Video demonstration: “Miguel”
Case study: “Natasha” 16-year old presenting for aphys
Adult limits for alcohol use, U.S. Moderate drinking Binge drinking Women No more than 1 drink per day 4 drinks per occasion Men No more than 2 drinks per day 5 drinks per occasion Daily limits are "not intended as an average over several days, but rather the amount consumed on any single day." Standard drink in the U.S. defined as: