Transcription
Introduction and MethodologyThis literature review is a refinement of the initial review and is an examination of the evidencebase for remote telemonitoring and therefore the emphasis has been on identifying key researchfrom the top levels of the evidence hierarchy as defined by the School of Health and RelatedResearch at the University of Sheffield. “The higher up a methodology is ranked, the more robustand closer to objective truth it is assumed to be” (ScHARR). The aim of the literature search was toidentify relevant systematic reviews and randomised controlled trials.Rank Methodology1Systematic reviews and meta-analyses2Randomised controlled trials3Cohort studies4Case-control studies5Cross sectional surveys6Case reports7Expert opinion8AnecdotalTable 1: Hierarchy of Evidence (ScHARR)A Systematic Review is a method of looking at a number of primary studies which have beenidentified in a review of the literature according to specific search criteria. Inclusion and exclusioncriteria have been set and the identified studies have been evaluated against consistentmethodological standards.A randomised controlled trial (RCT) is a trial where the patients / participants are randomlyallocated to an arm of the trial, the two arms being the intervention group and the placebo or usualcare group. Those trials which look at an intervention group and a placebo group but the patients1
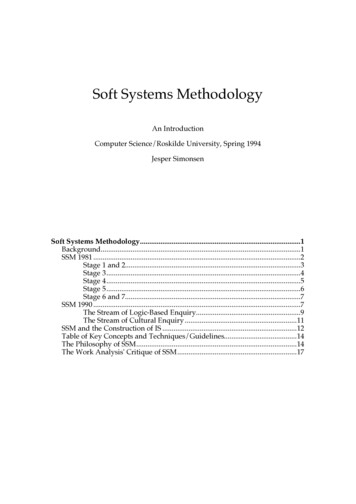
have not been randomly allocated are called non randomised controlled trials and can also beknown as other controlled clinical trials.The methodological approach for the literature search is illustrated in figure 1 and the details ofnumber of articles retrieved are given in table 2.PubMed was searched individually for each of the main clinical conditions of interest. Each searchwas run as a MeSH Major Topic in an attempt to ensure the condition was a major element ofinterest in the identified articles. Each of the individual searches for the clinical conditions wascombined into a single result set using the Boolean “OR”.A separate PubMed search was undertaken to address the concept of remote telemonitoring. Theterms included in this search were an attempt to be as inclusive as possible at this stage.The result set for the concept of chronic disease (heart failure, diabetes mellitus and COPD) wascombined with the result set for the concept of remote telemonitoring using the Boolean “AND”operator.Table 2: PubMed Search Terms and Number of Articles Retrieved.SearchNumberSearch Term#1"Heart Failure"[MeSH Major Topic]#2"Diabetes Mellitus"[MeSH Major Topic]#3"Pulmonary Disease, ChronicNumber ofarticles returned4330117873716632Obstructive"[MeSH Major Topic]#4#1 OR #2 OR #3237985#5telemedicine OR telecare OR telehealth OR11135telemonitoring OR "home monitoring" OR"remote monitoring"#6#4 AND #5495#7#6 Limits: only items with abstracts, Humans,154Clinical Trial, Meta-Analysis, RandomizedControlled Trial, Review, Controlled ClinicalTrial, English2
Figure 1: Search methodologyThe 495 articles returned from the original combined PubMed search were reduced to 154 byapplying several limits. The result set was restricted to those articles that included an abstract, were3
in the English language and covered human subjects. Additionally only articles of the followingtypes were included: clinical trial, meta-analysis, RCT, review and controlled clinical trial.A further 8 articles were identified by hand searching the following journals: The Journal of Telemedicine and Telecare Telemedicine and e-HealthAbstracts for 162 articles were examined, leading to the exclusion of 103 articles. Articles wereexcluded from the review if: Remote monitoring was not the main focus of the article There was no central element of monitoring in relation to remotely collected data Remote monitoring consisted of telephone support only The article focused on paediatrics or conditions other than heart failure, diabetes mellitus orCOPD.59 articles were studied in detail. 15 of these publications were excluded from the review because itbecame apparent on detailed study that they met the exclusion criteria.44 publications are included in the review.4
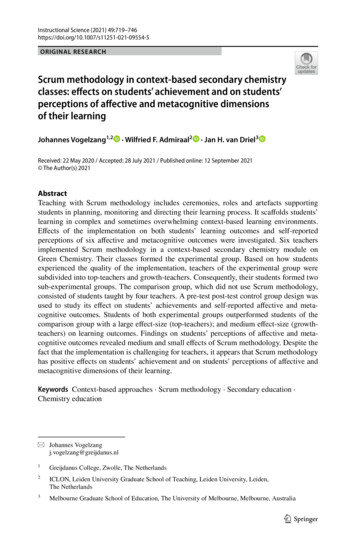
Literature ReviewRCT Checklist: Albisser (1996)Checklist Methodology is copyright Scottish Intercollegiate Guidelines Network, March 2004Methodology Checklist: Randomised Controlled TrialsStudy identification (Include author, title, year of publication, journal title, pages)AuthorAlbisser, A.M., et al.Title“Diabetes intervention in the information age.”ReferenceMed Inform (Lond), 1996. 21(4): p. 297-316.Section 1: Internal validityIn a well conducted RCT study:In this study this criterion is:1.1Adequately addressedThe study addresses an appropriate and clearlyfocused question.1.2The assignment of subjects to treatment groups isNot addressedrandomised1.3An adequate concealment method is usedNot addressed1.4Subjects and investigators are kept ‘blind’ aboutNot applicabletreatment allocation1.5The treatment and control groups are similar atNot addressedthe start of the trial1.6The only difference between groups is theNot addressedtreatment under investigation1.7Poorly addressedAll relevant outcomes are measured in astandard, valid and reliable way1.8What percentage of the individuals or clustersNot clearly addressedrecruited into each treatment arm of the study5
dropped out before the study was completed?1.9Poorly addressedAll the subjects are analysed in the groups towhich they were randomly allocated (oftenreferred to as intention to treat analysis)1.10Where the study is carried out at more than onePoorly addressedsite, results are comparable for all sitesSection 2: Overall assessment of the study2.1How well was the study done to minimise bias?(-) no indication givenCode , , or 2.22.3If coded as , or what is the likely direction inNo description of inclusionwhich bias might affect the study results?criteria for patientsTaking into account clinical considerations, yourEffect shown is due to theevaluation of the methodology used, and theintervention.statistical power of the study, are you certain thatthe overall effect is due to the study intervention?Section 3: Description of the study3.1How many patients are included in this study?Please indicate number in each arm of the study,117 recruited from healthmaintenance organisation.87 recruited from privateat the time the study began.practice office.3.2What are the main characteristics of the patientCharacteristics of the patientspopulation?were not specifically described– entrants were unrestricted inInclude all relevant characteristics – e.g. age,sex, ethnic origin, comorbidity, disease status,relation to age, gender, socioeconomic class, type ofcommunity/hospital baseddiabetes, method of treatment,type of medication and method ofglucose self management.3.3What intervention (treatment, procedure) is beingIntervention is the use of aninvestigated in this study?electronic information system tofacilitate control of blood6
glucose and evaluating if theList all interventions covered by the study.system is safe to use and/oreffective.3.4Comparisons are made by lookingWhat comparisons are made in the study?Are comparisons made between treatments, orbetween treatment and placebo / no treatment?at the blood glucose control ofthose patients using theelectronic system and thosepatients who are not using thesystem.3.5How long are patients followed-up in the study?Patients followed up for 1 year.Length of time patients are followed frombeginning participation in the study. Notespecified end points used to decide end of followup (e.g. death, complete cure). Note if follow-upperiod is shorter than originally planned.3.6What outcome measure(s) are used in the study?Systems utilization statistics.List all outcomes that are used to assessBenefits to patients accordingeffectiveness of the interventions used.to metabolic outcomes, glycatedhaemoglobin and body weight.3.7Glycated haemoglobin (glycatedWhat size of effect is identified in the study?List all measures of effect in the units used in thestudy – e.g. absolute or relative risk, NNT, etc.Hb) fell significantly showing adrop of 1- 1.3%, p 0.01 orp 0.001.Include p values and any confidence intervalsthat are provided.3.8How was this study funded?Not documented.List all sources of funding quoted in the article,whether Government, voluntary sector, orindustry.3.9Does this study help to answer your keyThis study focuses on the safetyquestion?issue of the use of anSummarise the main conclusions of the study andelectronic device to monitor/feedback clinical information onindicate how it relates to the key question.a patients blood glucose leveland thus provide information onhow well a patients condition is7
controlled.It illustrates thatthere are no observeddetrimental effects to patientsusing the system and alsoindicates that due to the factthat up to date information onthe patients blood glucosemeasurements are available, thehealthcare professionals are ina better position to makechanges to the patientstreatment regime with the aim ofimproving the patients diabeticcare.8
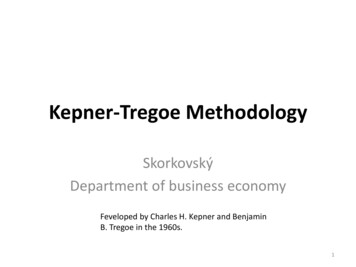
RCT Checklist: Albisser (2007)Checklist Methodology is copyright Scottish Intercollegiate Guidelines Network, March 2004Methodology Checklist: Randomised Controlled TrialsStudy identification (Include author, title, year of publication, journal title, pages)AuthorAlbisser, A.M., C.E. Wright, and S. SakkalTitle“Averting iatrogenic hypoglycemia through glucoseprediction in clinical practice: progress towards a newprocedure in diabetes.”Reference Diabetes Res Clin Pract, 2007. 76(2): p. 207-14.Section 1: Internal validityIn a well conducted RCT study:In this study this criterion is:1.1Well coveredThe study addresses an appropriate and clearlyfocused question.1.2The assignment of subjects to treatment groups isAdequately addressedrandomised1.3An adequate concealment method is usedNot addressed1.4Subjects and investigators are kept ‘blind’ aboutNot addressedtreatment allocation1.5The treatment and control groups are similar atAdequately addressedthe start of the trial1.6Adequately addressedThe only difference between groups is thetreatment under investigation1.7All relevant outcomes are measured in aAdequately addressedstandard, valid and reliable way1.80% drop out rate in both armsWhat percentage of the individuals or clustersrecruited into each treatment arm of the studydropped out before the study was completed?9
1.9Adequately addressedAll the subjects are analysed in the groups towhich they were randomly allocated (oftenreferred to as intention to treat analysis)1.10Where the study is carried out at more than oneNot applicablesite, results are comparable for all sitesSection 2: Overall assessment of the study2.1How well was the study done to minimise bias?( )Code , , or 2.22.3If coded as , or what is the likely direction inUnclear how randomisationwhich bias might affect the study results?carried out.Taking into account clinical considerations, yourEffect due to the intervention.evaluation of the methodology used, and thestatistical power of the study, are you certain thatthe overall effect is due to the study intervention?Section 3: Description of the study3.1How many patients are included in this study?Please indicate number in each arm of the study,study. 11 patients in each armof the study.at the time the study began.3.222 patients included in theWhat are the main characteristics of the patientpopulation?Community based patients.Age range 49.9 to /- 17.6Include all relevant characteristics – e.g. age,years.sex, ethnic origin, comorbidity, disease status,Being intensively treated withcommunity/hospital basedinsulin. 1 episode/wk hypoglycaemia.Willingness to report dailyresults to diabetes center.3.3What intervention (treatment, procedure) is beingUse of telemedicine interventioninvestigated in this study?which would help to avertiatrogenic hypoglycaemiaList all interventions covered by the study.episodes occurring. The remotely10
monitored data is presented on ascreen to the healthcareproviders enabling predictedpending risks of hypoglycaemiato be identified.3.4Patients using the system areWhat comparisons are made in the study?Are comparisons made between treatments, orbetween treatment and placebo / no treatment?compared with those patients whodo not have access to the systemwith regard to the number ofhypoglycaemic episodes.3.5How long are patients followed-up in the study?2 months.Length of time patients are followed frombeginning participation in the study. Notespecified end points used to decide end of followup (e.g. death, complete cure). Note if follow-upperiod is shorter than originally planned.3.6What outcome measure(s) are used in the study?Primary outcome – Frequency ofhypoglycaemic episodes.List all outcomes that are used to assessSecondary outcomes includeeffectiveness of the interventions used.premeal blood glucose,medication dosages taken andglycated HbA1c.3.7Hypoglycaemia episodes 0.2 /-What size of effect is identified in the study?List all measures of effect in the units used in thestudy – e.g. absolute or relative risk, NNT, etc.Include p values and any confidence intervals0.3 (0to 1) in the interventiongroup and 2.0 /- 0.9 (1-3) inthe control group.that are provided.3.8Not clearly documented.How was this study funded?List all sources of funding quoted in the article,whether Government, voluntary sector, orindustry.3.9Does this study help to answer your keyThis study’s findings indicatequestion?that the more information madeSummarise the main conclusions of the study andavailable to the clinicians withregard to the patients blood11
glucose readings, the better theindicate how it relates to the key question.predictive control ofhypoglycaemia episodes inpatients is achieved. Theclinicians are in a betterposition to advise on treatmentoptions and changes required tothe patients treatment regime.The authors in this study haveshown that this effect can beachieved in 2 months but thenumbers involved in this studyare very small.12
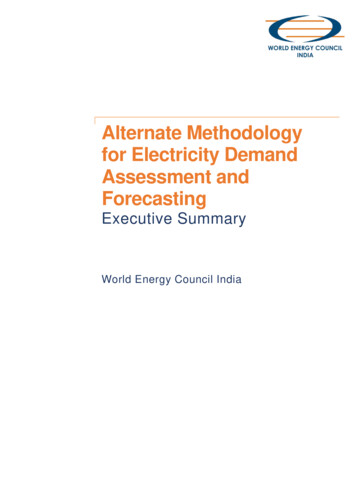
Systematic Review Checklist: Barlow (2007)Checklist Methodology is copyright Scottish Intercollegiate Guidelines Network, March 2004Methodology Checklist: Systematic Reviews and Meta-analysesStudy identification (Include author, title, year of publication, journal title, pages)AuthorBarlow, J., et al.Title“A systematic review of the benefits of home telecare forfrail elderly people and those with long-termconditions.”Reference J Telemed Telecare, 2007. 13(4): p. 172-9.Section 1: Internal validityIn a well conducted systematic review:In this study this criterion is:1.1Adequately addressedThe study addresses an appropriate and clearlyfocused question.1.2Well coveredA description of the methodology used isincluded.1.3The literature search is sufficiently rigorous toWell coveredidentify all the relevant studies.1.4Study quality is assessed and taken into account.Poorly addressed1.5There are enough similarities between the studiesAdequately addressedselected to make combining them reasonable.Section 2: Overall assessment of the study2.1How well was the study done to minimise bias?Code , , or 2.2If coded as , or what is the likely direction inwhich bias might affect the study results?13( )
Section 3: Description of the study3.1What types of study are included in the review?RCT, Cohort, Case-control3.2How does this review help to answer your keyThe main outcomes of thisquestion?systematic review looked at vitalSummarise the main conclusions of the reviewand how it relates to the relevant key question.sign monitoring and its benefitsto individuals and system widebenefits. Looking at theComment on any particular strengths orweaknesses of the review as a source of evidencefor a guideline produced for the NHS in Scotland.individual benefits the authorsidentified 18 RCTs and 1 largeobservational study and fromthese papers they found that thelargest amount of evidence forthe use of home telecare inelderly people with long termconditions was available in theclinical areas of diabetes andheart failure with less evidencebeing available for COPD. ForDiabetes 5 of the aforementionedstudies showed no significantdifference in clinical outcomesoccurring from telemonitoring ofblood glucose and another 3studies found significantlyimproved clinical outcomes. Forheart failure improvement inquality of life and reduction inmortality are the main findings.The system benefits shown fromthis review are that the remotetelemonitoring of data is atleast as efficient asconventional care and may evenreduce the use of health servicefor those patients with heartfailure and COPD. No detrimentaleffects on patient care areobserved in this review.14
Cohort Study Checklist: Barnett (2007)Checklist Methodology is copyright Scottish Intercollegiate Guidelines Network, March 2004Methodology Checklist: Cohort studiesStudy identification (Include author, title, year of publication, journal title, pages)AuthorBarnett, T.E., et al.Title“The cost-utility of a care coordination/home telehealthprogramme for veterans with diabetes.”ReferenceJ Telemed Telecare, 2007. 13(6): p. 318-21.Section 1: Internal validityIn a well conducted cohort study:In this study the criterion is:1.1Adequately addressedThe study addresses an appropriate and clearlyfocused question.SELECTION OF SUBJECTS1.2The two groups being studied are selected fromWell coveredsource populations that are comparable in allrespects other than the factor underinvestigation.1.3Not addressedThe study indicates how many of the peopleasked to take part did so, in each of the groupsbeing studied.1.4The likelihood that some eligible subjects mightNot addressedhave the outcome at the time of enrolment isassessed and taken into account in the analysis.1.5What percentage of individuals or clustersNot addressed – made knownrecruited into each arm of the study dropped outbefore the study was completed.1.6Comparison is made between full participantsand those lost to follow up, by exposure status.15Not addressed
ASSESSMENT1.7The outcomes are clearly defined.Adequately addressed1.8The assessment of outcome is made blind toPoorly addressedexposure status.1.9Where blinding was not possible, there is somePoorly addressedrecognition that knowledge of exposure statuscould have influenced the assessment ofoutcome.1.10Poorly addressedThe measure of assessment of exposure isreliable.1.11Poorly addressedEvidence from other sources is used todemonstrate that the method of outcomeassessment is valid and reliable.1.12Exposure level or prognostic factor is assessedPoorly addressedmore than once.CONFOUNDING1.13The main potential confounders are identifiedPoorly addressedand taken into account in the design andanalysis.STATISTICAL ANALYSIS1.14NoHave confidence intervals been provided?Section 2: Overall assessment of the study2.1How well was the study done to minimise the(-)risk of bias or confounding, and to establish acausal relationship between exposure and effect?Code , , or 2.2Taking into account clinical considerations, yourevaluation of the methodology used, and thestatistical power of the study, are you certain16Unclear
that the overall effect is due to the exposurebeing investigated?Section 3: Description of the study3.1How many patients are included in this study?370- site A 60, site B 56,List the number in each group separatelySite C 165, site D 89(reference group).3.2What are the main characteristics of the studyVeterans with diabetes, 2 or morepopulation?hospital admissions or emergencydepartment visits in the 12Include all relevant characteristics – e.g. age,sex, ethnic origin, comorbidity, disease status,months prior to enrolment, 10medication prescriptions, averagecommunity/hospital basedage68.2, male(365),Hispanic(175), white(154),black/other(41).3.3What environmental or prognostic factor is beingThe cost effectiveness of careinvestigated in this study?co ordination hometelehealth(CCHT) usingincremental cost effectivenessratios(ICERs).3.4Cost effectiveness of care for aWhat comparisons are made in the study?cohort of veterans was comparedAre comparisons made between presence orabsence of an environmental / prognostic factor,a CCHT programme of care.or different levels of the factor?3.5pre and post the introduction of12 months.For how long are patients followed-up in thestudy?3.6What outcome measure(s) are used in the study?Cost effectiveness of the careprovided measured using ICERsList all outcomes that are used to assess theimpact of the chosen environmental or prognosticcalculated by converting thepatients health related qualityfactor.of life data into qualityadjusted life year(QALY) scoresand then using costs to constructincremental cost effectivenessratios(ICERs).17
3.7The CCHT programme is shown to beWhat size of effect is identified in the study?List all measures of effect in the units used in thestudy – e.g. absolute or relative risk. Include pcost effective for at least 1/3of the veterans in the study.values and any confidence intervals that areprovided. Note: Be sure to include anyadjustments made for confounding factors,differences in prevalence, etc.3.8Funded by a contract from the VAHow was this study funded?List all sources of funding quoted in the article,VISN-8 Community CareCoordination Service.whether Government, voluntary sector, orindustry.3.9Does this study help to answer your keyThis study focuses on thequestion?analysis of the quality of lifeSummarise the main conclusions of the study andscores in order to help addresscost effectiveness of theindicate how it relates to the key question?intervention. It does notdescribe the content of the carecoordination home telehealthprogramme thus the authors do notgive enough detail as to whethervital sign monitoring or remotetelemonitoring is part of theCCHT programme.18
RCT Checklist: Benatar (2003)Checklist Methodology is copyright Scottish Intercollegiate Guidelines Network, March 2004Methodology Checklist: Randomised Controlled TrialsStudy identification (Include author, title, year of publication, journal title, pages)AuthorBenatar, D., et al.Title“Outcomes of chronic heart failure.”ReferenceArch Intern Med, 2003. 163(3): p. 347-52.Section 1: Internal validityIn a well conducted RCT study:In this study this criterion is:1.1Well coveredThe study addresses an appropriate and clearlyfocused question.1.2The assignment of subjects to treatment groups isNot addressedrandomised1.3An adequate concealment method is usedNot addressed1.4Subjects and investigators are kept ‘blind’ aboutNot addressedtreatment allocation1.5The treatment and control groups are similar atAdequately addressedthe start of the trial1.6Well coveredThe only difference between groups is thetreatment under investigation1.7All relevant outcomes are measured in a standard,Well coveredvalid and reliable way1.8NoneWhat percentage of the individuals or clustersrecruited into each treatment arm of the studydropped out before the study was completed?19
1.9Adequately addressedAll the subjects are analysed in the groups towhich they were randomly allocated (oftenreferred to as intention to treat analysis)1.10Where the study is carried out at more than oneNot applicablesite, results are comparable for all sitesSection 2: Overall assessment of the study2.1How well was the study done to minimise bias?(-)Code , , or 2.2If coded as , or what is the likely direction inNo indication of randomisationwhich bias might affect the study results?2.3Taking into account clinical considerations, yourEffect due to the intervention.evaluation of the methodology used, and thestatistical power of the study, are you certain thatthe overall effect is due to the study intervention?Section 3: Description of the study3.1How many patients are included in this study?Please indicate number in each arm of the study,216 patients – 108 in each arm ofthe study.at the time the study began.3.2What are the main characteristics of the patientPatients admitted to hospitalpopulation?with heart failure, New Yorkheart association(NYHA) class 3Include all relevant characteristics – e.g. age,sex, ethnic origin, comorbidity, disease status,or 4, conventional heart failuresymptoms, echo evidence of heartcommunity/hospital basedfailure ejection fraction 40%,mean age 62.9 /- 13.2, 63%female,86.1%african American.3.3What intervention (treatment, procedure) is beingThe use of transtelephonic homeinvestigated in this study?monitoring devices to measureweight, blood pressure, heartList all interventions covered by the study.rate and oxygen saturation.20
3.4Nurse telemanagement, with theWhat comparisons are made in the study?Are comparisons made between treatments, orbetween treatment and placebo / no treatment?patient using the transtelephonichome monitoring devices versususual home nurse visits.3.5How long are patients followed-up in the study?3 months post discharge fromhospital.Length of time patients are followed frombeginning participation in the study. Notespecified end points used to decide end of followup (e.g. death, complete cure). Note if follow-upperiod is shorter than originally planned.3.6What outcome measure(s) are used in the study?Heart failure readmissions,length of stay and anxiety,List all outcomes that are used to assessdepression, self efficacy andeffectiveness of the interventions used.quality of life of the patients.3.7What size of effect is identified in the study?Heart failure readmissionsList all measures of effect in the units used in thestudy – e.g. absolute or relative risk, NNT, etc.reduced for nurse telemanagement(13 versus 24) p 0.01, shorterlength of stay for nurseInclude p values and any confidence intervalstelemanagement patients (49.5that are provided.versus 105 days) p 0.01,meanhospital anxiety and depressionscore decreased in the nursetelemanagement group from 18.89to 12.53 ( p .11) compared with adecrease from 17.69 to 15.52 inthe nurse home visit group(p .046), mean quality of lifescore increased from 16.65 to20.93 (p .01) in thetelemanagement group andincreased from 15.06 to 18.34 inthe visit group ( p .01).3.8Study funded by grants from theHow was this study funded?List all sources of funding quoted in the article,National Institutes of Health,Bethesda, Md.whether Government, voluntary sector, orindustry.21
3.9Does this study help to answer your keyThe findings from this study showquestion?that the use of remoteSummarise the main conclusions of the study andtelemonitoring has a positiveimpact on the readmission ratesindicate how it relates to the key question.of patients with heart failure,decreasing this rate and alsoshows a decrease in the length ofstay required by a patient whomay be readmitted. The samplesize used in this study is areasonable size.22
Systematic Review Checklist: Bensink (2006)Checklist Methodology is copyright Scottish Intercollegiate Guidelines Network, March 2004Methodology Checklist: Systematic Reviews and Meta-analysesStudy identification (Include author, title, year of publication, journal title, pages)AuthorBensink, M., D. Hailey, and R. WoottonTitle“A systematic review of successes and failures in hometelehealth: preliminary results.”Reference J Telemed Telecare, 2006. 12 Suppl 3: p. 8-16.Section 1: Internal validityIn a well conducted systematic review:In this study this criterion is:1.1Well coveredThe study addresses an appropriate and clearlyfocused question.1.2A description of the methodology used isWell coveredincluded.1.3The literature search is sufficiently rigorous toWell coveredidentify all the relevant studies.1.4Study quality is assessed and taken into account.Adequately addressed1.5There are enough similarities between the studiesAdequately addressedselected to make combining them reasonable.Section 2: Overall assessment of the study2.1How well was the study done to minimise bias?Code , , or 2.2If coded as , or what is the likely direction inwhich bias might affect the study results?Section 3: Description of the study23( )
3.1What types of study are included in the review?RCT, CCT, Cohort, Case-control3.2How does this review help to answer your keyThis systematic review looks at aquestion?number of different conditions inSummarise the main conclusions of the reviewand how it relates to the relevant key question.which the use of remotetelemonitoring has been used. Theauthors state that the body ofComment on any particular strengths orweaknesses of the review as a source of evidencefor a guideline produced for the NHS in Scotland.evidence for the use of remotetelemonitoring is growing andthat more, larger scale RCT’s arerequired. This paper is thepreliminary findings of theauthors. It indicates thatconditions most commonly lookedat in relation to the use ofremote telemonitoring includediabetes, heart failure, heartdisease and to a lesser extentchronic lung disease.24
Systematic Review Checklist: Bensink (2007)Checklist Methodology is copyright Scottish Intercollegiate Guidelines Network, March 2004Methodology Checklist: Systematic Reviews and Meta-analysesStudy identification (Include author, title, year of publication, journal title, pages)AuthorBensink, M., D. Hailey, and R. WoottonTitle“A systematic review of successes and failures in hometelehealth. Part 2: Final quality rating results.”Reference J Telemed Telecare, 2007. 13 Suppl 3: p. 10-14.Section 1: Internal validityIn a well conducted systematic review:In this study this criterion is:1.1Well coveredThe study addresses an appropriate and clearlyfocused question.1.2A description of the methodology used isWell coveredincluded.1.3The literature search is sufficiently rigorous toWell coveredidentify all the relevant studies.1.4Study quality is assessed and taken into account.Well covered1.5There are enough similarities between the studiesWell coveredselected to make combining them reasonable.Sectio
types were included: clinical trial, meta-analysis, RCT, review and controlled clinical trial. A further 8 articles were identified by hand searching the following journals: The Journal of Telemedicine and Telecare Telemedicine and e-Health Abstracts for 162 articles were examined, leading to the exclusion of 103 articles. Articles were