Transcription
Health ProgramsSingle-campus Discussion GroupPage 1 of 40HEALTH ACADEMIC PROGRAMSUHCC Single-Campus Discussion, Kapiʻolani Community CollegePhase I ReportNovember 9, 2020The ProcessThe following health academic program faculty met on October 19, 2020. Before the meeting, thefacilitator provided faculty with Guiding Questions, Deliverables, and Main Concepts. Eachprogram was to discuss with their respective program faculty and provide a written response byOctober 19. Each Program Director shared their response during the meeting. The other programfaculty and the facilitator asked questions about their response. Each program then updated theirresponse based on feedback from the group.FacultyFacultyMemberTitleE-mail AddressEmergencyMedicalTech (EMT)JeffreyZuckernickEMT Program CoordinatorEMS Department Chairzuckerni@hawaii.eduMobileIntensiveCare Tech(MICT)LeaugeayBarnesMICT Program Directorlcbarnes@hawaii.eduEMT &MICTMarkKunimuneEMT & MICT Clinical Coordinatormarkkuni@hawaii.eduOccupational TherapyAssistant(OTA)Jaynee MeyerOTA Program Director(resignation waguchiOTA Fieldwork Coordinator (unable toattend the 1st nt(PTA)BennettZazzeraPTA Program Directorbzazzera@hawaii.eduPTAMichelle DelaCruzPTA Clinical D)Kimberly SuwaRAD Program Directorsuwak@hawaii.eduProgram
Health ProgramsSingle-campus Discussion GroupPage 2 of 40RADJodi NakaokaRAD Clinical itioner(RESP)Robert VegaRESP Program Directorrobertlv@hawaii.eduRESPJung Eun KimRESP Clinical Coordinator(unable to attend the 1st meeting)jungeun@hawaii.eduFacilitatorLisa RadakDean, Health Academic Programslradak@hawaii.eduDiscussionOBJECTIVES1. Find and prioritize potential solutions in response to VP Erika Lacro’s 10/12 memo.2. To support the development of faculty recommendations for repositioning UHCCacademic programs for FY22 and beyond (in time to prepare for planning that may requirecurricular changes that need approval in the fall).3. The Facilitoar will send a Recommendation Memo will be sent to VP Erika Lacro on11/9/2020.GUIDING QUESTIONS1. N/A2. To what extent are low enrolled programs or programs with low counts of graduates (lessthan ten graduates as a 3-year average) meeting workforce needs or meeting criticalgeneral education requirements? Some potential solutions:a. If workforce need is at the certificate level (not associates), convert to non-creditprogram with articulation agreement or PLA for liberal arts or transfer, asappropriate.i.N/Aii. Coordinate across campuses to stagger cohorts. LR Note: Maybeapplicable with on-ground and an online or DE program. iii.N/Ab. If workforce need is at the bachelor’s level (not associates), reorganize under atransfer program.c. Review the extent to which the program is uniquely or strategically meeting ageneral education requirement (e.g., through scheduling or modality to meetstudents’ needs).3. To what extent can low enrolled courses ( 10) (login required for link) be scheduled morestrategically and cost-effectively? A combined Fall 2020 low enrolled course report isavailable here.Some potential solutions:a. Consolidate course offerings at one campus and provide distance delivery forstatewide access.DELIVERABLES1. Description of the group’s process.
Health ProgramsSingle-campus Discussion GroupPage 3 of 402. Key data indicators and trends that emerged from discussion as significant and reason forsignificance.3. Recommendations that emerged from the meeting. For example:a. For duplicated or similar programs, recommend program alignment andconsolidation options to meet student needs in the state.b. For single-campus programs, provide evidence of current and future demand(student and workforce) for the program and specific credentials being awarded.c. For duplicated or similar courses and/or low enrolled courses, provide at least tworecommendations for how courses can be scheduled and delivered more costeffectively.4. Faculty priorities regarding potential solutions.MAIN CONCEPTS Provide updated program information to include: maximum program capacity, the numberof students accepted each year, the retention, graduation, exam/registry pass, andemployment rates. Note: ARPD data is collected on a different timeline and will not alwayscapture graduate data accurately. How can we increase enrollment to address small class sizes? DE as a possible solution(one on ground cohort and a separate DE cohort)? Revisit lab ratios when not prescribedby accreditation? How can we schedule and deliver our programs more cost-effectively? Performcomparison with like programs from other community colleges within the ACCJC region.Review overall credits, number of lab hours, number of clinical hours, and programoutcomes (retention, graduation, exam/registry pass, and employment rates)The Nature of Selective Enrollment ProgramsAll the Health Academic Programs at Kapiʻolani Community College are selective enrollmentprograms. Each program's cohort size is limited based on the number of approved clinical sitesable to accept students during the semesters in which clinical experiences are scheduled. Foraccredited programs, the clinical sites must be approved, and the number of students each sitecan accommodate.ARPD Data DiscrepanciesARPD Data is collected on a Fiscal Year (July 1 - June 30). Data was captured for graduatingcohorts in Summer 2019, Fall 2019, and Spring 2020. ARPD adopted the FY reporting convention(as opposed to AY) to be consistent with UH System IRAPO data and Federal IPEDS data.Accredited Health Academic Programs must report program effectiveness data on an Academiccalendar. The difference in data collection timeframes may have caused a discrepancy in theprogram's reported program data and perceived ‘health.’ Program Directors were asked to provide2019 cohort data within their responses.Distance Education Growth of Health Academic ProgramsThe Hawai’i Pacific Basin AHEC Center Directors held a meeting on Tuesday, October 13. Therewere representatives from American Samoa, Palau, Yap, Northern Mariana Islands (CNMI),Guam, Pohnpei, and Marshall Islands (RMI). They need allied health training for all programs,focusing on Emergency Medical Technician, Medical Lab Technology, Radiologic Technology,and Respiratory Care Practitioner. Efforts are underway to offer accredited programs to non-US
Health ProgramsSingle-campus Discussion GroupPage 4 of 40territories using a Distance Education (DE) model where didactic information is delivered online.The hospitals serve as both the lab and clinical experience. By offering to several distant locations(to include the other Hawaiian Islands), cohort sizes will be large enough to support theinstructional costs. The 150% tuition rate policy for Pacific Islanders is under review to offer theseprograms to all USAPIs at the same rate of tuition.Meeting Workforce NeedsEmergency Medical Technician (EMT)Final Response: GUIDING QUESTIONS - PHASE 1- EMT Program ResponseKapi‘olani Community College Emergency Medical Services Department is responsible fortraining Emergency Medical Technicians (EMTs) and Paramedics (also known as MobileIntensive Care Technicians or MICT’s) seeking licenses to practice. This specialized training isprovided at our KapCC training centers located at KauCC, KapCC (main office), MC, and HawCC.KapCC has been the sole source training center for the state since 1986. Graduates of KapCCoften work for American Medical Response, the City and County of Honolulu, Hawaii FireDepartment.The Emergency Medical Technician program (EMT) resides within the Emergency MedicalServices (EMS) Department at Kapi'olani Community College (KapCC). Unlike our Paramedicprogram accredited through the Committee on Accreditation of Educational Programs for theEmergency Medical Services Professions (CoAEMSP), our EMT program, or any otherthroughout the nation, requires this type of credential.Currently, the KapCC EMT Program is the only training institution recognized by the Hawai'iDepartment of Health and the Department of Commerce and Consumer Affairs to provide aninstate instructional pathway that terminates with the ability to obtain a license. This sole-sourcestatus puts the EMT Program in a unique position in that we have to be very responsive to ourcritical infrastructure public safety provider needs being that every EMS provider in Hawaii isreliant on the UniversityFinally, both KapCC’s Paramedic and EMT programs' national credentialing test score pass ratesconsistently greatly exceed that of the rest of the nation (NREMT, 2020).1. To what extent are low enrolled programs or programs with low counts of graduates (less thanten graduates as a 3-year average) meeting workforce needs or meeting critical generaleducation requirements? The EMT program is not a low enrollment program as defined by this matrix. The UHCC Hawaii Career Explorer occupation profile also predicts a 10% increase inEMTs and Paramedics' needs. The US Department of Labor is anticipating a 7% growth rate indicating an increasingneed for EMT’s and Paramedics in Hawaii as compared to the rest of the nation
Health ProgramsSingle-campus Discussion GroupPage 5 of 40 The City and County of Honolulu reported they have approximately 10-20 vacancies peryear. Also, with COVID and budget issues, the City is anticipating more than averageloss due to retirements. As the primary EMS agency on Hawaii Island, Hawaii Fire Department providesadvanced notice for their training needs. The training needs generally result in anaverage of 1 EMT class per year on Hawaii Island (cohorts of approximately 14-28). AMR Maui does the same, which has resulted in offering EMT programs every otheryear (12-18). AMR Kauai has requested 2 EMT classes over the last ten years. AMROahu is adequately staffed. EMT cohorts, before COVID, have had as many as 24-students. Oahu's structurallimitations due to COVID have since limited enrollment to 16 in our primary EMTclassroom (and 12 in our secondary classroom). This structural limitation is our primarylimiting factor on Oahu, where there happens to be the greatest need for EMT’s andParamedics. Since EMT is a direct feeder to the paramedic program, the needs assessmentconducted by Leaugeay Barnes demonstrates a need for EMS personnel. (see NeedsReport. edited)https://uhcc.hawaii.edu/career explorer/occupations/profile.php?state HI&soc paramedics.htm2. If workforce need is at the certificate level (not associates), convert to a non-credit programwith articulation agreement or PLA for liberal arts or transfer, as appropriate. Opposed: This is counterintuitive to our current strategic plan (2015-2021) I: Hawai’iGraduation initiative subsections (A), (B), (D), and (J) affecting the pathway from EMTto ploads/2013/03/StrategicPlan2015-2021.pdf Opposed: PLA’s significantly increase the tuition expense for EMT’s who will transitionto the Paramedic Level. Students will be required to “buy back” creditsAlso, non-credit tuition for the initial program will have a negative effect. Opposed: EMT students may not have the same financial aid opportunities in a noncredit program (scholarships). Opposed: Farber and McTernan (1989) state in their article, “The Education Agendafor the Future: A System Approach” published by the National Highway Traffic SafetyAdministration (NHTSA) and the Health Resources and Services Administration(HRSA) that most allied health-related fields instituted more and better training andhave adopted education requirements that include formal academic degrees.
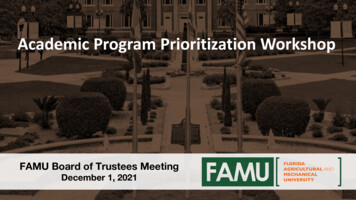
Health ProgramsSingle-campus Discussion Group Page 6 of 40Noncredit programs may significantly increase the program's cost as general fundsmay not be available to supplement the process, increasing the student's expense andif sponsored by an employer.3. Provide updated program information to include: maximum program capacity, the number ofstudents accepted each year, the retention, graduation, exam/registry pass, and employmentrates. Program Capacity / Class SizesClass sizing depends on how the program is delivered. As an example, the Maui EMS TrainingCenter’s capacity is 12 students; however, David Kingdon delivered the program as a hybrid.This required him to split the F-2-F sections into two, allowing for appropriate social distancing.The Oahu EMT classes share the spare classroom allowing for proper social distancing whenavailable. The Hawaii EMT Program, when MICT class is not in session, can flip, thusexpanding the capacity for EMT training. Following are the raw F-2-F numbers.Oahu MICT (205) 14 students Oahu EMT (206) 12 students Oahu EMT (108) 16students Maui EMS 12 studentsKauai EMS12 studentsHilo EMT (Bldg. 380/Room 36) 10 studentsHilo MICT (Bldg. 380 / Room 39) 20 studentsRemaining formation provide in graph form (number of students accepted each year,the retention, graduation, and exam/registry pass) EMT (Emergency Medical Technician) 1322718610684KapCC NREMT Cert.Exam Pass Rates1st Attempt / AllAttempts1st AllNationalPass 1816-271715-26261211141316* reenrollment from previous classes** NREMT.org77
Health ProgramsSingle-campus Discussion GroupPage 7 of 40 Pass Rates: The Program consistently outperforms the rest of the nation on first-timepass rates See 1.PROGRAM INFORMATION.docx). Employment Data: Accurate employment data is challenging to obtain. Typically, theprogram does not capture employment information. Graduates have an opportunityto work in many settings, such as at EMS, fire, ocean safety and police departments,hospitals, and clinics as examples. Several students have been inspired to move intoother health care settings, such as medicine and nursing. ARPD data grosslymisrepresents actuals in that employers have shared they need 10-20 or morereplacements each year.KapCC’s “Hawaii Fire Department EMT” classes have a 100% employment rateKapCC’s “Kauai Fire Department EMT” classes have a 100% employment rate.EMT classes on Oahu and Maui, based on informal surveys conducted by the facultymembers, suggest approximately 60-70% of graduates obtain employment in the field.Using employment rates to assess the efficiency of programs can fall on a slipperyslope. The primary purpose of the college is to educate/train students. The primarypurpose of the national certification agency/state licensing board is to validate thetraining. The primary purpose of the employer is to vet for employability. Thus, it isnot the primary responsibility of the college to determine if the student is instructional.php?action analysis&college KAP&year 2018&program 654. How can we schedule and deliver our programs more cost-effectively? Review overall credits,number of lab hours, number of clinical hours, and program outcomes (retention, graduation,exam/registry pass, and employment rates) (See 1.PROGRAM INFORMATION.docx) David Kingdon (Maui) is currently piloting an asynchronous hybrid program.We arefinding that due to Covid, F2F capacity is reduced due to social distancing, increasingthe number of instructional hours. We have proposed cost-sharing with the Honolulu Fire Department to increase thestudent population while reducing college costs. See below for an explanation: COVID 19 has reduced our capacity on Oahu at a time when demand is increasing.Thus, finding classrooms with a larger size will allow the program to maximizeinstructional efficiency while dramatically increasing revenues. A review of the program's structure (EMT 111 (EMT 115), EMT 120, and EMT 125) willallow for further segmentation of the program to distribute teaching loads more broadly.This action could reduce instructional expenses due to incorporating underloadedfaculty or lectures (vs. overload). Reducing instructional time (TE/Credits) is not recommended. Licensing requirementsfor the state far exceed that of the national norms. Licensing requirements mandate
Health ProgramsSingle-campus Discussion GroupPage 8 of 40EMTs’ are trained to work on a Paramedic ambulance. Reducing instructional timemay prevent students from obtaining a license to practice. Due to increased operational asks and coming out of a recession that usually increasesstudent populations, increasing the number of sections or section size will increaserevenues for the college.https://uhcc.hawaii.edu/career explorer/occupations/profile.php?state HI&soc -paramedics.htmMobile Intensive Care Tech (MICT)Final Response: GUIDING QUESTIONS - PHASE 1- Paramedic Program ResponseThe Paramedic Program resides within the Emergency Medical Services (EMS) Department atKapi'olani Community College (KapCC). Students are required to be Hawai'i state licensed EMTsto apply and be admitted to the Paramedic Program. The Commission on Accreditation of AlliedHealth Education Programs (CAAHEP) (Commission on Accreditation of Allied Health EducationPrograms [CAAHEP], n.d.) accredits the Program through recommendation by The Committeeon Accreditation of Educational Programs for the Emergency Medical Services Professions(CoAEMSP) (CoAEMSP, n.d.).Currently, the KapCC Paramedic Program is the only program recognized by the Hawai'iDepartment of Health and is therefore authorized to provide paramedic education and training forthe entire state. This sole-source status puts the Paramedic Program in a unique position. Wehave very little competition (few students who attend programs on the mainland and seekreciprocity). One poor-performing cohort can bring the state pass rates down and jeopardize bothaccreditation and the ability to provide competent graduates to meet Hawai'i EMS workforceneeds. Notably, the KapCC Paramedic Program has led the nation in first-time pass rates for overa decade (NREMT, 2020).1. To what extent are low enrolled programs or programs with low counts of graduates (lessthan ten graduates as a 3-year average) meeting workforce needs or meeting criticalgeneral education requirements? The Paramedic Program is not a low enrollment program defined by this overall;however, the neighbor islands may be. (see Attachment for EMT & paramedicinformation. (See 1.PROGRAM INFORMATION.docx) Response: All paramedic classes should have a minimum of 10 enrolled. The programwill utilize an asynchronous hybrid to provide greater access on all islands and greaterflexibility for scheduling faculty assignments. Rotating classes offered on neighborislands may be used. Labs will need lecturer support (see Needs Report. edited). Thestart of the Fall 2020 Hilo cohort was delayed to allow for an increase in enrollmentand offer qualified Kauai students access. We will pilot the Asynchronous HybridProgram in Jan. 2021. Additionally, see #4 below.
Health ProgramsSingle-campus Discussion Group Page 9 of 40The UHCC Occupation profile predicts a 10% increase in EMTs and paramedics1however, paramedic employment on all islands for all graduates is 100%. Although theO’ahu Paramedic Program typically accepts 12 students per cohort, we received 30applicants for the 2021 cohort and are looking at strategies to increase enrollment.The primary limiting factor continues to be access to prehospital clinical placement with the City& County of Honolulu EMS (HEMS). Paramedic students must complete 814 hours of internshiprotations requiring significant ambulance time, and mentors are trained to meet CoAEMSPrequirements.1. https://uhcc.hawaii.edu/career explorer/occupations/profile.php?state HI&soc 29-202. If workforce need is at the certificate level (not associates), convert to a non-credit programwith articulation agreement or PLA for liberal arts or transfer, as appropriate.a. Response: Opposed and recommended the College maintain both the CA and AD.See Below:1 CoAEMSP requires all paramedic programs to have a pathway to collegecredit.2 We encourage all graduates to pursue the degree; however, it is currently nota requirement for the industry (although it could be in HI). It was recommendedby faculty two years ago and was not supported by the administration.3 A certificate with no college credit (i.e., pursuing non-credit option) means agraduate has little to show for their time if they fail to renew their state ornational certification in 2 years. There is nothing of value to assist them infinding a new job or advancing in opportunities requiring a degree despitecompleting the equivalent of 40 CH. With college credit, they will always haveat least a CA to turn into an associate degree and then articulate into abachelor's degree.4 From a talk given by John Morton, funding to community colleges is based onthe number of degrees and CA certificates awarded, which is why the CAcertificate was created. All MICT graduates can be awarded a CA certificate.They have the course work and number of credits accumulated from the MICTclasses alone. If what John Morton stated still holds, keeping the CA isessential.5 It would not seem that having CA and AD would cost the College more moneyto conduct? All students are in the same cohorts (mixed), and in fact, the ADstudents add to the number of College credits in other classes (i.e., gen edclasses). Students can pursue what they are interested in and return after afew years to obtain their degree to articulate into the bachelor’s degree.6 The associate degree is a crucial step towards graduates obtaining abachelor's degree. It articulates with UH West O'ahu and gives students theability to obtain a bachelor's degree. Furthermore, to help advance theparamedicine field, having paramedics with degrees will help move theprofession forward. Eventually, paramedics will obtain graduate degrees anddoctorates.Doctoral candidates will perform research to advanceparamedicine further and legitimize it as a true profession. This educationprogression is what many fields have done in the past to advance the field andsubsequent higher-level career paths. The career span for many paramedics
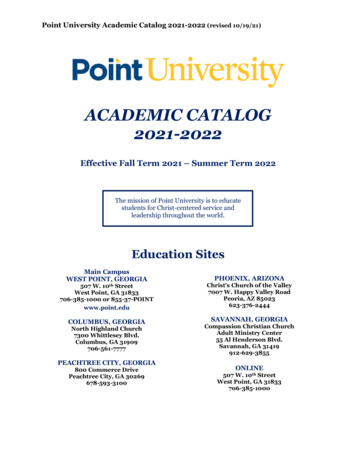
Health ProgramsSingle-campus Discussion Group7Page 10 of 40is relatively short. Having a bachelor's degree will provide additionalopportunities with better compensation if they decide to make a career change.Students may not have the same financial aid opportunities when in a noncredit program.3. Provide updated program information to include: maximum program capacity, the number ofstudents accepted each year, the retention, graduation, exam/registry pass, and employmentrates.a. NFORMATION.docx). The Program consistently outperforms the rest of the nation onfirst-time pass rates.Table 1: 2015-2020 Average TotalsAverageEmployment100%Average Retention84%AverageEnrollment19.6/ year9.1/ cohortAverageGraduationAverage 1st timePass RateNational 1st timePass Rate2015-2020 (N 6)2015-2020 (N 6)(outlier- 56% included)Range: 5-1316.3/ year84%97.8%2015-2020 (N 6)72%2015-20206)b. Program capacity limitation is due to the program's structure and clinical course timeframes limit the number of students who can enter the clinical setting. We are reviewingthe program to identify ways to accommodate larger numbers. Program graduationrates are at least 70%. As required by accreditation, 100% of all graduates pass thenational certification/state licensure exam, and 100% of graduates are immediatelyemployed (see Table 1 and 1. Program Information link). Note: ARPD data is collectedon a different timeline and will not always capture graduate data accurately.c. Program capacity limitation is also due to structural restrictions with COVID. Splittinglabs will allow the Program to accommodate classroom limitations while maintainingenrollment but will increase workload requirements.
Health ProgramsSingle-campus Discussion GroupPage 11 of 404. How can we schedule and deliver our programs more cost-effectively? Review overall credits,number of lab hours, number of clinical hours, and program outcomes (retention, graduation,exam/registry pass, and employment rates) (See 1.PROGRAM INFORMATION.docx).a. Response: (see Needs Report. edited (1).docx) We will pilot the asynchronous hybrid paramedic program for neighbor islandcohorts with low enrollment in Jan. 2021. We are also looking at offering someasynchronous hybrid slots to O’ahu applicants if they qualify for entry. Furtherdiscussions with HEMS are required. We discuss the possibility of increasing the cohort on O’ahu by splitting the labsand didactic and rotating students, potentially increasing enrollment from 1216;however, this would rely on HEMS ability to backfill additional personnel andincrease in AMR applicants.We have been working to eliminate barriers by reviewing the application processand updating the info session information to include strategies for successfullyapplying to the program. Some examples include: We are reviewing the requirement of 300 ambulance transports, which can bedifficult for neighbor island applicants to achieve, and are piloting a team leadoption (100) and a 50/50 split option. We are piloting an early provisional acceptance for military personnel to allowthem to compete for funding. The military personnel performance isbenchmarked against earlier cohorts' performance from all islands and a cutscore determined based on their likelihood of being admitted. If they fall in thisrange, we allow early provisional admittance. If not, they are ranked with therest of the class. (See Early Military Testing & Summary Raw ApplicantScores). We are piloting a Grit Survey to see if this reflects those most likely to persist. Zoom Info Sessions have increased attendance by agency administration,AMR personnel, and neighbor island potential students. This increase inattendance will improve everyone’s understanding of the process and lead tobetter-prepared applicants. We have also seen attendees with a few monthsof EMT experience preparing for the paramedic program. Typically, studentsattend the year before application. We are currently reviewing and discussing curriculum revisions; however,this will not be submitted until F2021 and implemented in F2022.Modifications of curriculum require significant work, which will require support from the college.a. Differentiate lab from didactic- there is a difference in the lecture (15) and lab or lab/lecture(18). Therefore, when I separated the lab, there was an increase in TE/ CH (from 40 to42), a move in the worn direction as far as the College is concerned but is a more accuratereflection of work.b. I cross-referenced the National EMS Education Standards along with our SLOs/ coursesbut was at nine months and 42 CH when I stopped due to tenure and challenges with theschedule.c. Classes designed which have non-fractional CH. Currently, most classes have fractionalCH. We will update to align with the current format. For example, two classes / 8 week or16 block semesters. Lab and clinical class could run the entire semester, potentially
Health ProgramsSingle-campus Discussion GroupPage 12 of 40expanding clinical access. This schedule change would increase flexibility, decrease thenumber of courses students need to enroll in, and align us with the academic calendar.d. We could modify some of the courses to run together in the same module. Separatecourses for lecture, lab, and clinical running concurrently increases flexibility and providesadditional access. The courses could be aligned to COI's needs.e. We are discussing the possibility of decreasing internship rotations from 5 to 4-weekblocks. There is also the possibility of the prehospital clinical courses replacing InternshipI, meaning we could go to 3 rotations with a 4th as needed. We piloted grading primaryassessment this semester utilizing new evaluation tools we developed last year andemploying directed scenario practice. It was successful, with mentors indicating studentswere better prepared for the primary assessment rotation. Unfortunately, COVID resultedin minimizing lab time. We had just started History & PE in the scenario and cannotdetermine the level of success we may have had.f. Revisiting how we calculate internship and clinical TEs may also be a solution to loweringour overhead. Currently, we use 24 as the denominator in our TE calculations. However,employing a model with decreased instructor interaction, we could use 45 as the basis.Before we propose this to our administration, it would be prudent to do the calculationsand see how it panned out. An example would be; currently, internships are 202.5hours.202.5 divided by 24 8.43 TE. If changed to 45, 202.5 divided by 45 4.5 TE.The instructional costs would be reduced significantly.CoAEMSP. (n.d.). [CoAEMSP home page]. https://coaemsp.org/Commission on Accreditation of Allied Health Education Programs. (n.d.). [CAAHEP home page].https://www.caahep.org/Occupational Therapy Assistant (OTA)KapCC Campus Discussions Phase I Response: Occupational Therapy Assistant ProgramThe Occupational Therapy Assistant Program (OTA) at Kapi’olani Community College hasdistinct value to Hawaii’s healthcare system. The OTA Program:I. Prepares Hawai’i residents to meet state workforce needs in healthcare Actively works to align with Accountability Core Indicators of Performance Engages in a rigorous examination of goals, activities, and achievements and makescalculated adjustments in response.Preparation of Hawai’i Residents to Meet State Workforce Needs in HealthcareAs the only occupational therapy educat
average of 1 EMT class per year on Hawaii Island (cohorts of approximately 14-28). AMR Maui does the same, which has resulted in offering EMT programs every other year (12-18). AMR Kauai has requested 2 EMT classes over the last ten years. AMR Oahu is adequately staffed. EMT cohorts, before COVID, have had as many as 24-students. Oahu's .