Transcription
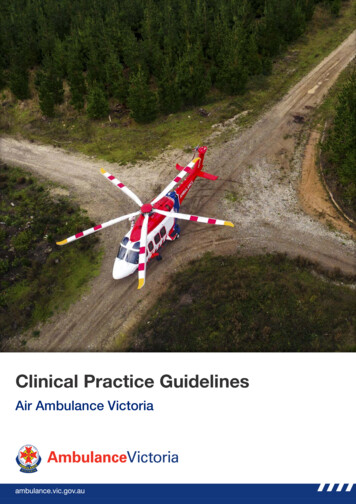
Clinical Practice GuidelinesAir Ambulance Victoria
AboutThis work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0International License. Ambulance Victoria 2019The information contained in ‘Clinical Practice Guidelines for Ambulance and MICA Paramedics’ (‘thework’) has been developed and is owned by Ambulance Victoria, with the exception of content provided bythird parties and other excluded material identified below. An online version of the work can be accessedfrom: https://cpg.ambulance.vic.gov.auWith the exception of: Ambulance Victoria’s branding, logos and trademarks; other trademarks, logos and coats of arms; and content supplied by third parties,the work is available under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0International License. Licensees can copy and distribute the material for non-commercial purposes only. Ifyou remix, transform or build upon the material you may not distribute the modified material.To view a copy of this licence visit the Creative Commons website using the following /4.0/legalcodeUse of the work under the above Creative Commons Licence requires you to attribute the work in anyreasonable manner requested by Ambulance Victoria, but not in a way that suggests that AmbulanceVictoria endorses you or your use of the work. The following is provided to enable you to meet yourobligation under the Creative Commons Licence.Material used ‘as supplied’Source: ‘Clinical Practice Guidelines for Ambulance and MICA Paramedics’, Ambulance Victoria, 2019.Available under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.Derivative material for internal use onlyBased on ‘Clinical Practice Guidelines for Ambulance and MICA Paramedics’, Ambulance Victoria, 2019, asamended by [insert name].The original resource is available under a Creative Commons Attribution-NonCommercial-NoDerivatives4.0 International License. An online version of the original resource can be accessed from:https://cpg.ambulance.vic.gov.au.Third Party CopyrightIn some cases, a third party may hold copyright in material presented in the work. Their permission may berequired to use that material.1This is an uncontrolled document, it is the reader's responsibility to ensure currency.AboutPage 1 of 2
AboutEnquiriesEnquiries in relation to these guidelines can be emailed to: hese Clinical Practice Guidelines (CPGs) are expressly intended for use by Ambulance Victoriaparamedics and first responders when performing duties and delivering ambulance services for, and onbehalf of, Ambulance Victoria.Other users:The content of these CPGs is provided for information purposes only and is not intended to serve ashealth, medical or treatment advice. Ambulance Victoria does not represent or warrant that the content ofthese CPGs is accurate, reliable, up-to-date, complete or that the information contained in these CPGs issuitable for your needs or for any particular purpose. You are responsible for assessing whether theinformation is accurate, reliable, up-to-date, authentic, relevant or complete and where appropriate, seekindependent professional advice.To the maximum extent permitted by law, Ambulance Victoria excludes liability (including liability innegligence) for any direct, special, indirect, incidental, consequential, punitive, exemplary or other loss,cost, damage or expense arising out of, or in connection with, use or reliance on these CPGs or anyinformation contained in the CPGs (including without limitation any interference with or damage to a user’scomputer, device, software or data occurring in connection with the CPGs or their use).These CPGs provide links to external websites. Ambulance Victoria does not control and accepts noliability for the content of those websites or for any direct, special, indirect, incidental, consequential,punitive, exemplary, or other loss, cost, damage or expense arising from use or reliance on those websites.Ambulance Victoria does not endorse any external website and does not warrant that they are accurate,authentic, reliable, up-to-date, relevant or complete. Your use of any external website is governed by theterms of that website. The provision of a link to an external website does not authorise you to reproduce,adapt, modify, communicate or in any way deal with the material on that site.If these CPGs contains links to your website and you have any objection to such links, please contactAmbulance Victoria at: clinicalguidelines@ambulance.vic.gov.auDeveloped by Media4Learning: www.media4learning.co.nz2This is an uncontrolled document, it is the reader's responsibility to ensure currency.AboutPage 2 of 2
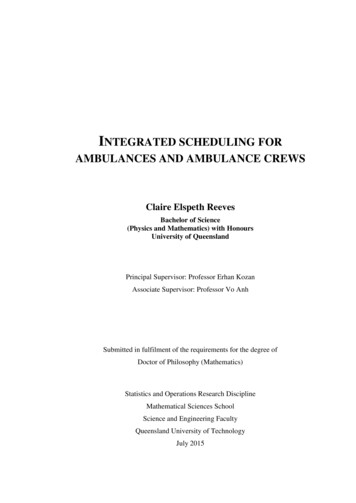
Rapid Sequence IntubationCPG AAV 01Care Objective Ensure safe and effective airway management throughout entire episode of care To be read as an adjunct to CPG A0302 Endotracheal intubation. This CPG includes two additionalpathways available to MICA flight paramedics.General notes While traditionally patients with altered conscious state are intubated for airway protection duringaeromedical transport, it is not a mandated clinical requirement. Transport time, ability to divert,reason for transport and clinical fragility must be taken into account even in the setting ofaeromedical retrieval. The term ‘peri-arrest’ is reserved for the patient whose vital signs predict a strong likelihood of rapiddeterioration into cardiac arrest. Due to the rapid metabolism/off-set of propofol in critically unwell patients, an immediate postintubation bolus of propofol and subsequent infusion will be required to maintain anaesthesia /sedation. MFPs are authorised to undertake a second RSI in the setting of a failed intubation where it’sdeemed to be clinically appropriate and safe to do so. A second RSI should be undertaken as perCPG A0302/AAV 01.RSI – Crash airway The aim is to secure the airway rapidly while avoiding haemodynamic compromise and extendedscene/procedure times in unconscious patients who require immediate airway management toprevent pending cardiac arrest. It is expected that concurrent IV access should be attempted if not already obtained. RSI with a paralytic only and with expedited preparation is permitted where there is an immediateneed to secure the airway and:——Administration of sedative / analgesic is likely to cause delay and / or haemodynamic collapsePeri arrest, airway reflexes presentThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 3.0.0 - 21/09/20Exported 02/11/2020Rapid Sequence Intubation CPG AAV 013Page 1 of 2
Rapid Sequence IntubationCPG AAV 01FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 3.0.0 - 21/09/20Exported 02/11/2020Rapid Sequence Intubation CPG AAV 014Page 2 of 2
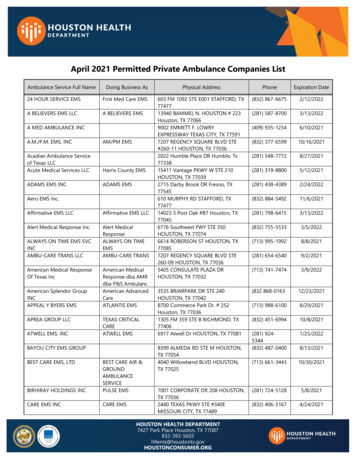
Difficult Airway GuidelineCPG AAV 02General NotesGuideline Principles This guideline supplements CPG A0303 Difficult Airway Guideline, which applies to all MICAParamedics. In addition to the following notes, Plan C is the key variation from CPG A0303.Crew Resource Management In complex cases where MFPs are committed to other tasks (such as finger thoracostomy) the mostexperienced MICA Paramedic should be selected for intubation.Additional intubation attempts MFPs should in general abide by the limitation of two intubation attempts. However a third attemptmay be appropriate in the setting of:——Oxygen saturations can be maintainedThere is an identified corrective intubation strategy (E.g. technique issues, airway visibility,insufficient ramping, equipment failure, etc.)Plan C The intubating LMA replaces the iGel within Plan C. In the setting of intubating LMA insertion, correction of desaturation by ventilation should beundertaken prior to ETT insertion through the device. With regard to iLMA:——LMA success is measured by oxygenationiLMA-ETT success is measured by electronic ETCO2This is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 2.0.0 - 21/09/20Exported 02/11/2020Difficult Airway Guideline CPG AAV 025Page 1 of 2
Difficult Airway GuidelineCPG AAV 02FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 2.0.0 - 21/09/20Exported 02/11/2020Difficult Airway Guideline CPG AAV 026Page 2 of 2
Airway MaintenanceCPG AAV 13Care Objective Optimise sedation /- paralysis Optimise ventilation parameters using lung protective strategies Undertake the ‘Critical IHT Checklist’ to ensure comprehensive patient care post intubation To be read as an adjunct to CPG A0305 Airway MaintenanceThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.0 - 21/09/20Exported 02/11/2020Airway Maintenance CPG AAV 137Page 1 of 3
Airway MaintenanceCPG AAV 13General NotesSedation and Paralysis If Propofol is given to induce unconsciousness then consider post intubation sedation using:—Propofol infusion at rate 100 mg – 300 mg/hr (10 – 30 mL/hr). Add Morphine infusion forpatients intubated with Propofol with underlying pain If patient has had continuous seizure activity:——————Midazolam Infusion @ 0.2 – 0.4 mg/kg/hr IV as an independent infusionSupplement with Midazolam 0.05 – 0.1 mg/kg IV bolus as required (nil maximum)Consider adding Propofol infusion 50 – 200 mg/hr in the seizure patient who appearsresistant to opioid / midazolam sedation.It is preferable to over-sedate these patients to maintain patient control than administerparalysis and potentially mask seizure activity.Patients intubated for status epilepticus should not receive routine post intubation paralysis.However if sedation using Midazolam and Propofol is insufficient to safely maintain intubationand ventilation, then Rocuronium should be administeredPatient receiving high dose sedation may require cardiovascular supportTrauma Blood pressure should be managed as per CPG AAV 08 Inadequate Perfusion associated withHypovolaemiaNon-traumatic brain injury In suspected NTBI due to suspected intracranial bleeding or sub-arachnoid haemorrhage (pre-RSIGCS 8), maintain SBP 120 mmHg and 140mmHg. If hypotension is present in the suspected NTBI (SBP 120 mmHg):———Maintain minimum sedation rates of Fentanyl 20 mcg/hr and Midazolam at 2 mg/hr IVAdminister Normal Saline 0.9% 20 mL/kg IV, titrated to target BPIf SBP remains 120 mmHg despite fluid challenge then consider Noradrenaline infusion.Titrate to a SBP 120 mmHg using a dose between 5 – 25 mcg/min IV (5 mL/hr – 25 mL/hr) If hypertension is present (SBP 140 mmHg) despite Fentanyl 100 mcg/hr and Midazolam at 10mg/hr——Administer Propofol 0.5 mg/kg IV bolus. Repeat as requiredConsider Propofol infusion at 50 mg/hr (5 mL/hr). Titrate to effectThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.0 - 21/09/20Exported 02/11/2020Airway Maintenance CPG AAV 138Page 2 of 3
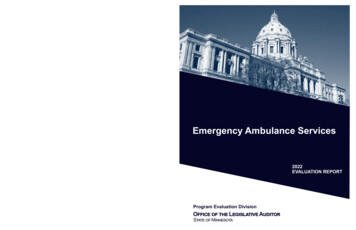
Airway MaintenanceCPG AAV 13Mechanical VentilationObstructivelungNormal lungAcutebronchospasm,COPD, asthmaModeFiO2Tidal VolumeARDS, obesity, pneumonia, aspiration,pulmonary fibrosisSIMV Volume-Control1.0May be titrated once stable, stationary and ventilator/ETT is secure.6 – 8 mL/kg6–8RateRestrictive lungTitrate tocorrect forAutoPEEP,blood pressure,blood gasesand PIPs6 mL/kg12 – 15Titrate rate and VT totarget EtCO2 30 – 35mmHg or blood gases 18Titrate to ABGsRate is usually the primary method for adjusting Minute VolumeABG / VBG analysis should be used to guide ventilation strategy where possibleMetabolic acidosis: MV to target EtCO2 (expected PCO2 (1.5 x HCO3-) 8)PEEPZeroI:E1:6–8Inspiratorytime1 – 1.5 secondsPIPs mayexceed 40 -60cmH2O,particularly inacute AsthmaOtherSerialUltrasound:Consider rulingout TPTdevelopmentEtCO2: Accepthypercapniabut aim for pH 7.15 cmH2O5 – 15 cmH2OTitrate to SpO2 94%1:2–31 : 1 – 1.5Titrateto indicated I:EConsider ABGanalysis: ETCO2 can bean unreliable guide forPCO2, even in ‘stable’patientsMost critical patientsare acidotic: Does thepatient requirerespiratorycompensation andhigher MVs?Avoid disconnection / suctioning asoptimal lung recruitment depends oncontinuous airway pressure (PEEP).EtCO2: Mild hypercapnia acceptable inrestrictive lung patients without brain injury.Severe multi-trauma: Where combinedhead / chest injury, blood pressurepreservation outweighs normalisation ofblood gases. Titrate Mean AirwaysPressure accordingly.Monitor for ventilator synchrony and MV.SpontaneouslyVentilatingPressure support (5 – 10 cmH2O) titrated to expected VT and complianceEnsure triggering and sensitivity accurately captures breaths.Sedation must be adequate to avoid asynchrony.This is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.0 - 21/09/20Exported 02/11/2020Airway Maintenance CPG AAV 139Page 3 of 3
Transthoracic PacingCPG AAV 03FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/12/2014Exported 02/11/2020Transthoracic Pacing CPG AAV 0310Page 1 of 1
Transvenous PacingCPG AAV 04Pacing Wire Care In general the OUTPUT setting on the pacemaker should be set at 2 times the THRESHOLD levelplus 1mA (i.e. 2 x THRESHOLD(mA) 1mA) Pacing THRESHOLD would usually be determined on consultation with the sending hospital In general the SENSITIVITY setting should be set towards the maximum sensitivity (i.e. 0.5mV is themost sensitive) If Transthoracic Pacing instituted prior to or during flight consider implications on mission safety andappropriate communication with relevant aircrew/pilot.This is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/07/2010Exported 02/11/2020Transvenous Pacing CPG AAV 0411Page 1 of 2
Transvenous PacingCPG AAV 04FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/07/2010Exported 02/11/2020Transvenous Pacing CPG AAV 0412Page 2 of 2
Pain ReliefCPG AAV 05General Notes Multimodal pain relief is recognised as the most effective pathway for efficacious analgesia and limitsexcessive opiate administration. Unless contraindicated Paracetamol IV should be administered to alltrauma patients complaining of pain. Parecoxib, in addition, should be strongly considered forpatients with moderate to severe pain unless contraindicated. Paracetamol and Parecoxib are slow acting, long lasting agents that provide bridging analgesiabetween the prehospital and Emergency Department settings. The use of Ketamine is not specifically contraindicated in the patient requiring winching. HoweverMFPs must be acutely aware that that a dissociated patient can be an inherent safety risk during thewinching operation. Ideally patients should be allowed time to return to full consciousness prior toextrication and MFPs should include this potential delay in winch operations planning. Alternatively,other analgesic agents such as Methoxyflurane may be considered for procedural pain relief in thewinch setting. ALS Flight Paramedics must consult with either the clinician or a MFP via the FCC prior to exceedingMorphine 20 mg IV or Fentanyl 200 mcg IVInfusionsMorphine Infusion Morphine 30 mg added to make 30 mL with Dextrose 5% or Normal Saline. 1 mL/hr 1 mg/hrFentanyl Infusion Fentanyl 300 mcg added to make 30 mL with Dextrose 5% or Normal Saline 1 mL/hr 10 mcg/hrKetamine Infusion Ketamine 50 mg added to make 50 mL with Dextrose 5% or Normal Saline 1 mL/hr 1 mg/hrKetamine 50 mg may be obtained by adding 50 mg (5 mL) of the pre-diluted 10 mg/mL Ketamine solutionto 45 mL Dextrose 5% or Normal Saline to make a 1 mg/mL dilutionThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.2 - 21/09/20Exported 02/11/2020Pain Relief CPG AAV 0513Page 1 of 2
Pain ReliefCPG AAV 05FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.2 - 21/09/20Exported 02/11/2020Pain Relief CPG AAV 0514Page 2 of 2
Inadequate Perfusion Associated withSepsisCPG AAV 07Special Notes Noradrenaline infusion preparation——Noradrenaline 3mg added to 47ml of Dextrose 5% or Normal Saline1ml/hr 1 mcg/min Steroid therapy is not routinely administered in severe sepsis Appropriate antibiotics should be administered. Consult with receiving hospital for administration ofCeftriaxone 1gm IV For inter-hospital transfers, consult with ARV for recommended antibiotic therapyFlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 3 - 1/12/2010Exported 02/11/2020Inadequate Perfusion Associated with Sepsis CPG AAV 0715Page 1 of 1
Inadequate Perfusion Associated withHypovolemiaCPG AAV 08Special NotesAdditional Modifying Factors Penetrating trunk trauma – accept a palpable carotid pulse and transport immediately. The treatmentof major haemorrhage following penetrating truncal trauma is surgical. In cases where there is uncontrolled bleeding and the flight time is short, there must be no additionalscene time spent undertaking RSI, even in the comatose patient If the patient is aged 15 – 17 years, parental consent is required for administration of PRCC iCa should be measured as early as practicable in patients with haemorrhagic hypovolaemia.Calcium Gluconate 10% may be administered empirically following 4 units of PRCC or wherehypocalcaemia is identified (regardless of the number of units of PRCC administered). Ifhypocalcaemia is present following the initial dose for either indication, a repeat dose may beadministered.This is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.0 - 21/09/20Exported 02/11/2020Inadequate Perfusion Associated with Hypovolemia CPG AAV 0816Page 1 of 2
Inadequate Perfusion Associated withHypovolemiaCPG AAV 08FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.0 - 21/09/20Exported 02/11/2020Inadequate Perfusion Associated with Hypovolemia CPG AAV 0817Page 2 of 2
Chest InjuryCPG AAV 09General Care Always consider pneumothorax and/or haemothorax in the setting of unexplained hypotension,especially in the setting of traumatic chest injury and positive pressure ventilation Early targeted pain relief in the conscious chest injury patient remains an important strategy formaximizing spontaneous minute volume and patient comfort. In the setting of major chest trauma in the IHT, consult with ARV.FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 2.0.0 - 21/09/20Exported 02/11/2020Chest Injury CPG AAV 0918Page 1 of 2
Chest InjuryCPG AAV 09Related /CWI/CWI OPS 170 Pleural Decompression with FingerThoracostomy [CPG AAV 09].pdfThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 2.0.0 - 21/09/20Exported 02/11/2020Chest Injury CPG AAV 0919Page 2 of 2
Spinal Cord InjuryCPG AAV 10FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/06/2015Exported 02/11/2020Spinal Cord Injury CPG AAV 1020Page 1 of 1
Traumatic Cardiac ArrestCPG AAV 11General Care This CPG is to be used in conjunction with and as an adjunct to AV CPG A0201 Cardiac ArrestTraumatic Cardiac Arrest The intent is to prioritise haemorrhage control and managing correctable causes prior to othertherapies. Priorities include oxygenation and ventilation; exclusion of tension pneumothorax byinsertion of bilateral pleural decompression and administration of Red Cell Concentrate x 4 IV/IO inorder of clinical need. This should be followed by routine cardiac arrest management includingcardiac rhythm check. Once correctable causes have been addressed, a cardiac rhythm check andother standard cardiac arrest therapies such as compressions and adrenaline should beadministered. In cases where the Hx, MOI or injuries are inconsistent with traumatic cardiac arrest, or patient is inVF/VT, consider medical cause. If any doubt exists as to the cause of arrest, treat as per MedicalCardiac Arrest. Control of major haemorrhage is a priority and can be achieved with tourniquets, haemostaticdressings and/or direct pressure. A pelvic splint should be applied after other interventions in undifferentiated blunt trauma. Wherepelvic fracture is clearly contributing to cardiac arrest, a pelvic splint may be applied earlier. A supraglottic airway is an appropriate option to manage the airway initially and to facilitatecontinuous compressions. When ETT is attempted, it should not interrupt compressions. ETCO2 can be used as a surrogate marker of cardiac output during cardiac arrest. Wherecapnography is available, measure ETCO2. An ETCO2 reading greater than 10mmHg is desirable. Where clear signs of prolonged cardiac arrest are present, or continued resuscitation may be futile,consider AAV CPG G 01 and/or AV CPG A0203 Withholding or Ceasing Resuscitation. IV access may be difficult in this cohort of patient and consideration should be given to rapidlyestablishing peripheral access via IO.Ratios of compression to ventilation:No ETT/SGA 30 compressions to 2 ventilations Aim for 100 – 120 compressions per minute Pause for ventilationsETT/SGA 15 compressions to 1 ventilation Aim for 100 – 120 compressions per minute 6 - 8 ventilations per minute No pause for ventilations The required depth of compression is 5cm and full recoil of the chest should be allowed.This is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/09/2016Exported 02/11/2020Traumatic Cardiac Arrest CPG AAV 1121Page 1 of 2
Traumatic Cardiac ArrestCPG AAV 11 Evidence suggests compressions rates often differ from recommendations. Consider usingmetronome if available. CPR operators should rotate every 2 minutes to reduce fatigue and maintain performance. A gradualfall in ETCO2 may suggest fatigue during CPR.FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/09/2016Exported 02/11/2020Traumatic Cardiac Arrest CPG AAV 1122Page 2 of 2
AsthmaCPG AAV 12General Notes This CPG applies to critical asthmatic patients who remain acutely unwell despite salbutamol,ipratropium bromide and adrenaline therapy given as per CPG A0601 Asthma. Consider administration of Magnesium Sulfate as soon as practicable following commencement ofadrenaline infusion.InfusionsADULT Dilute Magnesium Sulfate 10 mmol (2.5 g) to 25mL with Normal Saline (this equals 100 mg / 1mL) for IV administration. Administer 10 mmol (2.5 g) via infusion pump over 20 minutes.FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.0.0 - 22/07/20Exported 02/11/2020Asthma CPG AAV 1223Page 1 of 1
Rapid Sequence Intubation(Paediatric)CPG AAV P01 This guideline is to be read as an adjunct to CPG AAV A01 Rapid Sequence Intubation and CPGP0301 Endotracheal intubation (paediatric)FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 2.0.0 - 21/09/20Exported 02/11/2020Rapid Sequence Intubation (Paediatric) CPG AAV P0124Page 1 of 1
Airway Maintenance (Paediatric)CPG AAV P08 This guideline is to be read as an adjunct to CPG P0303 Airway Maintenance (paediatric)FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Exported 02/11/2020Airway Maintenance (Paediatric) CPG AAV P0825Page 1 of 1
Pain ReliefCPG AAV P03General Notes Multimodal pain relief is recognised as the most effective pathway for efficacious analgesia and limitsexcessive opiate administration. Unless contraindicated, Paracetamol IV should be administered toall trauma patients complaining of pain regardless of severity. Parecoxib, in addition, should bestrongly considered for patients with moderate to severe pain unless contraindicated. Paracetamol and Parecoxib are slow acting, long lasting agents that provide bridging analgesiabetween the prehospital and emergency department settings. Dose errors in IV paracetamol administration for paediatrics is a documented issue. Do notadminister paracetamol directly from the soft pack to paediatric patients. To avoid the risk ofoverdose, draw the required dose out of the soft pack and administer from a separate syringe. The use of Ketamine is not specifically contraindicated in the patient requiring winching. HoweverMFPs must be acutely aware that that a dissociated patient can be an inherent safety risk during thewinching operation. Ideally patients should be allowed time to return to full consciousness prior toextrication and MFPs should include this potential delay in winch operations planning. Alternatively,other analgesic agents such as Methoxyflurane may be considered for procedural pain relief in thewinch setting ALS Flight Paramedics are not permitted to cannulate paediatric patients for the administration ofanalgesia. In the event of an established IV, ALS Flight Paramedics are to consult with an on dutyMFP via the FCC for specific treatment outlined in this CPG.IV Paracetamol dose / volume tableAge(years)Weight(kg)Dose(mg)Total volume(mL)Rate(mL/hr)3 months6909366 months812012481 3349549.5198113654054216InfusionsThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.1.1 - 21/09/20Exported 02/11/2020Pain Relief CPG AAV P0326Page 1 of 2
Pain ReliefCPG AAV P03Morphine Infusion Morphine 30 mg added to make 30 mL with Dextrose 5% or Normal Saline 1 mL/hr 1 mg/hrFentanyl Infusion Fentanyl 300 mcg added to make 30 mL with Dextrose 5% or Normal Saline 1 mL/hr 10 mcg/hrKetamine Infusion Ketamine 50 mg added to make 50 mL with Dextrose 5% or Normal Saline 1 mL/hr 1 mg/hrKetamine 50 mg may be obtained by adding 50 mg (5 mL) of the pre-diluted 10 mg/mL Ketamine solutionto 45 mL Dextrose 5% or Normal Saline to make a 1 mg/mL dilutionFlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1.1.1 - 21/09/20Exported 02/11/2020Pain Relief CPG AAV P0327Page 2 of 2
Inadequate Perfusion Associated withHypovolemiaCPG AAV P05FlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/09/2016Exported 02/11/2020Inadequate Perfusion Associated with Hypovolemia CPG AAV P0528Page 1 of 1
Traumatic Cardiac ArrestCPG AAV P06General Care This CPG is to be used in conjunction with and as an adjunct to AV CPG P0201 Cardiac Arrest(Paediatric)Traumatic Cardiac Arrest The intent is to prioritise haemorrhage control and managing correctable causes prior to othertherapies. Priorities include oxygenation and ventilation; exclusion of tension pneumothorax byinsertion of bilateral intercostal catheters; and administration of Red Cell Concentrate 10ml/kg IV/IOin order of clinical need. This should be followed by routine cardiac arrest management includingcardiac rhythm check. Once correctable causes have been addressed, a cardiac rhythm check andother standard cardiac arrest therapies such as compressions and adrenaline should beadministered. In cases where the Hx, MOI or injuries are inconsistent with traumatic cardiac arrest, or patient is inVF/VT, consider medical cause. If any doubt exists as to the cause of arrest, treat as per MedicalCardiac Arrest. Control of major haemorrhage is a priority and can be achieved with tourniquets, haemostaticdressings and/or direct pressure. A pelvic splint should be applied after other interventions in undifferentiated blunt trauma. Wherepelvic fracture is clearly contributing to cardiac arrest, a pelvic splint may be applied earlier. A supraglottic airway is an appropriate option to manage the airway initially and to facilitatecontinuous compressions. When ETT is attempted, it should not interrupt compressions. ETCO2 can be used as a surrogate marker of cardiac output during cardiac arrest. Wherecapnography is available, measure ETCO2. An ETCO2 reading greater than 10mmHg is desirable. Where clear signs of prolonged cardiac arrest are present, or continued resuscitation may be futile,consider AAV CPG G01 and/or AV CPG A0203 Withholding or Ceasing Resuscitation.Administration of Red Cell Concentrate (RCC) It is a legal requirement to obtain parental consent prior to administration of Red Cell Concentrate forany patient aged under 18 years (except if married). Therefore RCC must only be administered to achild 18 years if a parent/legal guardian can be contacted and the parent/legal guardian does notobject to the administration of a “blood transfusion”Ratios of compression to ventilationNo ETT/SGA 15 compressions to 2 ventilations Aim for 100 - 120 compressions per minute 14 ventilations per minute Pause for ventilationsETT/SGA 15 compressions to 2 ventilationsThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/09/2016Exported 02/11/2020Traumatic Cardiac Arrest CPG AAV P0629Page 1 of 2
Traumatic Cardiac ArrestCPG AAV P06 Aim for 100 - 120 compressions per minute 14 ventilations per minute No pause for ventilationsFlowchartThis is an uncontrolled document, it is the reader's responsibility to ensure currency.Version 1 - 1/09/2016Exported 02/11/2020Traumatic Cardiac Arrest CPG AAV P0630Page 2 of 2
AsthmaCPG AAV P07General Notes This CPG applies to critical asthmatic patients who remain acutely unwell despite salbutamol,ipratropium bromide and adrenaline therapy given as per CPG P0602 Asthma. Consider administration of Magnesium
Rapid Sequence Intubation CPG AAV 01 Version 3.0.0 - 21/09/20 Exported 02/11/2020 Rapid Sequence Intubation CPG AAV 01 Page 1 of 2 This is an uncontrolled document, it is the reader's responsibility to ensure currency.
![MOH STANDARDS FOR EMERGENCY AMBULANCE SERVICE (2017) [Updated 21 Nov 2018]](/img/51/emergencyambulancestandards.jpg)