Transcription
Design and Validation of a 2nd Tier NextGeneration Sequencing (NGS) Panel forNewborn Screening for Severe CombinedImmunodeficiency Disease (SCID)September 13, 2017Colleen Stevens, Ph.D.Research ScientistNYSDOH Wadsworth CenterNewborn Screening Program
September 13, 20172Current Testing Algorithm for SCIDT-cell receptor excision circle(TREC) assay 125 Avg. TRECsRefer to Specialist for Diagnostic TestingPhysician ordered testsCBC, Flow cytometry, Mitogen studiesMolecular tests – candidate genes;gene panel Insurance issues Slow TAT (2-8 wks) Increased stress to families
September 13, 20173Potential Benefits of Molecular Testing by the NBSProgram: Shortened TAT to identify genetic basis of disease Faster diagnosis; phenotype prediction Earlier decision on best treatment options – betteroutcomes Cost savings to family and health care system Less stress for families
September 13, 2017APHL/CDC Cooperative Agreement - Specific Aims Develop and validate a 2nd tier multi-gene immunodeficiency panelon 2 different commonly used NGS platforms Compare the 2 platforms for accuracy, ease of use, cost and turnaround time Evaluate Utility of Targeted NGS for SCID Identify causative gene? Shortened time to diagnosis? Earlier, targeted treatment? Provide CDC with quality control/reference samples4
September 13, 20175NYS NBS 39-gene SCID panelGene Selection: Commercial SCID panels CLSI guideline Literature search and case RMRPSLC46A1STAT5BTBX1WASZAP70
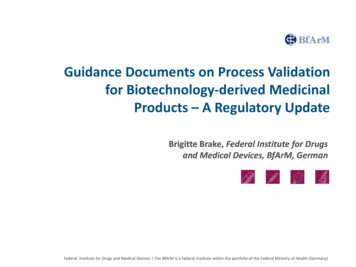
September 13, 20176NGS PlatformsIllumina MiSeq –TruSeq CustomAmplicon (TSCA) panelLife TechnologiesIon Torrent S5AmpliSeq (AS) panel
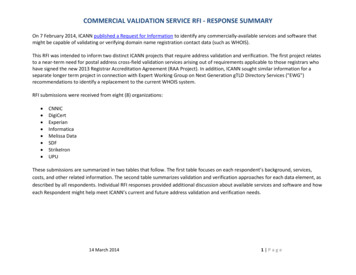
September 13, 20177Platform ComparisonsIllumina MiSeqSpecificationIon Torrent S510 ngRecommended Minimum DNAInput1 ngPaired-end readsSequence ReadsSingle end readsLigation capture/amplificationLibrary Prep/Gene TargetingMultiplex PCRReversible terminator withfluorescent dNTPsSequence detectionSemiconductor basedsequencingThe workflow isvery similar forboth platformsMiSeq Flow CellIon Chip
September 13, 20178SCID NGS Turn-Around Time (TAT)MiSeqTorrentStep8Samples16Samples1 hr1 hr8 hr(3 hrs hands on)8 hr(3 hrs hands on)Library Prep *15 min15 minLoading chip *17 hrs24 hrs4 hrs30.25 hrsDNA Extraction(Generations Soln)8Samples16Samples1 hr1 hr8 hrs16 hrs(15 min hands on)(15 min hands on)15 hrs15 hrs(15 min hands on)(15 min hands on)Instrument run time2.5 hrs2.5 hrs6 hrsBasecalling alignment(platform software)5 hrs8 hrs39.25 hrsTotal TAT(to raw data)31.5 hrs42.5 hrs*Library prep and chip loading: Manual for MiSeq (performed by Core facility)Ion Chef for Torrent (8 samples at a time)
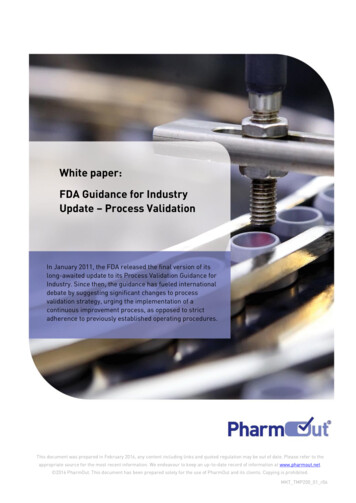
September 13, 20179NGS Data Analysis – Bioinformatics PipelineMiSeq Reporter / Torrent ServerFilter out benign/likely benign variantsFASTQCalling bases- SequencefileBAMAlignsequence toreference DetectvariantsVCFAnnotatevariants –Gene/ cDNA/ aa changeClinicalReportDo you need someone trained in Bioinformatics?Relevant Variants/Other incidentalfindings (carrier)
September 13, 201710Not necessarily, but .Bcbio NGS Bioinformatics Tools Genome Build: GRCh37 Alignment: bwa-mem Variant Callers: freebayes, gatk-haplotype& samtools Variant Filtering (quality): bcftools RTG vcfeval used to generatethresholds for filtering Variant Annotation: snpeff, VEP & vcfanno dbnsfp 3.3a (gnomad, exac, 1000g etc) clinvar 20160502 dbsnp 147-20160408 Variant Prioritization: st/contents/internals.html
September 13, 2017Validation Plan NGS Sequence1) 8 samples from infants diagnosed with SCID – genetic cause known2) 16 samples from infants diagnosed with SCID or other immunodeficiency –genetic cause known/unknown3) Reference Sample – NA12878 (NIST; GIAB) – variants published Sanger sequence 8 samples from #1 above All 39 genes 657 amplicons/sample 5256 amplicons total 16 samples from #2 above Sanger confirm pathogenic/likely pathogenic and VOUS Every sample sequenced in 2 separate runs on each platform – inter-assayreproducibility One sample run twice on each run – intra-assay reproducibility11
September 13, 201712NGS Results for 24 DBS SamplesMetricTruSeq (MiSeq)AmpliSeq (Torrent)Avg. Depth of Coverage661(211-884)586(247-789)# Variants called287(231-388)336(272-384)% Bases Called(met QC criteria)98.4%(93-98.8%)97.8%(95.1 - 98.3%)Both platforms provide good quality sequence data and adequatecoverage of the targeted region
September 13, 201713Platform Performance – Example RunTruSeq (MiSeq)Sample101102103104105106107107 2NA12878NA12878 lowAmpliSeq (Ion Torrent)%#%Avg#ng DNAUncalled ng DNA Avg Depth Variant UncalledDepth 281.81.81.91.82.01.81.71.71.71.8AmpliSeq appears somewhat more tolerant to low DNA concentration
September 13, 201714Accuracy – Reference Sample NA1287832731355810.96050.9999AmpliSeq(Ion Torrent) Both platforms demonstrated excellent sensitivity and specificity foridentification of variants in the reference sample Results were reproducible between runs
September 13, 2017158 Validation Samples – Confirmed Genetic CauseSampleGeneVariant(cDNA)Variant CHD7c.434G Ap.Trp145TerHet (dom)PathogenicYes105ADAc.301C Tp.Arg101TrpHomPathogenicYes108IL7Rc.83-2A T-HetVOUSIL7Rc.353G Ap.Cys118TyrHetPathogenic110IL2RGc.982C Tp.Arg328TerHomLikely PathogenicYes113IL2RGc.865C Tp.Arg289TerHomPathogenicYes115ADAc.301C Tp.Arg101TrpHomPathogenicYes116JAK3c.2872G Tp.Glu958TerHetLikely Pathogenicc.1261delCp.Leu421fsHetLikely Pathogenicc.501A Cp.Arg167SerHetVOUS120RAG2c.283G Ap.Gly95ArgHetPathogenicVariants filtered for pathogenic/likely pathogenic - homozygous or compoundheterozygote. VOUS unfiltered if 1 pathogenic/likely pathogenic.YesYesYes
September 13, 20171616 Validation Samples – Genetic Cause Known/Unknown* Genetic cause Trp522Cys;p.Arg778Trp114None103*ADAp.Pro297del (Hom)117None104None118ATMc.5763-1G A (Hom)106ADA119IL2RGp.Asp194Tyr Arg507Trp;p.Ser966Thr112*None124*IL2RGp.Leu272fs (Hom)p.Arg101Trp (Hom)p.Gly216Arg (Hom)Further analysis to be done: Sanger confirm all pathogenic/likely pathogenic/VOUS Re-assess potentially causative variants – 2 VOUS
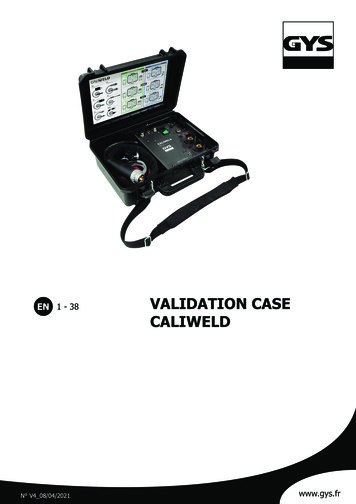
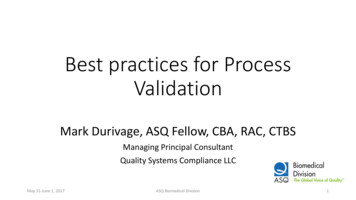
September 13, 2017DECoN17Sample 121Uses depth of coverage to copy number variantsSamples 109 and 112 also had low coverage for TBXThese 3 infants were reported asDiGeorge Syndrome(heterozygous deletion of TBX1)
September 13, 2017Summary TruSeq (MiSeq) and AmpliSeq (Ion Torrent) 39-gene SCID panels demonstrate similaraccuracy and reproducibility for detection of variants in the reference sample NA12878 Both panels detected known pathogenic variants in infants diagnosed with SCID Potential genetic causes were identified for infants diagnosed with an immunodeficiency forwhom we do not have genetic information.Next Steps Complete validation Sanger confirmations Sensitivity and Specificity of assay for dried blood spot samples Submit validation to NYS Clinical Laboratory Evaluation Program for approval Begin Consented Study18
September 13, 201719Proposed Testing Algorithm for SCIDT-cell receptor excision circle(TREC) assay 125 Avg. TRECsRefer to Specialist for Diagnostic TestingCBC, Flow cytometry, Mitogen studiesNBS NGS: 39-gene SCID panelImmunodeficiencyidentified:Informed Consent No Insurance issuesTAT ( 1 wk)Less stress on families
September 13, 201720Acknowledgments:NYS NBS Program:Michele Caggana, ScD, FACMGBob Sicko, BSAllison Madole, BSDenise Kay, PhDCarlos Saavedra, MDBeth Vogel, MS, CGCSarah Bradley, MS, CGCWadsworth Center AppliedGenomic Technologies Core
TruSeq Custom Amplicon (TSCA) panel. September 13, 2017 7. Illumina MiSeq. Specification. Ion Torrent S5. 10 ng. Recommended Minimum DNA Input. 1 ng. Paired-end reads. Sequence Reads. Single end reads. Ligation capture/amplification . Library Prep/ Gene Targeting. Multiplex PCR. Reversible terminator with fluorescent dNTPs. Sequence detection. Semiconductor based sequencing. Platform .