Transcription
Physician OrganizationGovernance:Transformation andThree Perspectives
IntroductionSpurred by the passage of the Affordable Care Act (ACA), the health care field has beenmoving forward in redefining what it means to be a hospital. In addition to expandingcoverage, the ACA also called for a number of pilot programs to redefine care delivery, allowingproviders to experiment and think more broadly about the move from volume to value-basedcare delivery. As the field moves toward more integrated and accountable care, existing silosand divisions will need to come down to allow for coordinated efforts to manage the healthof populations.The field’s vision of overall transformation includes all providers joining together to takeresponsibility for populations, better coordinate across care settings and providers, moreeffectively manage chronic disease, and take a greater role for primary care.To support the field in these transitions, the AHA isworking with the American Medical Association (AMA)to identify principles of integrated leadership. Theprinciples were released in 2015 and can be found he principles focus on the need to develop a structurewith collaborative and integrated leadership betweenclinicians and the hospital leadership. The principlesemphasize the need for physician and hospital leaderswith similar values and expectations, aligned incentivesand goals as well as shared responsibility for financial,cost and quality targets and a shared focus onengaging patients as partners in their care.Further, the principles call for an interdisciplinarystructure that supports collaborative decision-makingbetween physicians and hospital executives at all levelsof the integrated health system. This collaborative,2participatory partnership must be built on trust with asense of interdependence and working towards mutualachievement of the Triple Aim. That trust is developedby open and transparent sharing of information toimprove care and supported by a robust clinicalinformation system.To work effectively as partners in this type of model,more coordination between hospitals and clinicians isneeded, as well as greater organization of physiciansinto effective, accountable groups that can manage careacross the continuum. Key among the organizationalprinciples of a physician organization is an inclusivegovernance process that examines performance of thegroup, membership requirements, establishes leadershipand manages how resources are used. The group alsomust be able to create strategy, a future vision andhave resources underpinning them.
Governance of Physician OrganizationsKey Learnings and Gaps Identifiedin Physician GovernanceTo understand how the governance ofphysician-led organizations is different, andsimilar, to that of health care systems, theAHA’s Center for Healthcare Governanceand Physician Leadership Forum, withgenerous support from Hospira Inc.,undertook a study to examine governancestructures and functions in a diverse set ofphysician organizations—entities designed toengage physicians in the leadership,governance and decision-making of theclinical care enterprise. The resulting report,The Blue Ribbon Panel on Governance ofPhysician Organizations, examines howphysician organizations govern themselves,how they come together as groups and howthey impart the discipline and get theoutcomes they need to be successful.The study aimed to understand whatgovernance practices currently exist amongphysician groups. Thirty-one physicianleaders, executives and board members ofsix organizations were interviewed andshared their insights. The organizationsstudied included: Advocate PhysicianPartners, Downers Grove, Ill.; Billings Clinic,Billings, Mont., East Bay Physicians MedicalGroup, Lafayette, Calif.; Hill PhysiciansMedical Group, San Ramon, Calif.; HospitalSisters Medical Group, Springfield, Ill; andMemorial Hermann Physician Network(MHMD), Houston.In follow up to the report, the AHA convenedan educational session to share highlights ofthe study and provide an in-depth examinationfrom three leading-edge case studies.John R. Combes, M.D., chief medical officer and seniorvice president, American Hospital Association,welcomed session participants and set the stage forthe program by sharing the findings of The Blue RibbonPanel on Governance of Physician Organizations.As Dr. Combes explained, the study shows physicianorganization governance drives value for patients andhealth care organizations by championing a relentlessfocus on quality, safe, cost-effective care, fulfilling avision of providing the highest quality care and acommitment to being the best at delivering care.Governance can impede organizational success whenthere is a failure to engage in crucial conversations,being perceived as self-serving and failing to basedecisions on data and evidence.Challenges for physician organizations includetransitioning from fee-for-service to fixed payment,governance oversight and setting strategic direction inan environment with many unknowns, assumption ofclinical risk to drive assumption of financial risk, andlack of alignment and trust between physicianorganizations and hospitals and health systems.Additionally, difficulties arise due to lack of understandingof differences between governance and management asphysicians are often involved at both levels, lack ofdefinition of relative roles, responsibilities and authoritiesamong boards and management, such as who hires andfires the physician organization CEO, and lack of self-reflection on board capabilities to drive improved governance.Most of the study boards are structured with the keycommittees needed to achieve successful governanceoversight, appropriately dividing work between thecommittees and the board. However, committees werenot broadly used to diversify the board’s perspective,since most of the committees are composed of boardmembers rather than outside expertise. Finally, theboards often struggled to refrain from becomingoperational and getting involved in management matters.3
The organizations that took part in the studydemonstrated strong focus on quality and delivering safecare. Physician board members prepared for and activelyparticipated in meetings, and there was a willingnessto share dissenting opinions. Study participants alsoshowed strong investment in developing physicianleaders to assume governance roles.The nature of health care is changing. Boards mustmove beyond being only fiduciary responsibility, thinkdifferently and ask the generative questions such as‘what is our purpose?’ Leaders can change the focusof care across the system, recognizing it takespartnership of clinicians and executives to move towardpopulation health.Keynote: Governance Models in aTransforming Delivery SystemBased on the findings of The Blue Ribbon Panel onGovernance of Physician Organization supporting theneed for strong physician organization governance,JoAnn McNutt, Ph.D., Nygren Consulting, provided sixessential tools for effective governance of physicianorganizations.4needed expertise in clinical risk, quality and patientexperience to begin to address population health.As governance evolves, boards need to be able togovern themselves before they can govern anorganization. Until the board understands its roles andresponsibilities and what governance is, it will not beable to effectively govern an organization. To governwell, a board must determine what is working well, whatis not working well, and what can be done differently.The core responsibilities of the board has evolved inrecent years. Board governance used to consist of thehiring and firing of the CEO, financial oversight andstrategy. Responsibilities expanded to establishing andupholding the mission, vision and values, CEOsuccession and executive compensation. Enterpriserisk management, clinical risk, ethics and compliancealso have come under the board’s purview, and finally,quality, patient experience and population health.Dr. McNutt, an expert in board governance, firstdiscussed key themes in the transformation ofgovernance models. In her work, Dr. McNutt has seenan increase in mergers and acquisitions as well asaffiliations and partnerships that are creating largersystems of equals working together to effect change.According to Dr. McNutt’s observations, goodgovernance boils down to three things: what is done inthe board room, who is in the board room, and whathappens outside the board room. What gets done inthe board room is strategic oversight, financialoversight, policy setting, priority setting, decisionmaking, accountability and committee work. Whendetermining who is in the board room, organizationsneed to consider competencies and diversity—reflecting the community being served as well as themission, vision, values and strategy.These collaborations and affiliations are becomingmore common as the health care delivery environmentchanges, in part as a result of the ACA. As the fieldevolves, governance must grow and change to providethe best direction for new models. For organizations totruly address population health, they need to determinewhat the board’s work should consist of and define thekey roles and responsibilities.Once boards have determined what gets done in theboard room and who is present, high-performingboards are able to address what occurs outside of theboard room including: communicating with fellow boardmembers, management and stakeholders; buildingrelationships; maintaining confidentiality; managing crisis;being ambassadors of the organization; and developingleadership within the board and executive team.The mission, vision and values of an organizationinform the strategy for governance. Once the mission,vision and values have been identified as the work ofthe board, an organization needs to determine whatcompetencies are needed. Boards are looking forleaders with needed competencies who alsounderstand population health. Physicians can provideAs mergers and acquisitions, affiliations and partnershipshappen, confidentiality is especially important asinformation leaks can be problematic. Having a compactdefining roles and responsibilities and addressingconfidentiality can ensure the board acts as a unit. Inaddition, boards need to be intentional about how theyrelate to the executive team. With an effective process
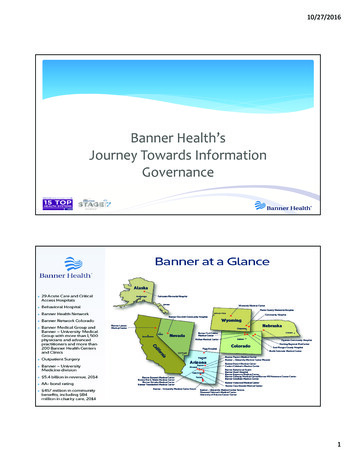
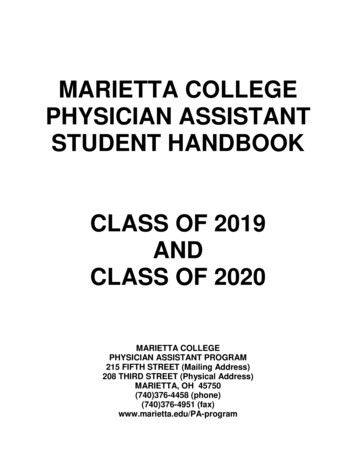
in place, board members can be deliberate about howthey ask the management team for information.Six Essential Tools for Effective Governance ofPhysician OrganizationsDr. McNutt provided six tools to create a high-performingeffective board; these are a strategic roadmap,authority matrix, decision-making policy guideline,board competency profile, director self- and peerassessment and a board member code of conduct.Strategic RoadmapA strategic roadmap, alternatively referred to as astrategic plan or direction, is a tool boards can use tobe clear about the vision, mission and purpose of theorganization. The vision, what an organization hopes tobe, needs to be audacious yet attainable.A strategy statement is typically internal and sets forthbenchmarks the organization wants to achieve within acertain time frame. Priorities are established based uponthe statement, distilling the strategy into external andinternal foci. Each area of focus has specific goals andoutcomes, as well as approaches and tactics, measuresand timelines. This tool provides a single page summary ofwhat the organization’s purpose is, what it does, and whatit strives to achieve. Everyone in the organization shouldbe able to see themselves in the summary. (Figure 1)Authority MatrixThe authority matrix addresses potentialmiscommunications by answering questions and clarifyingresponsibilities. It is important to capture all stakeholdersin the matrix, including the executive leadership team,committees, the board, a system board, and anyoneelse with an investment and interest in operations. Thedevelopment of the matrix will clarify authority andidentify exactly where decision-making occurs.The authority matrix includes the mission, vision, valuesand strategy as well as the major decisions the boardwill address. Policy decisions can be included as wellas finance and investment transactions.The process of completing the matrix throughdiscussion and debate allows all involved to participateand understand their roles. (Figure 2)Governing Through Policy SettingGood boards govern through policy setting. Policylevels may be broken down into major, secondary,functional, minor and standard operating procedure.Establishing levels at which decisions are made allowsboards to be more efficient. Knowing at what level amatter ought to be discussed can save the board timeand energy addressing an issue that should bedecided elsewhere. (Figure 3)Figure 1.5
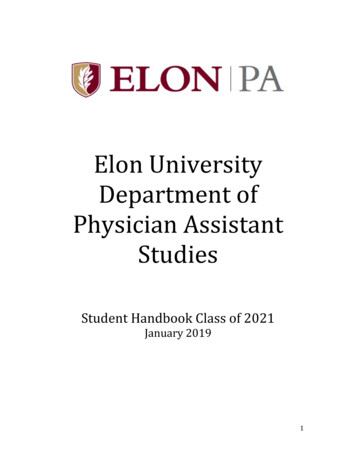
Figure 2.Board Competency ProfileA board competency profile is developed afterdetermining what the work of the board is, assessingwhat is needed to ensure good governance and whatcompetencies are needed. Competency profiles can becreated for the entire board or by specific committee.Usually handled by a governance committee, acompetency profile should assess whether collectivelythe board is strong in specific needed areas rather thanaddress individual competencies. (Figure 4)Director Self- and Peer-AssessmentSome organizations complete director self- andpeer-assessments annually utilizing results to driveimprovement. Others use assessments to determineboard members’ fitness for re-election. The assessmentcould be as simple as three questions: What is thisdirector’s most significant individual strength? What areareas for development? And, would you recommendthe director for re-nomination to the board?The goal of assessment is to ensure the right leadersare involved, are asking the right questions, andchallenging management to effectively fulfill themission, vision and values of the organization.6Board Member Code of Conduct(or Board Compact)A code of conduct, or compact, is a tool to setexpectations and clarify consequences. A board shouldbe proactive and govern by intention, not byconsequence. It is essential to establish board andcommittee participation in the compact. A compactalso can address confidentiality, information requests,communication, crisis management, ambassadorshipand education expectations. The board should haverobust conversations about what items the compactwill include. Some organizations have physician andmanagement compacts as well as board compacts,and some combine all three. For example, the boardmay promise management to ask for the rightinformation, and management may in turn promise toprovide effective analysis of data. Once in place, all ofthese tools need to become part of the board’sfunction and their performance assessed and improvedas needed. As a learning organization, the board mustlead the constant evolution to becoming a highperforming, effective board.
Figure 3.General Core Competencies for all Board MembersService ona Board ofDirectorsor BoardCommitteeDirectorScoresKnowledgein PhysicianIntegrationand CareIntegrationCommittee-Specific CompetenciesKnowledgein HealthcareAdvocacy,Public Policy,CommunityBenefitKnowledge/Experience inTechnologyand InformationSystemsKnowledge/Experience asa HealthcareProfessionalCompensationCompliance andAuditGovernanceQualityKnowledge/Experiencein ershipDevelopment,SuccessionPlanning, TalentManagementKnowledge/Experiencein ics, ExternalAuditKnowledge/Experiencein opmentKnowledge/Experiencein HealthcareQuality andPatient SafetyFinanceKnowledge/Experiencein ledge/Experience inInvestments,Philanthropy,Real .82.62.42.61.62.41.62.42.82.21.6OverallAverage rageRelativeStrengthAverageRelativeWeaknessFigure 4.7
Three Perspectives:Physician Organization GovernanceMemorial Hermann Physician Network(MHMD)partnership with Rice University to create a five-monthcertificate program for physicians and administrators.D. Keith Fernandez, M.D., former president andphysician-in-chief of MHMD, the Memorial HermannPhysician Network, and former chief medical officer ofthe Memorial Herman Accountable Care Organizationin Houston shared the MHMD governance model.Another critical component to the physician group’sperformance is the compact MHMD developed. Thecompact states that MHMD leadership agrees toprovide excellence, governance and transparency;accountability to collaborate with physicians to achievequality and efficiency goals; to demonstratecompassion and respect; to foster team spirit; and, tosupport innovation. Physicians, in turn, agree topractice evidence-based clinical care, be transparent,collaborate with MHHS to improve safety andefficiency, demonstrate compassion and respect topatients, other physicians and health careprofessionals, be accountable, function as a memberof the MHMD team, and support innovation. Thecompact is a tool with which to measure performanceand a means to hold one another accountable.Founded in 1982 and formerly known as MemorialHermann Health Network Providers, MHMD is aclinically integrated, for-profit, multispecialty,independent physician organization of more than 3,000doctors in the greater Houston area serving 350,000patients. It is the primary physician network forMemorial Hermann Healthcare System (MHHS) whichincludes 12 hospitals, 19 ambulatory surgery centersand an accountable care organization. MHMD iscomprised of private, independent primary care andspecialist physicians as well as physicians on the facultyof the University of Texas Medical School at Houston.MHMD originally had a small, non-elected board, themembers being the individuals who started theindependent physician association. Board membersbegan to be elected, but the board was dysfunctional,with everyone representing either their hospital orspecialty. Few accomplishments were achieved. Thisevolved into a representative board by medical staffsize, which was even less effective. Governance beganto improve once it became an appointed representativeboard. Currently, there are nine members nominated bymembership and each hospital campus medicalexecutive committee (MEC), and 13 who are appointedby the board. There is a board nominating committeethat screens all potential board members based ontheir qualifications.MHMD’s governance success has been due in largepart to education about governance and a physician’srole in governance, both of which are critical toestablishing a common vision. MHMD developed a8Holding one another accountable and trusting oneanother in decision-making is evident in delegation ofauthority. Each specialty and sub-specialty reports to aClinical Programs Committee (CPC), which then reportsto the board. The CPC is delegated authority from thesystem quality committee to put in place care protocolsacross the system. In addition, there are task-orientedcommittees, as well as five vendor committees thatnow run the supply chain for the health system. Morethan 400 physicians serve on these committees,attending 75 percent of the meetings. The CPCsconnect to the system board and the MECs.Another factor in the success of MHMD is the utilizationof data. Doctors meet every quarter to review theirquality and cost data. Physicians review reports forquality metrics, per-member, per-month scorecards,outlier reports as well as patient and physician profiles.Data and rankings are shared unblinded, which fostersunity and cohesiveness across the physician community.Resources are available to facilitate improvement.
Good governance is critical and can be expanded froma board to specialties, sub-specialties and supplychains. Empowering physicians as part of governanceallows them to understand how to deliver on the TripleAim of better health, better health care and lower cost.Billings ClinicJ. Scott Millikan, M.D. is a practicing cardiovascularsurgeon at Billings Clinic, Billings, Mont. where he hasbeen an active leader for many years, serving as amember of the Board of Directors since 2005. Dr.Millikan recently completed a term as chairman of theboard of directors and is now chairman of theDepartment of Cardiac, Thoracic and Vascular Surgery.Dr. Millikan described the governance journey atBillings Clinic as one of going from a private multispecialty group practice to a fully integrated health caresystem. Along the way, physician leadership has beenencouraged and important lessons have been learned.Billings Clinic was founded in 1917. The hospital thatBillings Clinic eventually integrated with, BillingsDeaconess Hospital, was built in 1927. In 1989 theBillings Clinic partnership was 90 physicians, representing85 percent of the admissions to Deaconess MedicalCenter. Merger discussions began in 1989 and eventuallythe two merged in 1993. The merger happened becausethe physician group needed capital and incomestabilization while the hospital was worried the grouppractice might move services out of the hospital. Therewere infrastructure inefficiencies and a need tominimize duplication of services. Upon merging, thevision and culture were established. Once merged, theparent board was formed, but the hospital and clinicwere maintained as separate business entities.At the time of the merger, rather than a single CEO,responsibilities were shared between the hospital CEO,a clinic physician CEO and an administrative manager.This leadership approach had its challenges andultimately was changed. The board also started as amerged entity with a lack of clear direction andexpectations. Divisions between hospital and physicianmembers of the board and differing expectations andperceptions became clear. Physicians thought themerger was a partnership and a chance to embark on9
a new relationship similar to Virginia Mason Clinic orMayo Clinic. Many on the hospital side viewed it as anacquisition of a group practice.These differing ideas ended with mediation.Management was changed to a co-CEO model for atime. In 1997, Billings moved to a single CEO andsingle unified budget. Comparisons and infighting werecurtailed and the work of building a unified board andvision began.Over time, Billings Clinic has become financially stable,and physician recruitment has improved with significantinvestment in physician leadership development.Centers of Excellence have been developed, as well asa greater regional strategy, operating plan, balancedscorecard and market share movement.Billings Clinic is a medical foundation model. There is aBillings Clinic board and a charitable foundation board.There are 12 members on the community-based board.It is representational in that two physician positions areelected by the physician body. Physicians serving on10the board, though, are not there to represent physicians,but provide a medical perspective. There are alsonurses on the board who are not employed by thehospital or health system.Many believe that physicians can’t help but representtheir own self-interest. Billings Clinic has proved thisstatement to be false. The board looks to thephysicians for clinical expertise and understanding ofthe functions of care delivery and feels that havingphysicians on the board is very beneficial.The CEO also sits on the board, and is a physician.The bylaws state that the CEO must be a physician.An operating council was established, called theLeadership Council. The Leadership Council consistsof seven physicians who are elected by the physicianbody and seven administrators. Three of the sevenadministrators are also physicians, the CMO of thehospital, the CMO of the clinic and the chief qualityofficer. There is a close relationship between theLeadership Council and board. The Leadership Council
members often attend board meetings. Feeding intothe Leadership Council are several committees onresearch, continuing care, post-acute care, grouppractice, the hospital and then a newer committeelooking at regional affiliations throughout Montana,Wyoming and the Dakotas.Several years ago management, along with the board,developed cornerstone principles which state thatBillings Clinic is, “at its core, a multispecialty physiciangroup practice, where a community of physicians workin a collegial manner to coordinate health care acrossa spectrum of services. We are a physician-ledorganization with a physician CEO, and physicians atall levels of leadership in the organization ” BillingsClinic values partnership among physicians, nurses,clinical and support staff and includes physicians in alllevels of decision-making. A not-for-profit communitygoverned organization, Billings Clinic has an obsessivededication to patient safety, quality, service and value.This culture of safety, quality, service and value isenhanced by strong physician leadership. The BillingsClinic board has come to understand that physicianscan be high-quality leaders, extremely visionary, andcommitted to a higher purpose. Physician leadershipdevelopment has a very high return on investment forBillings Clinic.Billings Clinic has found success in partnering thosephysician leaders with hospital managers in dyads.Physician-manager dyads can work very well togetherand provide great synergy of purpose. Physicians wantto be partners with management in delivering excellent,highly reliable, high-quality care. Physicians want to beentrusted and want to trust as well.East Bay Physicians Medical Group Inc.Affiliated with Sutter East Bay Medical FoundationSamuel Santoro, D.O. was named president and chiefexecutive officer of East Bay Physicians Medical Group,Lafayette, Calif., affiliated with Sutter East Bay MedicalFoundation, in 2011. As such, Dr. Santoro has helpedguide the rapid growth and development of East BayPhysicians Medical Group, a multi-specialty medicalgroup consisting of more than 300 clinicians.In Dr. Santoro’s experience, physicians, advancedpractice clinicians, staff, nurses, and administrators allwant to perform excellently, take care of their patientsand govern the organization well. The reality though, isthat governance has not traditionally been a focus oftraining for physicians. Understanding the importanceof governance education not just as an individual, butas a board is essential.East Bay Physicians Medical Group is a medicalfoundation model, part of Sutter Health, the 11thlargest not-for-profit integrated health system in theUnited States, with over 5,000 physicians, about half ofwhich are in independent practice associations, theother half are organized in multispecialty groups. Thereare 24 affiliated not-for-profit hospitals within the SutterHealth system, with about 10.5 billion in revenues,and many, many components. East Bay PhysiciansMedical Group, exclusively contracted with Sutter EastBay Medical Foundation, has nine different outpatientcare centers, and supports three major Sutter inpatientfacilities covering five campuses. The medical groupexists to employ and benefit clinicians.Physician leadership has poised Billings Clinic for thefuture. ACO models are being developed, as well asnew payment methodologies, evolving financialincentives, and a more competitive landscape. BillingsClinic is well set to move forward, mostly due to thework done to integrate physicians in management andgovernance.The board at Billings Clinic views physicians as a vitalpart of the organization, to be engaged and considereda partner to move care delivery forward.11
In 2005, the medical group consisted of 43 members,over half of whom were hospitalists. Today, there aremore than 300 clinicians. Not all specialties arerepresented, but there has been tremendous growth.Currently 55 percent of the group is primary care while45 percent is specialty care.The board of directors consists of 12 shareholdermembers with an executive committee and fivesubcommittees, the most important being quality andpeer review. Built out of the quality and peer reviewcommittee are credentialing, risk and best practicequality enhancement, pharmacy and therapeutics,electronic health records and the well-being committee.Each of the five subcommittees is chaired by a directorof the board. Members of the finance and compensationcommittees must be shareholders in order to vote. The12governance committee is very important, and a lot oftime has been spent on developing and honing thenomination process to ensure a strong pipeline of leaders.The other committees, such as pension and communitybenefit, do not require a board member to be the chair,nor do they necessarily require committee membersbe a shareholder of the group. These committees,then, serve as a training ground for members to betterunderstand the group and potentially, a means ofidentifying future leaders, particularly for the boardof directors.In 2010, the original East Bay Physicians Medical Groupleadership focused on acquiring physician practiceswhich quickly deteriorated as a strategy. The boardwas forced to take drastic actions including terminatingthe medical group CEO to stem the tide. This was a
bold step for the board, but not part of a consideredplan of action. Fortunately, the board recognized thatthey needed help and brought in a board consultantwho continues to assist. From that point on, the boardhad focus. The first order of business was to find apresident and CEO for the group. The president andCEO is an ex officio voting member of the board, butis not the chair, a key decision.The second, but equally important, task for the boardwas to decide what East Bay Physicians MedicalGroup would be and what they would be about. At thistime, the leadership of the medical foundation was indisarray,
AHA's Center for Healthcare Governance and Physician Leadership Forum, with generous support from Hospira Inc., undertook a study to examine governance structures and functions in a diverse set of physician organizations—entities designed to engage physicians in the leadership, governance and decision-making of the clinical care enterprise.