Transcription
10/11/2017Pharmacotherapy UpdateMultiple SclerosisYolande HanssensSIG Leader Medicine InformationHamad Medical CorporationPharmacy Department - Clinical Service UnitDoha - QatarHeidelberg/October 2017Pharmacotherapy UpdateMultiple Sclerosis Introduction Classification Therapeutic management of RRMS*Disease Modifying Drugs (DMDs)Patient tailored treatmentSpecial patient groups Summary & take home messages*RRMS Relapsing Remitting Multiple Sclerosis1
10/11/2017MS - Intro Progressive, chronic idiopathic autoimmune drivendisorder of the nervous system widespread inflammation affecting the brainand spinal cord plaques (MRI) Unpredictable Symptomsfrom numbness and tingling to blindness andparalysis Age 20-50, M:2F, genetic factors? North Europeans? 2.3 million No cureMS – Classification Relapsing-Remitting MS (RRMS)About 85% Secondary-Progressive MS (SPMS)Symptoms worsen more steadily over time, with or withoutthe occurrence of relapses and remissions.RRMS SPMS at some point Primary-Progressive MS (PPMS)About 10%slowly worsening symptoms from the beginning, with norelapses or remissions Progressive-Relapsing MS (PRMS)About 5%steadily worsening disease state from the beginning, withacute relapses but no remissions, with or without recoveryHooper K. Managing Progressive MS. New York, NY: National Multiple Sclerosis Society; 2011.Multiple Sclerosis: Just the Facts New York, NY; National Multiple Sclerosis Society; 2011.2
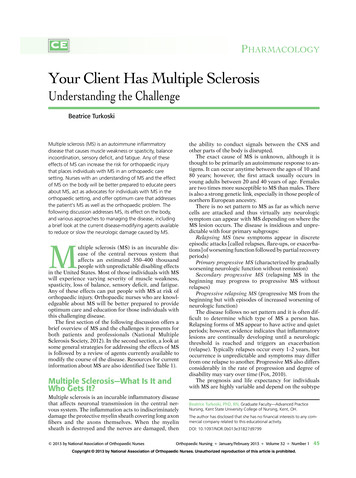
10/11/2017Types of MS at DiagnosisMS International Federation; www.msif.orgClinical EvolutionTIMEWINDOWtoSTARTTREATMENTRIS Radiological Isolated SyndromeCIS Clinical Isolated SyndromeRRMS Relapsing Remitting MSR-SPMS Relapsing Secondary Progressive MSSPMS Secondary Progressive MS3
10/11/2017Therapeutic Management No Cure DMDs for RRMS Mode of Action & Major Adverse Events Documented Treatment Effects Patient Tailored Therapy Special Patient groups& Overall Pharmaceutical Care ConsiderationsDMD Disease modifying DrugRRMS Relapsing Remitting MSOcreluzimabi.v. 2017EDDS Expanded Disability Status ScaleMSFC Multiple Sclerosis Functional CompositeNEDA No Evidence of Disease Activity4
10/11/2017DMDs for RRMS Interferon β (Rebif , Betaseron , Avonex , Plegridy )Glatiramer acetate (Copaxone )Teriflunomide (Aubagio )Dimethyl fumarate (Tecfidera )Fingolimod (Gilenya )Natalizumab (Tysabri )Alemtuzumab (Lemtrada )Ocrelizumab (Ocrevus )DMD Disease modifying DrugRRMS Relapsing Remitting MSInterferon β MOA - unknown (PEG)Interferon Beta-1aIM (Avonex ) & SubQ (Rebif , Plegridy )Chinese hamster ovary cells Interferon Beta-1bSubQ (Betaseron )E coli5
10/11/2017Interferon β - ConcernsRelated to adverse effects Anaphylaxis/hypersensitivity reactions Autoimmune disorders Bone marrow suppression Flu-like symptoms Hepatic effects obtain liver function tests at 1, 3, and 6 months posttherapy initiation and periodically thereafter. Injection site reactions Neuropsychiatric disorders Thrombotic microangiopathyGlatiramer Acetate MOA - thought to induce and activate T-lymphocytesuppressor cells specific for a myelin antigen & tointerfere with the antigen-presenting function ofcertain immune cells opposing pathogenic T-cellfunction SubQ - 20 mg once daily OR 40 mg 3x/week6
10/11/2017Glatiramer - ConcernsRelated to adverse effects Hypersensitivity reactionsImmune responseLipoatrophy including skin necrosisSystemic reactions anxiety, chest pain, constriction of the throat,dyspnea, flushing, palpitations, urticaria usually self-limited and transient generally occur several months after initiation oftreatment.Teriflunomide MOA - immunomodulatory agent that inhibitspyrimidine synthesis, resulting in antiproliferative and anti-inflammatory effects- may reduce the number of activatedlymphocytes in the CNS PO – 7 to 14 mg once daily7
10/11/2017Teriflunomide - ConcernsRelated to adverse effects Dermatologic reactions: Cases of serious skin reactions, includingcases of Stevens-Johnson syndrome and fatal toxicepidermal necrolysis have been reported with teriflunomide Hepatotoxicity - [US Boxed Warning] Hypersensitivity reactions - Anaphylaxis and severe allergicreactions may occur Hypertension Infections Interstitial lung disease Malignancy Pancreatitis Peripheral neuropathy Renal effects - Transient acute renal failureTeriflunomide - ConcernsOther Drug elimination procedure - up to 2 years toreach low levels of teriflunomide metabolite serumconcentrations. drug elimination procedure using cholestyramineor activated charcoal for more rapid eliminationBUT return of disease activity Teriflunomide is also found in semen Immunizations - before initiating therapy8
10/11/2017Dimethyl fumarate MOA - believed to result from its anti-inflammatoryand cytoprotective properties via activation of theNrf2* pathway PO – 120 mg BID; after 7 days to 240 mg BID*Nrf2 nuclear factor (erythroid-derived 2)-like 2Dimethyl fumarate - ConcernsRelated to adverse effects Dermatitis/irritation Flushing Gastrointestinal events Hepatotoxicity Hypersensitivity reactions- Anaphylaxis and angioedema may occurafter the first dose or at any time during treatment Lymphopenia Proteinuria Progressive multifocal leukoencephalopathy (PML) -9
10/11/2017Dimethyl fumarate - ConcernsRelated to adverse effects Dermatitis/irritationFlushingGastrointestinal eventsHepatotoxicityHypersensitivity reactionsLymphopeniaProteinuria Progressive multifocal leukoencephalopathy (PML)associated with persistent ( 6 months) lymphopenia, witha majority of cases occurring in patients with lymphocytecounts 500/mm3 and anti-JCV (John Cunningham virus)antibody 0.9 withhold therapy immediately at the first sign orsymptom suggestive of PML (eg, progressive weakness onone side of the body or clumsiness of limbs; visiondisturbances; mental status changes) and perform adiagnostic evaluation (MRI findings may appear beforeclinical signs/symptoms).Fingolimod MOA – Sphingosine 1-Phosphate (S1P) Receptor Modulator;blocks the lymphocytes' ability to emerge from lymph nodes the amount of lymphocytes available to the centralnervous system is decreased reduces central inflammation. PO – 0.5 mg PO once daily10
10/11/2017Fingolimod- ConcernsRelated to adverse effects Atrioventricular (AV) blockBradycardiaCryptococcal infectionsHepatic effectsHerpes infectionHypersensitivity reactionHypertensionImmune suppressionMacular edemaMalignancyNeurotoxicityProgressive multifocal leukoencephalopathy (PML)Respiratory effectsQT prolongationFingolimod- ConcernsOther specific warnings/precautionsDiscontinuation of therapy rebound syndrome may occur within 4 to 16 weeks of stopping fingolimod treatment in patients with multiple sclerosis of varying severity and duration relapses have occurred despite the initiation of other diseasemodifying therapies Rebound symptoms:back and extremity pain,confusion, constipation, diplopia,facial muscle spasms, fatigue,increased leg weakness, nausea,paraparesis and paresthesias11
10/11/2017NatalizumabAlemtuzumabOcrelizumab Monoclonal Antibodies with different MOA IV with different treatment schedules Natalizumab : 300 mg every 4 weeks Alemtuzumab : 12 mg daily for 5 consecutive days (total 60mg), followed 12 months later by 12 mg daily for 3 consecutivedays (total 36 mg); total duration of therapy: 24 months Ocrelizumab : 300 mg on day 1, 300 mg 2 weeks later and600 mg once every 6 monthsNatalizumabAlemtuzumabOcrelizumab Monoclonal Antibodies with different MOA Need for pre-medication methylprednisolone (1000 mg IV) 30 minutes prior to eachinfusion an antihistamine (eg, diphenhydramine) 30 to 60 minutes prioreach infusion may also consider premedication with paracetamol assess for infection; delay administration for active infection monitor patient during (and after) infusion12
10/11/2017Natalizumab, AlemtuzumabOcrelizumab - ConcernsRelated to adverse effects HepatotoxicityHerpes infection & other infectionsHep B reactivationsHypersensitivity reaction/antibody formationImmune reconstitution inflammatory syndrome (IRIS)MalignancyLab test abnormalitiesProgressive multifocal leukoencephalopathy (PML)Auto-Immune effectsBone marrow suppressionGI toxicityOcreluzimabi.v. 2017EDDS Expanded Disability Status ScaleMSFC Multiple Sclerosis Functional CompositeNEDA No Evidence of Disease Activity13
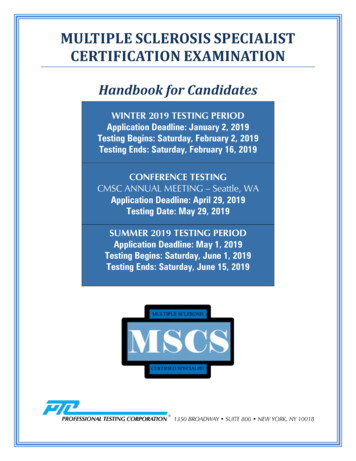
10/11/2017Overview of the efficacy of MS therapies currentlyavailable: NEDA# at 2 yearsTrialStudy drugOPERA I1***Ocrelizumab% patientsachievingNEDA#48sc IFN β-1a% patientsachievingNEDA#29OPERA II1***Ocrelizumab48sc IFN β-1a25CARE-MS I2*Alemtuzumab39sc IFN ingolimod33Placebo13CARE-MS II5***Alemtuzumab32sc IFN β-1a14ComparatorDEFINE6*Dimethyl o14.3Data cannot be directly compared between trials because of different study designs and/or populationsP-value study drug vs comparator; * 0.05; ** 0.001; *** 0.0001.1. Traboulsee A et al. Neurology 2016;86 [PL02.004]; 2. Cohen AJ et al. Lancet 2012;380:1819–28; 3. Havrdova E et al. Lancet Neurol 2009;8:254‒60;4. Bevan CJ, Cree BAC. JAMA Neurol 2014;71:269‒70; 5. Coles AJ et al. Lancet 2012;380:1829–39; 6. Giovannoni G et al. Neurology 2012;78[PD5.005]; 7. Freedman M et al. Neurology 2012;78 [PD5.007]#NEDA No Evidence of Disease Activity14
10/11/2017Comi G, Radaelli M, Soelberg Sorensen P. Lancet 2017;389: 1347-56.15
10/11/2017Switching Therapy &Wash-OutPeriods Required for Treatment Switch in MS PatientsTreatment 1Treatment 2Wash-OutIFN1 or GA2Any DrugNo wash-out requiredAny DrugIFN or GANo wash-out mabaccelerated eliminationprocedureor 3.5 monthsDimethyl FumarateFingolimodNatalizumabAlemtuzumabuntil lymphocyteslevel returnsto normal buntil lymphocyteslevel returns tonormal levels(1 to 2months)NatalizumabFingolimodTeriflunomideDimethyl Fumarate1-3 months1IFN Interferon; 2GA Glatiramer AcetateMichel L, et al. Update on treatments in multiple sclerosis. Presse Med. 201516
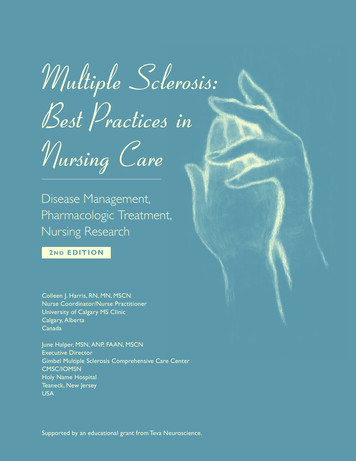
10/11/2017Treatment decisions for RRMS are multifactorial: Need for Systematic ApproachPatient &Disease ProfileTherapy Issues Age, gender, family statusDisease activity/disease typeStage of diseaseTreatment historyComorbidities & concurrent treatment EfficacySafetyTolerabilityAdministration (route/frequency)Monitoring requirements & frequencyof monitoringFemale Pregnancy LactationSharedDecision&PatientTailoredTreatment Sociodemographic profile (lifestyle,work status, family status) Convenience Risk tolerance Likelihood of adherencePatientPreferences Access to medication Approved usage CostGeographic &Economic FactorsMS & PregnancyEffects of pregnancy on MS Rate of relapse especially during 3rdtrimester Rate of relapses in first 3 months postpartumBefore0.71st Trim 2nd Trim 3rd Trim0.50.60.21st 3 months post1.2Confavreux C et al. NEJM. 1998:285-91Vukusic S et al. Brain. 2004:1353-6017
10/11/2017MS & PregnancyEffects of pregnancy on MSNo acceleration in the rate of disability ordisease progression postpartumEpidural anesthesiaBreastfeedingNo adverse eventon rate of relapseor progression ofMSConfavreux C et al. NEJM. 1998:285-91Vukusic S et al. Brain. 2004:1353-60MS & PregnancyMS does not seem to impair fertilityEffect of Assisted ReproductiveTechnology (ART)? risk of MS disease activity? Roles of extra hormones (GnRH agonist, FSH,progesterone) or rapid changes in hormone levelsHellwig K, Correale. J Clin Immunol. 2013:219-24Correale J et al. Ann Neurol. 2012:682-94Voskuhl RR. Ann Neurol. 2012:63118
10/11/2017MS & PregnancyEffect of MS on Pregnancy Outcomes rate of caesarian deliveryLower infant birth weightNo incomplicationsectopic pregnanciesbirth defectsspontaneous abortionsMS in offspring : 2.5% (single MS) vs30.5% (dual MS)Kelly VM et al. Neurology. 2009:1831-6Dahl J et al. Neurology. 2005:1961-3Mueller BA et al. Am J Obstet Gynecol. 2002:446-52Ebers G. Lancet Neurol. 2008:268-77MS & PregnancyTreatment of RRMS during Pregnancy To stop or NOT to stop? Washout periodDMDWashout periodGlatiramer acetatenoneInterferonszero to one monthDimethyl fumaratezero to one monthNatalizumabone to three monthsFingolimodtwo monthsAlemtuzumabthree to four monthsTeriflunomide*washout protocol using po cholestyramine oractivated charcoal ( 0.02mg/ml)*Also found in semen19
10/11/2017Safety during pregnancy of drugsused to treat RRMSCategory B - No evidence of human risk in controlled studiesGlatiramer acetateCategory C - Risk cannot be ruled outAlemtuzumabDimethyl fumarateFingolimodInterferon beta-1a (Avonex , Rebif )Interferon beta-1b (Betaseron )NatalizumabCategory X - Contraindicated in pregnancyTeriflunomideModified from: Damek DM, Shuster EA, Mayo Clin Proc 1997; 72:977(UptoDate-SEP2017)MS & BreastfeedingEffect of breastfeeding on MS NoneEffect of MS on breastfeeding Meds!Interferon β and glatiramer acetate “OK”?Others to avoidCoyle PK. Continuum (Minneap Minn). 2014:42-59Hale TW et al. Breastfeed Med. 2012:123-520
10/11/2017Conclusions Management of patients with MS/RRMS is very complex Early treatment influences the course over time There is a clear difference in safety profile among thecurrent DMDs The risk-benefit ratio needs to beindividualized Baseline assessment and monitoring are required formost of the DMDs in MS Teratogenicity & carcinogenicity are important factors inthe choice of DMD Cost 21
Injection site reactions Neuropsychiatric disorders Thrombotic microangiopathy Glatiramer Acetate MOA-thought to induce and activate T-lymphocyte suppressor cells specific for a myelin antigen & to interfere with the antigen-presenting function of certain immune cells opposing pathogenic T-cell function