Transcription
Diagnostic Guide forFetal Alcohol Syndromeand Related ConditionsThe 4-Digit Diagnostic CodeSecond EditionFAS Diagnostic andPrevention NetworkUniversity of WashingtonJanuary 1999
Diagnostic Guide for FAS and Related ConditionsDiagnostic Guide for Fetal Alcohol Syndrome and Related Conditions: The 4-Digit Diagnostic Code,2nd Edition 1999.Susan J. Astley, Ph.D.Associate Professor of Epidemiology / PediatricsSchool of Public Health and Community MedicineSchool of MedicineSterling K. Clarren, M.D.Robert A. Aldrich Professor of PediatricsSchool of MedicineUniversity of WashingtonSeattle, Washington, 98195Copyright 1999University of WashingtonSeattle, WA 98195, U.S.A.All rights reserved. This guide is protected by copyright. No part of this guide may be reproduced inany format or by any means, including photocopying, or utilized by any information storage andretrieval system without written permission from the copyright owner.Guide99.doc (6/9/99)To obtain additional copies of this manual please contact:Fetal Alcohol Syndrome Diagnostic and Prevention NetworkChildren's Hospital and Regional Medical Center4800 Sand Point Way N.E., CH-47Seattle, WA 98105http://depts.washington.edu/fasdpnUniversity of Washington, FAS Diagnostic & Prevention Network
Diagnostic Guide for FAS and Related ConditionsContentsContents .iAcknowledgments.iiPreface.iiiI.Introduction .1II.FAS Diagnostic Evaluation Form .5III.Instructions for use of the FAS Diagnostic Evaluation Form.17A. The 4-Digit Diagnostic Code.17B. 1. Scoring Growth .212. Scoring Facial Phenotype.253. Scoring Brain Function .314. Scoring Alcohol Exposure .355. Scoring Co-morbidities .37IV.Diagnostic Categories (n 22).39V.4-Digit Diagnostic Codes within each Diagnostic Category .41VI.4-Digit Diagnostic Codes sorted numerically (n 256).45VII.Clinical summaries for each of the 22 Diagnostic Categories.51VIII.Reference Charts of Normal Growth .75IX.Citations .95X.Appendices .971. New Patient Information Form .992. FAS-Tutor CD-ROM .111University of Washington, FAS Diagnostic & Prevention Networki
Diagnostic Guide for FAS and Related ConditionsAcknowledgmentsThe development of this Guide was supported in part by the following agencies and contributors:Centers for Disease Control and PreventionCenter on Human Development and Disability at the University of WashingtonDivision of Alcohol and Substance Abuse,Washington State Department of Social and Health ServicesMarch of Dimes Birth Defects FoundationJohn B. Chavez FAS FundWe wish to acknowledge our colleagues Diane Bailey, R.N., M.S.N., Pediatric Nurse Practitioner,Sharon Beck, M.Ed., Educational Counselor, Heather Carmichael Olson, Ph.D., DevelopmentalPsychologist, Sandra G. B. Clarren, Ph.D., Educational Psychologist, Truman Coggins, Ph.D.,Language Pathologist, Julie Gelo, Family Advocate, Tracy Jirikowic, MS, OTR/L OccupationalTherapist and Tina Talbot, M.S.W., Social Worker who use this Guide weekly and have helped us tohone the material on an ongoing basis. Their helpful criticism and thoughtful insights have beeninvaluable. We also wish to thank Kathleen Tharp, Kathy Briggs-Jones and Heather Grigg B.A. whoreadily offered their assistance when needed. Finally, a very special thanks is extended to all of ourpatients and their families who have contributed a wealth of knowledge and information to thedevelopment of this guide.iiUniversity of Washington, FAS Diagnostic & Prevention Network
Diagnostic Guide for FAS and Related ConditionsPrefaceThis Diagnostic Guide is the second edition. Based on our own experience and feedback from others,we continue to make modifications that enhance accuracy, improve clarity, and increase ease ofusage. We hope you will find this new approach to the diagnosis of individuals with fetal alcoholexposure helpful and broadly applicable.University of Washington, FAS Diagnostic & Prevention Networkiii
Diagnostic Guide for FAS and Related ConditionsIntroduction, Section II. IntroductionFetal alcohol syndrome (FAS).FAS is a permanent birth defect syndrome caused by maternal consumption of alcohol duringpregnancy. The definition of the fetal alcohol syndrome has changed little since the 1970’s when thecondition was first described and refined 1,2,3,4. The condition has been broadly characterized by preand/or postnatal growth deficiency, a characteristic set of minor facial anomalies, and evidence ofprenatal alteration in brain function such as microcephaly from birth, neurologic problems withoutpostnatal antecedents, or complex patterns of functional disability.The difficulty with diagnosing FAS and other disabilities associated with in uteroalcohol exposure.For the trained clinician, dysmorphologist, or clinical geneticist there is little difficulty in making thediagnosis of FAS when the typical anomalies in growth, face, and brain are all extreme and thealcohol exposure is conclusive and substantial. But the physical, cognitive and behavioral features arenot dichotomous, that is either normal or clearly abnormal. Rather, the features, and indeed thehistory of alcohol exposure, all range along separate continua from normal to clearly abnormal anddistinctive.In the absence of accurate, reproducible and unbiased methods for measuring and recording theseverity of exposure and outcome in individual patients, diagnoses will continue to vary widely fromclinic to clinic. From a clinical perspective, diagnostic misclassification leads to inappropriate patientcare, increased risk for secondary disabilities5 and missed opportunities to achieve prevention. Froma public health perspective, diagnostic misclassification leads to inaccurate estimates of incidence andprevalence. Inaccurate estimates thwart efforts to allocate sufficient social and health care services tothis high-risk population and preclude accurate assessment of primary prevention intervention efforts.From a clinical research perspective, diagnostic misclassification reduces the power to identifybetween-group contrasts within studies. Non-standardized diagnostic methods limit the ability tocompare outcomes between studies.The primary limitations in the current practice of diagnosing individuals with prenatal alcoholexposure include:1. There is no standardized clinical definition of FAS. Rather, there are diagnostic guidelines thatphysicians and medical researchers are encouraged to follow, but the guidelines are notsufficiently specific to assure diagnostic accuracy or precision.According to the latest proposed diagnostic guidelines published by Sokol and Clarren3 which area minor modification of the 1980 definition of FAS by the Fetal Alcohol Study Group of theResearch Society for Alcoholism 6:University of Washington, FAS Diagnostic & Prevention Network1
Introduction, Section IDiagnostic Guide for FAS and Related Conditions“The diagnosis of FAS can only be made when the patient has signs of abnormality in each ofthe three categories: 1) Prenatal and/or postnatal growth retardation (weight and/or lengthbelow the 10th percentile when corrected for gestational age), 2) central nervous systeminvolvement (including neurological abnormality, developmental delay, behavioral dysfunctionor deficit, intellectual impairment and/or structural abnormalities, such as microcephaly (headcircumference below the 3rd percentile) or brain malformations found on imaging studies orautopsy and 3) a characteristic face, currently qualitatively described as including shortpalpebral fissures, an elongated midface, a long and flattened philtrum, thin upper lip, andflattened maxilla.”Although these descriptions do provide guidance, they are not sufficiently specific to assurediagnostic accuracy and precision. The guidelines for CNS dysfunction do not address how manyareas of deficit must be present, how severe the deficits must be or what level of documentationmust exist to substantiate the presence of the deficit (i.e., parental history, psychometric testing orstructural imaging). The guidelines for the facial phenotype are equally nonspecific. How manyfacial features must be present, how severe must the features be and what scale of measurementshould be used to judge their severity? One need only read the clinical literature or reviewmedical records, birth certificates, birth defect registries or ICD-9 codes to see how variably thesecriteria are interpreted, applied and reported 7,8,9,10,11.2. There is a lack of objective, quantitative scales to measure and report the magnitude of expressionof key diagnostic features.For example, although a thin upper lip and smooth philtrum are key diagnostic features12,quantitative measurement scales have never been used to measure thinness or smoothness andguidelines have never been established for how thin or smooth the features must be. Objectivequantitative scales would not only improve accuracy and precision, but would also establish acommon descriptive language for communicating outcomes in medical records and the medicalliterature.3. The term FAS fails to convey the diversity of disability present in individuals with FAS.No two individuals with FAS present with the same constellation of anomalies and disabilities.Growth, facial phenotype, CNS dysfunction and alcohol exposure all vary along separatecontinua. The term FAS only conveys that the condition is permanent and was caused by prenatalalcohol exposure. The term does not convey what the individual’s disabilities are. Anomenclature that better conveys the diversity of outcomes among individuals with prenatalexposure would benefit both the patient’s caregivers and their medical/social/educational carenetwork.4. The term fetal alcohol effects (FAE) is broadly used and poorly defined.The term ‘suspected fetal alcohol effects’ was first introduced into the medical literature in 1978and was defined as ‘less complete partial expressions’ of FAS in individuals with prenatal alcoholexposure2. Based on this definition, an individual whose mother drank a few glasses of wine2University of Washington, FAS Diagnostic & Prevention Network
Diagnostic Guide for FAS and Related ConditionsIntroduction, Section Iintermittently throughout pregnancy and presented with attention deficit hyperactivity disorderwould be diagnosed FAE. So would an individual whose mother drank a fifth of vodka dailythroughout pregnancy and presented with microcephaly, severe mental retardation, cleft palateand severe growth deficiency. The broad use of this term and the reluctance to abandon it pointsto the clear need to develop diagnostic terms for individuals with prenatal alcohol exposure whopresent with physical anomalies and/or cognitive/behavioral disabilities, but do not have FAS.New diagnostic terms, which more finely differentiate the variable exposures and outcomes ofthese individuals without implying alcohol as the sole causal agent, are needed.5. Clinical terms like FAE13, alcohol related birth defects (ARBD)4 and alcohol relatedneurodevelopmental disorder (ARND)4 inappropriately imply a causal link between exposure andoutcome in a given individual. Leading dysmorphologists in the field of FAS diagnosis haveformally requested that the term FAE no longer be used for this reason13.With the likely exception of the facial phenotype, no other physical anomalies orcognitive/behavioral disabilities observed in an individual with prenatal alcohol exposure arenecessarily specific to (caused only by) their prenatal alcohol exposure. Features such asmicrocephaly, neurological abnormalities, attention deficit, mental retardation and growthdeficiency often occur in individuals with prenatal alcohol exposure, but also often occur inindividuals with no prenatal alcohol exposure.A new approach to diagnosis.Each of the above limitations has been overcome with the development the "4-Digit DiagnosticCode" introduced in this guide. The four digits reflect the magnitude of expression of four keydiagnostic features of FAS in the following order: (1) growth deficiency, (2) the FAS facialphenotype, (3) brain dysfunction, and (4) gestational alcohol exposure. The magnitude of expressionof each feature is ranked independently on a 4-point Likert scale with 1 reflecting complete absenceof the FAS feature and 4 reflecting a strong "classic" presence of the FAS feature.Benefits of the new diagnostic approach.This new approach:1. Greatly increases diagnostic precision and accuracy through the use of objective, quantitativemeasurement scales and specific case definitions.2. Better characterizes the full spectrum of disabilities of alcohol exposed individuals who do and donot have FAS.3. Documents the presence of alcohol exposure without judging its causal role.4. Provides a quantitative measurement and reporting system that can be used independent of theclinical case definitions.University of Washington, FAS Diagnostic & Prevention Network3
Introduction, Section IDiagnostic Guide for FAS and Related ConditionsWhile this document might at first appear overly complex and perhaps daunting, one will find that thisnew diagnostic approach is logical and easy to use and will greatly facilitate the proper descriptionand classification of patients presenting with all possible combinations of outcomes and exposure.Other syndromesThe methods of diagnosing fetal alcohol syndrome and related conditions arise from the larger fieldsof teratology and dysmorphology (clinical genetics). It is essential to remember that isolated featuresin many birth defect syndromes overlap with FAS. A few examples of conditions often easilyconfused with FAS include Aarskog syndrome, fragile-x syndrome, fetal hydantoin syndrome andNoonan syndrome. Furthermore it is likely that this diagnostic approach to organizing dysmorphicfeatures and issues of cognitive and behavioral problems could be used for patients exposed to otherpotentially teratogenic substances instead of or in addition to alcohol. This diagnostic guide is "FASspecific" but this in no way should imply that the diagnostician need not consider alternate syndromicdiagnoses and medical conditions at all times.4University of Washington, FAS Diagnostic & Prevention Network
Diagnostic Guide for FAS and Related ConditionsDiagnostic Form, Section IIII. FAS Diagnostic Evaluation FormThe FAS Diagnostic Evaluation Form guides the clinical team in the collection, recording, andinterpretation of all key information used to derive an accurate and precise diagnosis. Although themost accurate diagnoses are derived when complete information is available across all domains,complete information is not always available or obtainable. This is especially true with psychometricassessments. Although space has been provided to record a full complement of assessments, we are notimplying that all of these assessments must be conducted to derive a diagnosis. It is the responsibility ofthe clinical team to select the most appropriate psychometric assessment battery.The form also serves as a template for efficient generation of the final medical summary note.Where is the information for the Diagnostic Form obtained from?The information recorded in the Diagnostic Form is obtained from four primary sources:1.The New Patient Information Form completed by the caregivers (Appendix 1).2.Medical/psychological/educational assessments conducted prior to the diagnostic evaluation.3.Assessments administered by the clinical staff at the time of the diagnostic evaluation.4.The caregiver/patient interview conducted at the time of the diagnostic evaluationWhen is the form completed and by whom?The form is completed by the clinical staff before and during the patient's clinic visit. Typically, theclinician completes the following sections: growth, structural and neurologic brain function, facialfeatures, alcohol exposure and co-morbidities. The occupational therapist, psychologist and languagepathologist complete the psychometric measures of brain function and the results of the caregiverinterview are completed by the clinician and psychologist.University of Washington, FAS Diagnostic & Prevention Network5
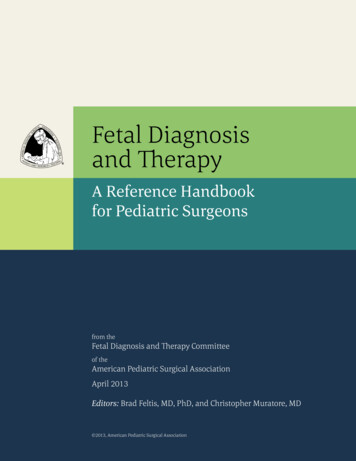
Diagnostic Form, Section IIDiagnostic Guide for FAS and Related ConditionsFAS Diagnostic Evaluation FormMedical #ClinicDate seen in Clinic / /Patient's Name: Age(y)FirstMiddleBirth Date / /LastName person(s) accompanying patientRelationship(s) to patientPatient's GenderMF4-Digit Diagnostic Code GridPatient’s Race/Ethnicity:(See instructions in Diagnostic Guide for FAS and Related Conditions)Form completed by:Diagnosis made 144high risk33some risk22unknown1no riskGrowthFAS FacialBrainDeficiency Features lGROWTHAt BirthBirth weight:(gms)(lbs/oz.),(centile) for gestational ageBirth length(cm)(inches),(centile) for gestational ageGestational age at birth (weeks)Highest Weight and Height Centiles Recordedwgt (kg), (lbs),(centile),age (yr)hgt (cm), (inches),(centile),Lowest Weight and Height Centiles Recordedage (yr),parent adjustment (cm)wgt (kg), (lbs),(centile),age (yr)hgt (cm), (inches),Current Weight and Height(centile),age (yr),wgt (kg), (lbs),(centile),age (yr)hgt (cm), (inches),Birth Parent's Heights(centile),age (yr),parent adjustment (cm)father’s hgt (cm) (inches),mid-parent hgt (cm)mother’s hgt (cm) (inches),ABC-Score for Growth DeficiencySee instructions in the “Diagnostic Guide for FAS”for deriving the ABC-score for growthand translating it into a 4-Digit Diagnostic Codeparent adjustment (cm)Circle the ABC Scores for: 3rd centile C 3rd and 10th centile B 10th centile AHeightCBAWeightCBAThis ABC Score reflects the patient's growth between years and years of age.Page 1 of 76(version 1/1/99)University of Washington, FAS Diagnostic & Prevention Network
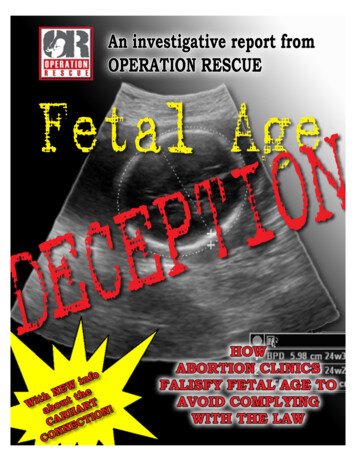
Diagnostic Guide for FAS and Related ConditionsDiagnostic Form, Section IIFACIAL FEATURES (and other physical findings)CURRENT PHENOTYPE: (Age yrs)Direct measuresRight palpebral fissure length (PFL)(cm)(z-score)Left palpebral fissure length (PFL)(cm)(z-score)Inner canthal distance (ICD)(cm)(z-score)Not PresentFlat philtrum*Thin upper lip*Mildly PresentDefinitely Present*1234Clinic Photograph(flat)5(thin)Internal MeasureWas a facial photograph taken? Yes , NoTrue sizeUnits ( )Size in photoUnits ( )Right PFLLength in photo(pixels or mm):True estimate (cm)(z-score)Left PFLLength in photo(pixels or mm):True estimate (cm)(z-score)ICDLength in photo(pixels or mm):True estimate (cm)(z-score)Not PresentFlat philtrum*Thin upper lip*Mildly PresentDefinitely Present1234PAST PHENOTYPE (Age yrs)(flat)Circularity**5(thin)Internal MeasureSource of data ( photograph , text record )Upper LipTrue sizeUnits ( )Size in photoUnits ( )Right PFLLength in photo(pixels or mm):True estimate (cm)(z-score)Left PFLLength in photo(pixels or mm):True estimate (cm)(z-score)ICDLength in photo(pixels or mm):True estimate (cm)(z-score)Not PresentFlat philtrum*Thin upper lip*Definitely Present1234Facial D-score**Mildly Present(flat)Upper LipCircularity**5(thin)Dscore 0.7408 – 5.7337 (Largest PFL/ICD) 1.1677 (philtrum Likert rank) 0.1587 (upper lip Likert rank)*(Use Lip-Philtrum Guide on page 26, Figure 1)** (See Astley & Clarren, 1996)ABC-SCORE for Facial PhenotypeSee instructions in the “Diagnostic Guide for FAS” for deriving the ABC Score and translating it into a 4-Digit Diagnostic Code5-Point Likert Scalefor Philtrum & Lip4 or 531 or 2Z-score for LargestPalpebral Fissure -2 SD -2 SD and -1 SD -1 SDPalpebral FissureCBACircle the ABC Scores for:Smooth PhiltrumCBAThin Upper LipCBAALL ADDITIONAL PHYSICAL ANOMALIES ON THE BODYPage 2 of 7University of Washington, FAS Diagnostic & Prevention Network (version 1/1/99)7
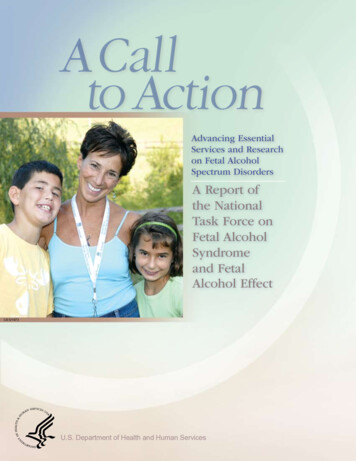
Diagnostic Form, Section IIDiagnostic Guide for FAS and Related ConditionsBRAIN FUNCTIONCircle:Severity01 2301 2301 2300000111112222233333Examiner’s Clinical Judgment of Severity of Outcome0 Unable to Judge, 1 Normal, 2 Mildly Abnormal,3 Severely AbnormalSTRUCTURALOFC (cm) (centile) at (years) of age.Structural anomalies on CT/MRIOther:NEUROLOGICSeizure Disorder: type Age at onset (yrs)Gross motorFine motorQuick Neurological Screening Test scoreOther neurologic signsPSYCHOMETRIC Provide most recent test scores01 23Intellectual: (test/version)Age (yr/mos)FSIQ or equiv. VIQ PIQ PercOrg VerbComp FreeDisInf. Sim. Arith. Voc. Comm. Dig. Pict C. Pict. A. Blo. Obj. Cod. Maz.01 23Age(s) of previous intelligence tests (yrs)Achievement (test/version)SubtestScoreAge (yr/mos)Type of Score (standard, %, age equiv., T, Z, etc)Age(s) of previous Achievement tests (yrs)01 23Adaptation (test/version)Composite Score NameAge (yr/mos)ScoreType of Score (standard, %, age equiv., T, Z, etc)SubtestAge(s) of previous Adaptation tests (yrs)See the “Diagnostic Guide for FAS” for instructions on deriving the 4-Digit Diagnostic Code for Brain Dysfunction8Page 3 of 7University of Washington, FAS Diagnostic & Prevention Network (version 1/1/99)
Diagnostic Guide for FAS and Related ConditionsDiagnostic Form, Section IIBRAIN FUNCTION (Continued)Examiner’s Clinical Judgment of Severity of OutcomeCircle:Severity01 230 Unable to Judge,1 Normal,2 Mildly Abnormal,3 Severely AbnormalPsychiatric Diagnoses: ADHD / ADD ( yes, no, unknown)other (specify)Medication(s)01 23LanguageTest name01 2301 2301 23Medication(s)Response ( , -, none )Neuropsychological (e.g., VMI, CVLT-C, Halstead-Reitan, WRAML, Rey, Bender-G, Luria-Nebraska, etc)Test name01 23Response ( , -, none )ScoreScoreType of Score (standard, %, age equiv., T, Z, etc)Type of Score (standard, %, age equiv., T, Z, etc)Age (yr/months)Age (yr/months)Mental State Reasoning Test 14, 15Age (yr/mos)1st Order ( Belief Justification ) 2nd Order ( Belief Justification )Narrative Test 14, 15Age (yr/mos)Bus StoryFrog StoryDevelopmental (test/version)Age (yr/mos)SubtestScoreType of Score (standard, %, age equiv., T, Z, etc.)See the “Diagnostic Guide for FAS” for instructions on deriving the 4-Digit Diagnostic Code for Brain DysfunctionPage 4 of 7University of Washington, FAS Diagnostic & Prevention Network (version 1/1/99)9
Diagnostic Form, Section IIDiagnostic Guide for FAS and Related ConditionsBRAIN FUNCTION (Continued)Examiner’s Clinical Judgment of Severity of OutcomeCircle:Severity0 Unable to Judge,1 No, NormalCAREGIVER INTERVIEW2 Yes, Mildly Abnormal,3 Yes, Severely AbnormalThese observations are intended to support, not define, clinical impressionsPlanning00000111112222233333Needs considerable help organizing daily tasksCannot organize time,Doesn't understand concept of timeDifficulty in carrying out multi-step tasksOtherBehavioral Regulation/ Sensory Motor 30000111122223333000000111111222222333333Poor management of anger / tantrumsMood Inappropriately [ high or low ] activity levelLying/stealingUnusual [ high or low ] reactivity to [ sound touch light ]OtherAbstract Thinking / JudgmentPoor judgmentCannot be left aloneConcrete, unable to think abstractlyOtherMemory / Learning / Information ProcessingPoor memory, inconsistent retrieval of learned informationSlow to learn new skillsDoes not seem to learn from past experiencesProblems recognizing consequences of actionsProblems with information processing speed and accuracyOtherSpatial Memory0 1 2 30 1 2 3Gets lost easily, has difficulty navigating from point A to point BOtherSocial Skills and Adaptive Behavior0 1 2 30 1 2 30 1 2 3Behaves at a level notably younger than chronological agePoor social/adaptive skillsOtherMotor/Oral Motor Control0 1 2 30 1 2 30 1 2 30 1 2 3Poor/delayed motor skillsPoor balanceOtherBehavioral/Social Competence: (test)SubtestScoreSee the “Diagnostic Guide for FAS” for instructions on deriving the 4-Digit Diagnostic Code for Brain Dysfunction10Age (yr/mos)Type of Score (standard, %, age equiv., T, Z, etc)Page 5 of 7University of Washington, FAS Diagnostic & Prevention Network (version 1/1/99)
Diagnostic Guide for FAS and Related ConditionsDiagnostic Form, Section IIMATERNAL ALCOHOL USEAlcohol consumption of the birth motherBefore pregnancy:Average number of drinks per drinking occasion:Maximum number of drinks per occasion:Average number of drinking days per week:Type of alcohol consumed Wine, Beer, Liquor, Unk., Other (specify)During pregnancy:Average number of drinks per drinking occasion:Maximum number of drinks per occasion:Average number of drinking days per week:Type of alcohol consumed Wine, Beer, Liquor, Unk., Other (specify)Trimester(s) in which alcohol was consumed 1st 2nd 3rd Unk. NoneNoSuspectedYesUnknownWas the birth mother ever diagnosed with alcoholism?Was the birth mother ever reported to have a problem with alcohol?Did the birth mother ever receive treatment for alcohol addiction?Was alcohol use during this pregnancy positively confirmed?If, yes, source of confirmationReported use of alcohol during pregnancy is: Reliable, Somewhat reliable, Of unknown reliabilityOther information about alcohol use during pregnancy:4-DIGIT RANK for Alcohol Exposure4-Digit DiagnosticCode RankGestational AlcoholExposure Category4High RiskDescriptionl Alcohol use during pregnancy CONFIRMEDandl Exposure pattern is consistent with the medical literature placingthe fetus at “high risk” (generally high peak blood alcoholconcentrations delivered at least weekly in early pregnancy).l Alcohol use during pregnancy CONFIRMEDand3Some Riskl Drinking occurred in gestation in frequencies and volumes lessthan in category (4) or exact amounts unknown.l Gestational exposure is simply not known or information is of2Unknown Riskquestionable reliabilityl Alcohol use during pregnancy is CONFIRMED to be completely1No RiskABSENT.Circle the 4-Digit Diagnostic Code Rank in the table above that best reflects the patient's gestational Alcohol Exposure CategoryPage 6 of 7University of Washington, FAS Diagnostic & Prevention Network (version 1/1/99)11
Diagnostic Form, Section IIDiagnostic Guide for FAS and Related ConditionsCO-MORBIDITIESO-MORBIDITIESPRENATALHigh risk4Some risk3Unknown risk2No risk1See the “Diagnostic Guide for FAS” for instructions on deriving the rank for Prenatal Co-morbiditiesPrenatal1. Poor prenatal care:No Suspected Yes Unknown2. Complications/trauma (specify)Genetics1. Parental learning difficulties (e.g. Special Ed., ADD, MR, did not complete high school, etc.)MotherNo Suspected Yes UnknownFatherNo Suspected Yes UnknownIf yes, specify MaternalPaternal2. Other conditions of heritability or malformation that may be significant in this case. (specify)Other Potentially Teratogenic ExposuresPOSTNATALHigh risk4Some risk3Unknown risk2No risk1See the “Diagnostic Guide for FAS” for instructions on deriving the rank for Postnatal Co-morbiditiesPerinatal DifficultiesIssues of Nurture1. Abuse: Physical Sexual2. Number of home placements3. Other (e.g., neglect, adverse home environment, etc)Other Issues That Could Explain Brain Dysfunction (e.g., head injuries, fever, chronic substance abuse, etc.)Page 7 of 712University of Washington, FAS Diagnostic & Prevention Network (version 1/1/99)
Diagnostic Form, Section IIDiagnostic Guide for FAS and Related ConditionsFAS Diagnostic and Prevention NetworkPreliminary Summary and RecommendationsThe final medical summary will be sent to you in approximately two weeks.Patient Name:Clinic:Birth Date: / / Clinic Date: / / Clinic phone:Diagnostic Outcome:Result(s) of assessment(s) performed in Clinic (if applicable):Recommendations for Follow-UpA. Medical IssuesPage 1 of 214University of Washington, FAS Diagnostic & Prevention Network (version 1/1
4. The term fetal alcohol effects (FAE) is broadly used and poorly defined. The term 'suspected fetal alcohol effects' was first introduced into the medical literature in 1978 and was defined as 'less complete partial expressions' of FAS in individuals with prenatal alcohol exposure 2. Based on this definition, an individual whose .