Transcription
GovernanceMarti LӧtterGroup Head of GovernanceUL HospitalsOctober 2019
Vision A health service meeting the National Standards for SaferBetter Healthcare provides care that is safe, effective, personcentred and that promotes better health and well being of thepeople using it. To achieve this the service has good leadership, clearaccountability, effective management and a well-organised,skilled and competent workforce. It uses high quality information and its available resourceseffectively and efficiently to deliver high quality, safe, reliablehealthcare for its service users.
‘Everyone in healthcare has two jobswhen they come to work everyday:to do their work and to improve it’“We are all responsible and together we are creating a safer healthcare systemQuality improvement is everybody's responsibility”Source: Batalden, professor of paediatrics and a senior fellow of the Institute of Healthcare Improvement
Governance for Quality and SafetyWhat is it .? It is described as: the system through which healthcare teams areaccountable for the quality, safety and experience ofservice users in the care they have delivered. For health care staff this means: Specifying the clinical standards you are going todeliver and showing everyone the measurements youhave made to demonstrate that you have done whatyou set out to do.
GovernanceThis can be achieved by creating an environment in which there istransparency of responsibility and accountability for maintainingstandards through measuring against set targets to ensure excellence inpatient care (HSE, 2018).
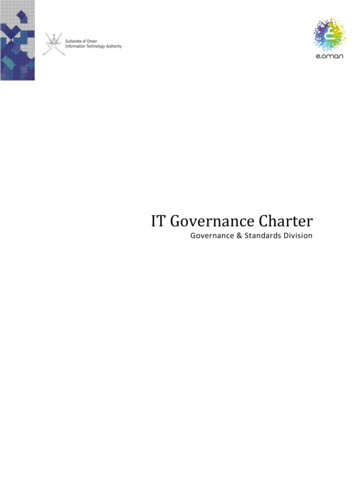
Key Components of Governance Knowledge and skills: Management teams have the knowledge and skills toachieve their role in driving quality care Leadership and Accountability: Management team are clear aboutleadership and accountability Information: Intelligent use of information to measure, monitor andoversee quality and safety of care Culture: A culture of learning focused on quality of care Relationships: The organisation promotes strong relationships that partnerwith patients and staff to facilitate the alignment of the entire organisationaround the quality of care Quality Improvement: There is a quality improvement plan in place foridentified risks aligned with national and organisational priorities
Key Components of Governance
Critical success factors for Clinical Governance Responsibility and accountability Risk management strategy with clear policies Programme of quality improvement activities Clear policies and procedures to identify and correct poorperformance
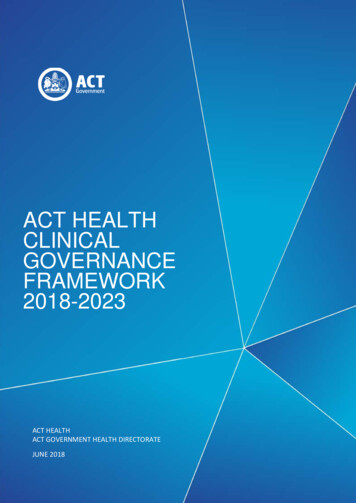
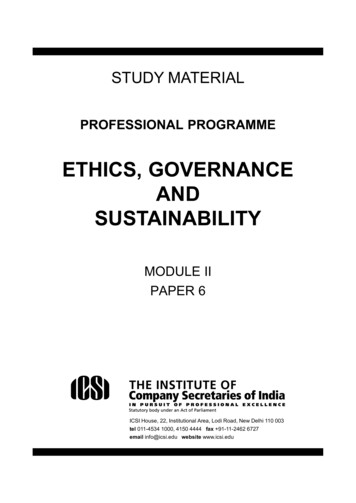
UL Hospitals Group Governance StructureMinister for HealthULHG Organisational GovernanceStructure V1221/05/2018DG HSENational Director Acute HospitalsULHG Board of DirectorsCEOCFOCAOCOODOMDOHRCDONMCIOCCDACD QualityGroup Head ofQualityNDTP Training LeadDirectoratesDiagnosticsClinical DirectorAssociate CDDGMBusiness ManagerPathology ManagerRSMChief PharmacistAHP ManagerRadiologyPerioperativeClinical DirectorAssociate CD x2DGM (H&S)DONBusiness ManagerDivisionsEmergency Med.Acute MedicineElderly MedicineRenalNeurologyInfectious logyGasteroeneterologyDermatologyOncologyClin HaemotologyPalliative CareDivisionsGeneralAnaestheticsPain MedicineVascularOrthopaedicsMaxillofacialCritical CareGeneral SurgeryENTUrologyOpthamologyGroup Head ofGovernanceGroup Head ofStrategyPMO LeadDepartmentsM&CHClinical DirectorAssociate CDDGMDOMBusiness ManagerOperationalServicesDGMFacilities ManagerClinical erationalDON EnnisOperationalDON NenaghScheduledCSBUCareACD x 1DGMData Manager G7Unschedueled0.5 x ADONCareDGMQualityGroup Headof QualityG8Quality &SafetyManagersPALSG7 x 7InformaticsPlanning andPerformanceeHealthDivisionPPBIHIPEICTHRGM X 1G8 x ieteticsMSWMedicineClinical DirectorAssociate CD x 4DGM x 2DONBM x 3Group Head ngContract ServicesColette Cowan CEO ULHGNoreen Spillane COO ULHGFinanceGM x 2G8 x 5
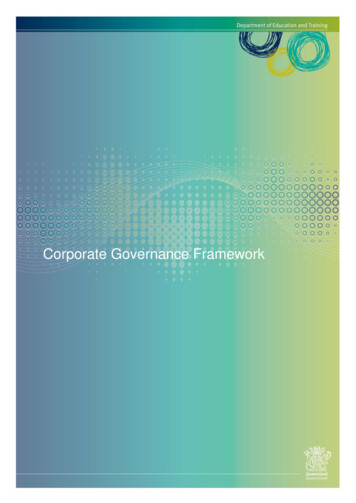
UL Hospitals Group Executive Management TeamCEOMs Colette CowanUL Hospital GroupBoardA/ChiefFinancialOfficerChief sOfficerMr JohnCowheyDr G BurkeProf PaulBurkeMs NoreenSpillaneChiefDirector ofNursing&MidwiferyMs MargaretGleesonInterim HRDirectorDirector ofCommsDirector ofInformatics,Planning andPerformanceLorraine RafterMs ElaineConnollyVacantClinical DirectorsDr Denis O’Keeffe - DiagnosticsDr Catherine Peters– MedicineMr D Waldron– Peri-OperativeDr Siobhan Gallagher– Maternal & Child HealthHead ofStrategy/Head ofGovernanceSuzanne DunneMarti Lӧtter
DirectoratesExecutiveExternalGovernance of UL Hospitals GroupDirectorate Team Members:Clinical DirectorDirectorate ManagerDirectorate Nurse Managers/Service ManagersBusiness ManagerQPS ManagerAccountantHR Liaison
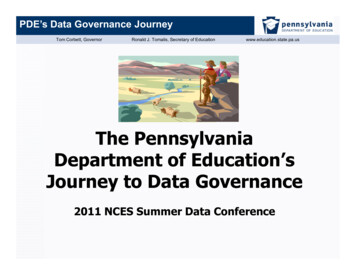
Different Levels of Shared Clinical Accountability accordingto level of responsibility within the Governance StructureCEOCCDCDACDConsultantsService nical SpecialistsSenior Grade StaffCNSNCHDsCateringANPADONBasic Grade StaffMTAPorterGrade 8Grade 7Grade 6CNM3CNM2Grade 5CNM1Grade 4Staff NurseMTA/PorterOperationalSupport ServicesGMConsultantsHSCPsNursingGrade 3Admin staff
Head of Governance RoleGOVERNANCE We work with departments and leaders of, developing and emerging states toenhance their effectiveness.Brief: To provide Governance through Measurement against a baseline.To Achieve: Quality Assurance (clinical and non-clinical quality data) thatcascades from one level to the next to prove continuous quality improvement Organograms of reporting relationshipsFunction of each grade and postList of duties and responsibilities for each gradeService Analysis – KPI selection for Balanced Score CardsRisk RegistersQuality Improvement PlansProject TrackersAudit Forward Plans
Integrated Corporate and Clinical Governance“The main lesson I take from the problems at Midstaffs is that in future, wemust never separate quality and financial data. They are always two sides ofthe same coin.” (Secretary of State for Health, England, 2010) “ .corporateand clinical governance arrangements must include unambiguous lines ofaccountability for assuring, performance managing and improving the qualityand safety of services at a national, regional, local and clinical level” (Ministerfor Health, 2013)
UHLG Governance Model underpinned by1. The HIQA National Standards for Safer Better Health Care (2012)2. HSE Code of Governance of which The Performance and AccountabilityFramework of the HSE (2017) form an integral part.3. The 10 facets of Clinical Governance, Jaggs-Fowler (2011)4. The Quality Risk Management System (QRMS) of the HSE(2008)with Pearson's Law as guiding principle.“That which is measured improves.That which is measured and reported improves exponentially. “- Pearson's Law-
CEO’s Priorities 2019Priority ActionSponsorOwnerCompletion DateStrategic Priority 1 –Clinical Transformation1.Implementation of Sláintecare. Implementation Strategy & ActionPlan.CEOCEO/ Executive TeamQ 1-42.Implement targets for Clinical Transformation to include MedicalTransformation.CEOCCDQ43.Plan & Co-Design place based Integrated Care Models.CEOCEO/ Executive TeamQ 1-4Strategic Priority 2 –Digital Health4.Progress on Microsoft Projects & identify other early innovationsin eHealth.CEOCIOQ35.Establish accessible Data Analytics & Clinical Information forClinical Groups.CEOCIO/CCDQ26.Implement Clinical Information Systems including expansion ofMaxims.CEOCIO/COO/ CCDQ47.Enable Paperless Systems to support Patient Care & operationaleffectiveness.CEOCIO/COO/ CCD/ CDONMQ3Strategic Priority 3 –Research & Innovation8.Progress Plans for Joint Health/University Health ScienceAcademy.CEOHead of Strategy/CAO/CCD/ CDONMQ39.Continue Progress with Future Innovations in Robotics,Technology & Integrated CareCEOCOO/ CDONM/CAO/CCD/ CIOQ 2-410.Establish Formal Approach for Integrated Care & Age RelatedDiseaseCEOCEO/ Executive TeamQ 2-4Strategic Priority 4 –Collaboration & Alliance
Value of New System of Assurance of HSE& Board Advices CEO set priorities according to National Goals CCD/COO/CDONM/CIO/CFO/DHR priorities and QIP’s to alignwith CEO priorities Each Directorate must provide data on the 4 elements thatenables the delivery of an excellent heath service: Quality, Finance , Access, Resources Each Directorate account and are responsible on a monthly basisat Performance Meetings using the Balanced Scorecard Model
Balanced ScorecardThe balanced scorecard is a strategic planning andmanagement system that is used extensively in business andindustry worldwide to align business activities to the visionand strategy of the organization, improve internal and externalcommunications, and monitor organization performanceagainst strategic goals (Norton and Kaplan,1992)
EXTERNAL HIQA (2012)OutcomeDimensions ofQualityProcessCapacity andcapabilityStructure
4 Dimensions of Balanced ScorecardQualityandSafetyPatient and Service User
National Balanced Scorecard for AcuteHospitalsEXAMPLE
Levels of Scorecards NationalUHL BoardCEOExecutiveDirectorateDepartmental
Data Cascades Form One Level to the NextCEO /UHL BOARDForum 1COO/CDONM/CCD/CFO/HR/CIO/DOMCEO /ExecutiveForum 2COO/CDONM/CCD/CFO/HR/CIO/DOMGM/CD/ACDForum 3DirectorateTeam MeetingsForum 4DepartmentalMeetingsForum 5Frontline
Theme 5 Leadership, Governance and ManagementNSSBH (Departmental Level)Standard 5.1 Clear AccountabilityDo you know where to access your departmental organogram with reporting relationships? (organogram)Do you know what every team member’s responsibility is in your department?Standard 5.2 Strong GovernanceDo you know where and how to access departmental policies?Have you read and signed them? What happens if these policies are breached?Standard 5.3 Statement of purposeDo you know where to access your department’s statement of purpose?Standard 5.4. Effective Strategic PlanningDo you know the strategic goals for your department/area? (strategic or development plan)Do you know where to access this document?Standard 5.5 Effective Operation PlanningDo you know the operational plan for your department/area? (operational plan)Are you clear on the day-to day running of the department in times of crisis?Do you know where to access escalation or prioritisation documents for your service?Standard 5.6 Promoting a Culture of Quality and SafetyDo you have monthly staff meetings where you can voice any concerns you might have? (minutes)Do you reflect as a department on complaints/compliments and incidents ? Logs on Q-PulseDo you receive learning notices via e-mail?
Theme 5 Leadership, Governance and ManagementNSSBH (Departmental Level)Standard 5.7 Supporting Staff in delivering Quality and SafetyDo you know how and to whom to report an incident?Do you know what to do when a patient complains about the service?Do you know what to do if you witness an error in patient care?Are training for staff in incident management and QIP provided? (training Records)Standard 5.8 Monitoring arrangements for quality and safetyDo you audit your service regularly and develop and implement quality improvement plans as a result.Do you routinely collect data ? (balanced Scorecards)Do you maintain a risk register for your department? (Risk register)Standard 5.9 Service AgreementsCan you access applicable documents in relation to SLA’sWhat are the monitoring arrangements in terms of quality assurance for 3rd party providers?(SLA’s)Standard 5.10 Compliance with LegislationAre you aware of any legislation governing your service?Do you know where to access this?Standard 5.11 Implementation of Standards, Alerts, Guidance and RecommendationsAre all HIQA recommendations from previous reviews implemented in your service area?Is all relevant standards alerts guidance and recommendations produced by relevant regulatory bodies appliedin your service.
THANK YOU
Plan & Co-Design place based Integrated Care Models. CEO CEO/ Executive Team Q 1-4 Strategic Priority 2 - Digital Health 4. Progress on Microsoft Projects & identify other early innovations in eHealth. CEO CIO Q 3 5. Establish accessible Data Analytics & Clinical Information for Clinical Groups. CEO CIO/CCD Q 2 6.