Transcription
Financing and Funding IndianHealthcare: Navigating the Turbulent Tidewww.pwc.in
Executive summaryThe cost of healthcare or, more appropriately, the cost a nationhas to bear to provide healthcare to its citizens has been one of themost hotly debated issues globally. How one defines this paradigmis important: Is healthcare a right that citizens can demand fromthe state, or is the individual responsible for his/her own health?However, there is a general consensus that unless some form ofuniversal health coverage care is available, the growth of the mostrobust economies can be derailed. The coverage should includeaccess to preventive, promotive and curative care of sufficient qualityto be effective while ensuring people do not suffer financial ruin.One of the tectonic shifts in Indian healthcare has been the launchof ‘Ayushman Bharat’, which addresses both pillars of universalhealthcare coverage—the role of primary care and financial access.Under the National Health Protection Scheme, the governmentplans to cover over 500 million population, making it one of thelargest schemes on the planet. Traditionally, the public and privatesectors have not worked together. International experience showsthat the most efficient public healthcare systems use private capitaland expertise to induce efficiency and innovation. The scheme givesa fresh impetus for both to work together towards achieving thenation’s goal of achieving universal healthcare.A host of factors—ranging from price control to regulatory overreachand safety of the caregivers in hospitals—have threatened toderail the robust growth of the sector. However, we see this as anopportunity to relook at financing and funding, the regulatoryframework and reimbursement mechanisms to build a newhealthcare ecosystem.The ‘New Indian Healthcare Eosystem’ will redefine the healthcaredelivery and products space with low-cost hospitals, specialityclinics, medical devices which cost a fraction of imported devices,mobile technologies which address primary healthcare needs and2 PwCquality healthcare which is affordable. Besides addressing India’sneeds, these innovations have the potential to be replicated in thedeveloping world, where most issues mirror those in our country.Rising patient consumerism, expansion of the continuum ofcare, a shift towards quality-based care, increasing patientparticipation, the use of technology in delivering care, andincreasing insurance penetration are some of the disruptivetrends which the Indian health economy is currentlywitnessing. These trends and turbulent events, along with theimplementation of NHPS, present an opportunity for the relevantstakeholders to redefine and reorganise themselves and adoptnew components of people, process and technology in theirbusiness models, in order to emerge successful in the ‘New IndianHealth Economy’.
Section 1Section 2Section 3Is India movingtowards an equitablehealthcare system?What were the effectsof the turbulent eventsthat hit the Indianhealthcare industrylast year?Can the National HealthProtection Scheme (NHPS)be the inflexion pointfor the industry?Financing and funding Indian healthcareSection 4Section 5Can the Indianhealthcareindustry continueto attract investorsgiven its long-termpotential?Are we now seeingthe birth of a"New Indian Health Economy"?Financing and Funding Indian Healthcare: Navigating the Turbulent Tide 3
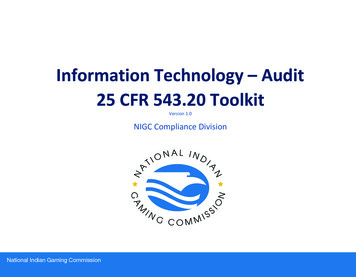
Section 1Is India movingtowards an optimalhealthcare system?India is a microcosm of all the healthcare systems in the world.Healthcare teinsurancePrivate andpublic insurancePrice controlExamplesMostly privateRegulationRegulation andpart-paymentGovernment manages pricesthrough regulationPwC Analysis4 PwCOut of zen tax paymentsCitizen premiumCitizenNeoclassicPublicMostly privateMostly privatePublic/privatePayment anddeliveryPaymentRegulationRegulationand deliveryAs the sole payer, govt. has strong control over aSwitzerlandCubaNew ZealandTaiwanUSA (mixed)Indian examplesDouglas modelClassicCitizen and employer premiumProviderGovernment’s inPublic sectorundertakingsState-run hospitals,armed forcesGovernmenthas limitedcontrolMostdevelopingcountriesSouth KoreaCGHS, PPPsIndividual/groupinsurance (public)Predominantmodel in India
High-quality clinical outcomes at an affordable cost have helpedproject India as a medical hub.The Indian healthcare system is moving towards quality healthcare at an affordable cost.37 Joint CommissionInternational (JCI)1 accreditedhospitals and 513 NationalAccreditation Board for Hospitals & HealthcareProviders (NABH)2 accredited hospitalCost of treatment is less than1/10th in comparisonto the USA3Clinical outcomes in leadinghospitals are comparableto those of internationallyrecognised facilitiesA strong brand of alternative medicineand rejuvenation therapies, along withan emphasis on wellnessandprevention, has drawn patients from across theglobe to the country.Source: 1 - JCI website, 2 - NABH website, 3 – IBEF website, PwC analysisFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 5
A strong quality focus and clinical outcomes at a low cost, coupled with credibility in alternative medicine, haveresulted in growing medical tourism in the countrAfghanistanIraqPakistanOmanAround OverBangladeshNigeriahalf a millionmedical visaswere issued inKenya2016.MaldivesThe numberhas increasedat a CAGR of 52% from2014 to 2016.source : Ministry of Tourism, Government of IndiaA strong quality focus and clinical outcomes at a low cost, coupled with credibility in alternative medicine, have resulted in growing medicaltourism in the country.Focus specialties for MVT in IndiaCardiac sciencesOrthopaedicsSource: PwC analysis MVT Medical Value Travel6 PwCOrgan transplantsNeurosciencesOncologyBariatrics
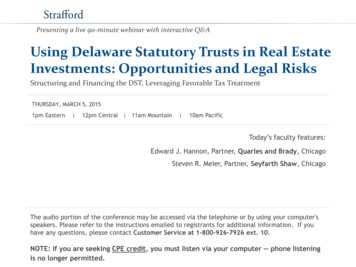
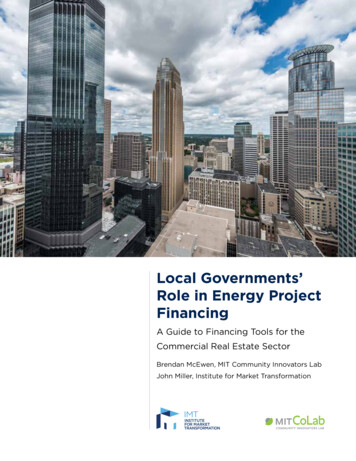
India has a commitment to achieve Universal Health Coverage (UHC) [as part ofSustainable Development Goals]. However, its total healthcare expenditure is lessthan 5% of its GDP, which has resulted in sub optimal outcomes.Universal Health Coverage TracerIndex (2017)1009080Bangladesh70UKUzbekistan Jamaica Argentina HungaryKyrgyz RepublicChileSri LankaBhutanZimbabweKenyaRwandaRussian ral African Republic Niger3010Pakistan100MauritaniaIndiaNigeriaUnited StatesNorwaySwitzerlandSingaporeTracer Indexgap for Indiaat current levelof healthexpenditurespend100010000Health expenditure per capita, PPP (constant 2011 international USD) (logarithmic scale)Source: World Bank estimates, SDG Index and Dashboards Report 2017OOPE : Out of Pocket ExpenditureUHC tracer definition : UHC Tracer Index: Summary measure of coverage of essential health services, computed for eachcountry by averaging service-coverage values across 16 tracer indicators on (i) reproductive, maternal, newborn andchild health; (ii) infectious diseases; (iii) non-communicable diseases; and (iv) service capacity and access, and healthsecurity. A higher score reflects a higher access to these services.Financing and Funding Indian Healthcare: Navigating the Turbulent Tide 7
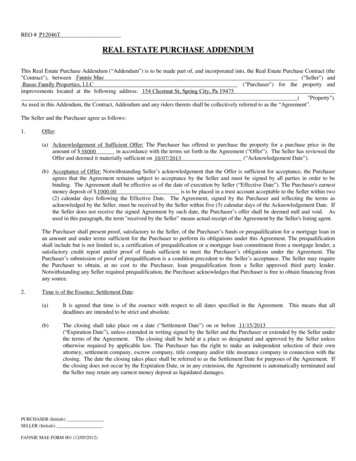
High performing countries have used different methods for healthcare financing toachieve UHCHighgovernment prepaid spendHigh government spendHigh government out ofpocket expenditure (OOPE)14% 13% 19% 7% 13% 22% 14% 18% 5% 11% 14% 13% 24% 24% 14% 20% 10%31% 50% 56% 25% 27% 28% 18% 28%11%30% 66%39%85% 85% 78% 80% 77% 77% 84% 78% 88% 82% 72% 83% 76% 71% 85% 70% 83%56% 46% 42% 60% 62% 68% 68% 67%50%Government pending as percentage of total healthcare spendOOPEPrepaid spending as percentage of total healthcare spendDevelopment assistanceSource: Future and potential spending on health 2015-40: Development assistance for health, and government, prepaid privateand out of pocket health spending in 184 countries.Lancet 2017; 389:2005-30.8 PwCIndiaAverage*United poreCyprusArgentinaUnited KingdomAustraliaSwedenSpainSlovak RepublicNorwayCanadaNew andDenmarkCzech Republic58% 31%Average of countries shown
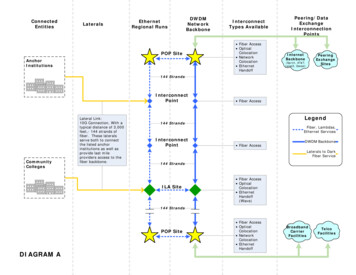
Relatively highRelatively lowLife expectancy at birth (years, 2015)The Nature of increased healthcare spend is important for better cost- efficienthealth outcomes.GreeceChileKorea, Rep. SpainJapanAustraliaSwedenSwitzerlandUnited StatesItalyCost – Efficient spendCost – Inefficient spendIndiaCountries performing low on healthcare IndicatorsRelatively lowRelatively highHealth expenditure per capita, PPP (constant 2011 international USD)Source: World Bank estimatesFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 9
In summary India is a microcosm of all the healthcare systems inthe world given its multiple attributes, be it those ofprovider, payor or the role of the private sector and thegovernment. The country is able to provide best quality outcomes ataffordable price points, thus leading to a more than 50%annual growth in the issuance of medical visas for the lasttwo years. However, significant challenges remain, especially relatedto healthcare expenditure, which is less than 5% of theGDP as compared to the world average of 10%. This has impacted India’s stride towards UHC, with OOPEbeing above 60%. Countries which have performed relatively well on UHCgenerally have high government spending on healthcare.10 PwC
Section 2What were theeffects of theturbulent eventsthat hit the Indianhealthcare industrylast year?DemStakeholderso n etis a tio nD i a g n o s tic sc o m p a niesGOtherregulHealthni dyoratPrice capuesissmptsforfi xing proaldicces ereM vi urd e f actum ansaPh cAtterom m acp a e u ticalsn iescedureratesFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 11
Impact of these eventsEventWhat happened?What was the impact?Price cap (stentand implant)*The NationalPharmaceutical PricingAuthority (NPPA) fixed aprice ceiling for stents inFebruary 2017 (amendmentin Feb 2018) and for kneeimplants in August 2017 Significant reduction in stent and implant prices along with reduction in trade margins (capped at 8%)for the entire distribution value chain (including hospital)Circulation of highdenomination currency (500and 1,000) was stopped inNovember 2016. Given the high OOPE expenditure, there were liquidity issues for cash paying patients. This made itdifficult for patients to pay for acute procedures/surgeries and also led to postponement of electivesurgeries.Attemptsfor fixingprocedure ratesSome states (West Bengal**and Karnataka**) haveattempted to regulate andfix procedure rates. Cap on procedure rates could make it difficult for hospitals to provide quality services.OtherregulatoryissuesHospitals were penalisedand licences werecancelled on account of 1-2unfortunate incidents. A few hospitals were forced to curtail operations (hospital licence cancelled, removal from governmentempanelment, suspension of operations for a few departments) for a brief period. This resulted in revenueloss and negatively impacted the hospital’s image.Demonetisation Companies withdrew premium stents from the Indian market. Companies have less inclination to launch new products given the uncertainty in the regulatory scenario. Reverse medical tourism with patients from India travelling to neighbouring countries for availing medicalservices. Hospitals and diagnostic centres saw reduction in revenue growth for a few months. Lower profitability due to this capping can impact new hospital investments. Possibility of other states also bringing in similar bills with an aim to cater to populist sentiments. Patients could not avail/had to postpone treatment or look for alternative options. Anxiety and job security concern for employees Question of propriety – should the patients, employees and the organisation suffer due to an individual’smistake or error?Source: *NPPA, **West Bengal Clinical Establishment Regulatory Commission, the West Bengal Clinical Establishments Registration, Regulation and Transparency Bill, 2017, and theKarnataka Private Medical Establishments (Amendment) Bill, 2017, Newspaper articlesUHC – Universal Health Coverage12 PwC
What needs to be done?While one of the events (demonetisation) was a one-off event, theynevertheless signal a need for change: There is a strong need for increasing transparency, improvinghospital and patient connect, and dispelling the negativeperception of the industry. With the aim of balancing the need for returns for investorsand affordability for patients, there is a need for hospitals tolook at their cost structure and work on operational efficiencyprogrammes. Technology advancements elements such as AI, wearablesand other mobile technologies, along with IoT, can play a bigrole in delivering quality and affordable care. The government also needs to use this opportunity to create arobust regulatory framework keeping in mind the interest of allstakeholders. There is a need for all the stakeholders to join hands and createstandard treatment protocols and SOPs which will helpimprove transparency and trust. While all the above measures will help, the major issue remainsthe high OOPE. Effective implementation of NHPS and UHCcould solve this problem.Financing and Funding Indian Healthcare: Navigating the Turbulent Tide 13
Section 3Can NHPS be theinflexion point forthe industry?World’s largest non-contributory government-sponsored health insurance schemeFeatures of scheme0.5 billionbeneficiariesBeneficiaryidentification as perSocio EconomicCensus 2011Proposed Aadhaarlinkage5,00,000 INRfamily floater capPremium to be borne60:40 by Centreand state14 PwCAdditional source offunding for government:1% cessParadigm shiftsShift towards outputbased strategicpurchasing of servicesfrom private sectorNew institutionalstructures proposed –National HealthAgency and StateHealth AgencyBoth public andprivate hospitals tobe empanelledFocused on themost vulnerablepopulationMerger of differentgovernmentinsurance schemesGovernmentshifts from beinga provider to apayer also
How will the NHPS evolve?Short-term steps Set up governancemechanism Increase hospitalempanelment Define the benefits underthe schemeLong term steps Benefits under thescheme to include OPDand Primary careMedium-term steps Price discovery andfinancing Right targeting ofbeneficiaries Expand schemecoverage Build in systemefficiencies Merge differentschemesStakeholder ImplicationsHospitals Push for package rates Focus on quality Focus on accreditationPharmaceuticalsand diagnosticcompanies Focus on low-cost drugs and qualityInsurancecompanies Build capacities to handle large claims and identifyfrauds, abuse and misuse Focus on centralised procurement Focus on supply-side shortages Empanel hospitals in tier 2 and 3 areas Negotiate package rates Improve system automation Build actuarial capacities, clinical audit capacity andhospital scrutinyDigital and ITservice providers Develop IT architecture to link patient data, hospitaldata and insurance company data with SocioEconomic Classification (SEC) and Aadhaar dataCentral and stategovernment andsector regulators Identify sources of financing Build in system automation for monitoring andgrievance redressal Ensure fair competitionFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 15
Current ecosystemHospitalsHospitalempanelment: 35,000 hospitalsunder ROHINI,majority intier 1 and 2 citiesPackage rate: 150 proceduresunder GIPSApackageHospital fraud: 15% of allclaims are fraudulentclaims 7State governmentPatientsDifferent schemeslike RSBY and otherinsurance schemesHospitalpayment: 25% of claims(in terms ofvalue)are settled afterone monthPeople insured: 33.5 crore persons under government-sponsored health insurance,including RSBY 5PatientsOOPE: 60% of THE is OOPE. Limited coverage of pre-andpost-hospitalisation expenses.6Insurance companies/TPAsROHINI – Registry of Hospitals in Network on Insurance, GIPSA – General Insurers’ Public Sector Association (India), RSBY - RashtriyaSwasthya Bima Yojana, TPA – Third party administrator, THE – Total health expenditureSource: 5. IRDA Annual Report 2016-17; 6. National Health Accounts 2013-14; 7. Industry reports16 PwC
Future ecosystemIncreased focus on quality (NABH) andtreatment protocols/standardsIncrease innumber ofhospitalsempanelledespecially inlower ordercities andrural areasIncrease inpatientnumber andclaim casesIncrease innumber ofprocedures underpackage ratesTechnology toact as aunifying forceHospitalsImprove systemefficiencies andcapacitiesInsurance companies toempanel public hospitals alsoDecrease innumber offraudulentcases forviabilityState governmentMergedifferentSchemesPush for instantclaim settlementdriven by Aadhaarand use oftechnologyImprove systemefficiencies andcapacities50 crore people, instant claim settlement, empanel public hospitals,package rates, quality, hospitals empanelledBenefit package to include multiple inpatient department (IPD) careprocedures along with pre- and post-hospitalisation chargesInsurance companies/TPAsPatientsFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 17
Section 4Can the Indianhealthcare industrycontinue to attractinvestors givenits long-termpotential?Most of the leading hospital chains have shown steady revenue growthdespite the recent headwinds.Revenue growth of the leading hospital chains in the country9%1%FortisHealthcare*12% 11%ApolloHospitals*18% 17%NarayanaHealth9M FY17 over 9M FY 1618 PwC21% 18%23%HCG9M FY18 over 9M FY 179%Max*17%ShalbyHospitals*Only the hospital businessrevenue is accounted for inthese cases.Source: Q3 Earning updates forFY17 and FY18 from companywebsites – Apollo, Fortis, NarayanaHealth, HCG, Max and ShalbyHospitals
Healthcare Players continue to see listing as an attractive optionfor raising fundsYearCompanyHealthcare IPOsShalby HospitalsAmount raised (crore INR)At an approx. valuation (crore INR)504.82,678Aster DM a Health6135,109HCG6501,854Dr. Lal Pathlabs6704,500Like FY 16 and FY 17,FY 18 also witnessedcontinued investorinterest in healthcareIPOs, with Shalby andAster DM getting listedSource: VCCircle and Livemint websiteFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 19
PE deals and FDI inflow in the last 12 monthsAreasKey featuresMajor private equitydeals since the lastreport (more than 10million USD)The interest of the private equity fraternity continued in the year 2017 with multiple companies in the healthcare sector raising funds.This year also saw private equity interest in the home healthcare spaceSince January 2010,more than 110private equity (PE)and venture capital(VC) investors haveinvested in Healthcaredelivery space.Source: Venture IntelligencePwC analysis20 iant Life Care200HospitalsKKRJuly ’17Condis Healthcare200HospitalsIndia Value FundMar ’17Manipal Health Enterprises171HospitalsTemasekMar ’17Max Healthcare Institute75HospitalsIFCMay ’17Paras Healthcare43HospitalsCreador CapitalJuly ’17Healthcare at Home40Home healthcare servicesQuadria IndiaApr ’17Portea Medical26Home healthcare servicesIFC, Accel India, Sabre Capital, QualcommVentures, CDC-MEMGNov ’17Asian Institute of MedicalSciences21HospitalsCDC GroupDec ’17Nightingales Home HealthServices21Home healthcare servicesEight Roads Ventures, Mahindra PartnersApr ’17iGenetic Diagnostics20DiagnosticsCDC-MEMGMar ’17Regency Hospital14HospitalsIFC, Healthquad, Kois InvestFeb ’17ASG Eye Hospitals11.7Eye CareIDFC AlternativesSep ‘17
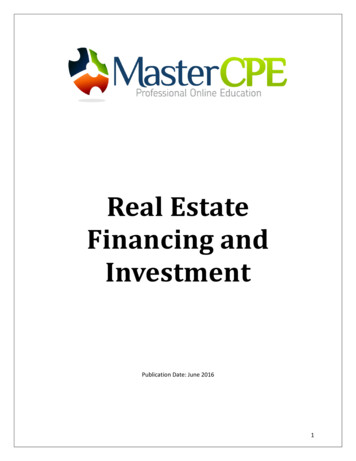
Healthcare has seen a significant increase in FDI inflow over the last 4 years.Healthcare FDI inflows (million USD)Healthcare FDI overthe years.24031 82 576 856636477 47FY11FY12FY13FY14FY15FY16FY 17Source: FDI Fact SheetsIn summary Most of the leading hospital chains have shown steady revenue growthdespite the recent headwinds. FY18 continued to witness interest from the primary market in healthcarecompanies, with the listing of Shalby Hospital and Aster DM Healthcare. The interest of the PE fraternity continued in the year 2017, with investmenttaking place in multiple healthcare companies. FDI flow continued unabated with a flow of 747 million USD in FY17, thehighest amount in the last 7 years.Financing and Funding Indian Healthcare: Navigating the Turbulent Tide 21
Section 5“Are we now seeingthe birth of a “NewIndian HealthEconomy”?”22 PwC
To grow in this “New Indian Health Economy”, stakeholders need to focus oncreating value in the ecosystemNew Indian HealthEconomyAn ecosystem of collaboratorswith interrelated value drivers Renewed focus ongenerics Healthcare trackersand wearables Rise in consumerism Enhanced customer/patient experiencePharmaceuticalsand life sciences Shift from sickness towellness Tailored health plan Operational efficiency Digital health Better quality at lower cost Integrationwith telecom Physician engagementmodelContinuumof careCaretransparencyConsumer Artificial intelligence RoboticsHealthcare providersTechnologyas leverLow cost Increase insurancepenetration Focus on quality outcomes Decrease fraudsInsurance companiesQualityoutcomesTechnology players NHPSimplementation Effective financemechanismHospital providerConsumerGovernmentFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 23
To grow in this ‘New Health Economy’, stakeholders need to alignthemselves with the accelerating trends.New Indian Health EconomyShift from volume to valueCare deliveryTechnological advancesand digitalisationRise of consumerismGovernmentFrom sick Focus on moving from providerto payor Effective implementation of NHPS Renewed focus on genericsDiagnostics andtherapeutics Facilitate ‘Make in India’WellnessTo wellProviders Providers need to recalibrate theiroperating model Leverage the following:DecentralisationSurge in interest inwellness Technology Value-based care Operational efficiency Patient experiencePlatform and support24 PwCFinancing, paymentand regulation
AboutNATHEALTHNATHEALTH has been created with theVision to “Be the credible and unified voice inimproving access and quality of healthcare”.Leading Healthcare Service Providers, MedicalTechnology Providers (Devices, Equipments& IT), Diagnostic Service Providers, HealthInsurance companies, Health EducationInstitutions, Medical Journalism companies,Biotech/Lifesciences related companies,Healthcare Publishers, Healthcare Consultants,Home Healthcare companies, PE & VC companiesand other stakeholders have come together tobuild NATHEALTH as a common platform tocreate the next level of momentum in IndianHealthcare. NATHEALTH is an inclusiveInstitution that has representation of small &medium hospitals and nursing homes as well asHealthcare Start-up companies. NATHEALTH iscommitted to work on its Mission to encourageinnovation, help bridge the skill and capacitygap, help shape policy & regulations and enablethe environment to fund long term growth.NATHEALTH aims to help build a better andhealthier future for both rural and urban India.About PwC’sHealthcarepracticePwC India’s Healthcare team offersadvisory services in the healthcare sectorcovering multiple domains such as strategy,business planning, market scan, commercial duediligence, feasibility study, operationsimprovement, cost reduction, health IT, digitaland technology, internal audit and PPPs.Healthcare Advisory has a dedicated teamwith diverse operational experience in settingup and managing hospitals, and in healthcareconsulting. This enables the team to delivergranular strategy and market and operationalinsights of the highest quality. The team workswith leading healthcare providers, medicaltechnology companies, central and stategovernments, diagnostic players, insurancecompanies and private equity players on projectsboth in India and overseas.ContactContactMr. Anjan BoseSecretary General, Healthcare Federationof India (NATHEALTH)Mb: 91-9999016000anjan.bose@nathealth.co.inDr. Rana MehtaPartner and Leader, HealthcarePricewaterhouseCoopers Private LimitedD: 91 124 6266710 M: 91 9910511577rana.mehta@pwc.comFinancing and Funding Indian Healthcare: Navigating the Turbulent Tide 25
About PwCAt PwC, our purpose is to build trust in society and solve important problems. We’re a network of firms in 157 countries with more than2,23,000 people who are committed to delivering quality in assurance, advisory and tax services. Find out more and tell us what matters toyou by visiting us at www.pwc.comIn India, PwC has offices in these cities: Ahmedabad, Bengaluru, Chennai, Delhi NCR, Hyderabad, Kolkata, Mumbai and Pune. For moreinformation about PwC India’s service offerings, visit www.pwc.com/inPwC refers to the PwC International network and/or one or more of its member firms, each of which is a separate, independent and distinctlegal entity in separate lines of service. Please see www.pwc.com/structure for further details. 2018 PwC. All rights reserved.AcknowledgementsHealthcare TeamDr. Preet MataniAshish RampuriaDr. Ashwani AggarwalVarun KarwaDr. Kuntal MukherjeePublishing and Online TeamDion D’SouzaCorporate Communications TeamKirtika Saxena26 PwC
Financing and Funding Indian Healthcare: Navigating the Turbulent Tide 27
pwc.inData Classification: DC0This document does not constitute professional advice. The information in this document has been obtained or derived from sources believed byPricewaterhouseCoopers Private Limited (PwCPL) to be reliable but PwCPL does not represent that this information is accurate or complete. Anyopinions or estimates contained in this document represent the judgment of PwCPL at this time and are subject to change without notice. Readersof this publication are advised to seek their own professional advice before taking any course of action or decision, for which they are entirelyresponsible, based on the contents of this publication. PwCPL neither accepts or assumes any responsibility or liability to any reader of this publicationin respect of the information contained within it or for any decisions readers may take or decide not to or fail to take. 2018 PricewaterhouseCoopers Private Limited. All rights reserved. In this document, “PwC” refers to PricewaterhouseCoopers PrivateLimited (a limited liability company in India having Corporate Identity Number or CIN : U74140WB1983PTC036093), which is a member firm ofPricewaterhouseCoopers International Limited (PwCIL), each member firm of which is a separate legal entity.KS/March2018-12229
Financing and Funding Indian Healthcare: Navigating the Turbulent Tide 7 India has a commitment to achieve Universal Health Coverage (UHC) [as part of Sustainable Development Goals]. However, its total healthcare expenditure is less than 5% of its GDP, which has resulted in sub optimal outcomes. Angola Arge nti na Bangladesh Bhut an