Transcription
MalpracticeSurvival Kitfor Oral and Maxillofacial SurgeonsOMS
Contact UsConnect with MedPro and Get Started Today.1-800-4-MEDPRO x d@MedProDentalWEBSITETWITTERoms@medpro.comRequest A QuoteEMAILSCAN
MalpracticeSurvival Kitfor Oral and Maxillofacial Surgeons
01Malpractice 10108Understanding Malpractice Policies 1 0Understanding Malpractice Claims & Defense 22Understanding Malpractice Insurance04 05Who is MedPro?3942Malpractice Longevity Chart 44ASDA Discount 46What is MedPro’s OMS Preferred ProgramMost Proactive & Winning Claims Defense02Dental SpecialtyAdvisory BoardMedPro’s Dental Specialty Advisory Board49
02 03Risk Management 1012710 Ways to Reduce Your Liability Risk 29Clinical Risk Management06Glossary & NotesGlossaryTrue or False Quiz5557Choosing the Right MalpracticeInsurance CompanyHow to Choose a Company3507Get StartedContact UsRequest a Quote616203
Welcome to the Big Leagues.Congratulations, you’ve made it. Now it’s timeto start your career. It’s also time to considermalpractice insurance.That’s why Medical Protective developedthis Malpractice Survival Kit for Oraland Maxillofacial Surgeons. It gives youeverything you need to make an informeddecision about malpractice insurance,including a guide to choosing a carrier,instructions on how to obtain insurance,an explanation of policy types and helpfulrisk management tips.We’ve also included information aboutMedPro and what makes us the industryleader in malpractice insurance.If you have any questions about theenclosed information, please contact yourMedPro representative. Our goal is to helpyou make an informed decision, and tomake the selection process easy.Let’s get started.04
Malpractice 101HANDBOOK0101
Malpractice 101
From childhood, Steve had known thathe wanted to be an oral and maxillofacial surgeon.He worked hard to achieve this dream, graduated with honors fromdental school and was accepted into his first choice of residencyprograms. Everyone agreed he was one of the best and brighteststudents. After completing residency, Steve had a handful of joboffers and his whole life ahead of him. Steve joined a prestigiouspractice and was successful in a short period of time. He married,bought a house, and was thoroughly enjoying life.Three years later, Steve received noticethat a lawsuit was being filed againsthim for services he had provided duringhis first year of practice. His psyche andconfidence were shaken, and he wasunsure of how to proceed.Unfortunately, Steve had never takenthe time to read his malpracticeinsurance policy in any detail. He reallyhadn’t understood many of the terms,such as “claims-made coverage,” “policylimits,” and “consent to settle.” Asmany do, Steve had allowed someoneelse – his practice manager – to selecthis malpractice insurance. Now he hadno way of knowing whether or notthis decision left him with sufficientcoverage or quality claims defensenecessary to protect him duringthe case.This scenario is not uncommon. Arecent Medical Protective studyindicates that 64% of first-timemalpractice insurance buyers allowothers to either recommend or decidefrom which malpractice insurancecompany they should purchase theirinsurance.1 New-to-practice oral andmaxillofacial surgeons may be poorly1Medical Protective internal dental malpractice data, 2013informed about insurance issues. As aresult, they may feel more comfortableleaving such an important decision inthe hands of others. However, somelater regret the malpractice companyor insurance policy that was chosen —usually at the time a claim is made orwhen the insurance company exitsthe market.This handbook outlines the critical factorsto consider when choosing malpracticeinsurance. It also introduces MedicalProtective’s OMS Preferred programand our expertise in healthcare liabilitycoverage (malpractice insurance).64% of first-time malpractice insurance buyers allowothers to either recommend or decide from whichmalpractice insurance company they should purchasetheir insurance.%07
Understanding Malpractice InsuranceIn basic terms, malpractice refers to a deviationfrom the standard of care that results in patientinjury or death due to negligent treatmentor failure to diagnose and/or treat. If it canbe proved that an oral and maxillofacialsurgeon acted negligently to cause a patientinjury, the patient may be able to recoverdamages through the civil litigation process tocompensate for his or her harm.A dereliction of professional duty orfailure to exercise an ordinary degreeof professional skill or learning by onerendering professional services whichresults in injury, loss, or damage.malpracticeas defined by Merriam-Webster08
QuizIf an OMS practices for 30 years,in approximately how manyclaims could he or she expect to beinvolved?2a) 10b) 1c) 4d) 6Approximately how many OMS arenamed in lawsuits every year?a) 2,500b) 1,000c) 500d) 920WHAT IS MALPRACTICE INSURANCE?A malpractice (healthcare liability) insurancepolicy typically provides for both defensecosts when a malpractice case is broughtforward and indemnification for anydamages deemed payable to the plaintiff.WHY DO I NEED MALPRACTICEINSURANCE?Many oral and maxillofacial surgeons whohave not been involved in a lawsuit think,“This won’t happen to me.” Unfortunately,each year, about 920 of your futurecolleagues are named as defendants inmalpractice lawsuits. Although the likelihoodof being involved in a lawsuit can increase ordecrease based on practice location, type ofThe average dental-relatedmalpractice payout is about 68,000, not includingdefense costs or lostincome.practice, and procedures you perform, thisaverages to approximately four claims in atypical OMS’ career.The National Practitioner Data Bank (NPDB)indicates that the average dental-relatedmalpractice payout is about 68,000. Thisnumber is limited to the actual indemnitypayment to a plaintiff; it does not includedefense costs, which can be greater thanthat same amount when defending a claim ina malpractice trial.A lawsuit is not necessarily the tool thatmeasures “good” or “bad”, but the end resultof a malpractice claim can be traumatic,time-consuming, and expensive — regardlessof the final verdict.Estimated based on the number of reported claims to the NPDB.09ANSWERS: 1. C 2. D2Did you know?
Understanding Policy TypesWhen it comes to malpractice Insurance, you have twodistinct coverage options: occurrence or claims-made.The major difference between the two types of coverage is whether coverage istriggered based on when an incident occurs or when an actual claim is filed.Occurrence CoverageOccurrence coverage is triggered the moment treatment occurs, regardless of when an eventualclaim is filed.EXAMPLEIf a claim is filed in 2015 based on treatment rendered in 2013, the 2013 occurrence policy responds.Benefits of Occurrence Coverage Coverage is provided for treatment renderedwhile the policy is in effect regardless ofwhen the policy period is over. A separate set of policy limits is availableevery year you have occurrence coverage.This means policy limits stay in place yearafter year, even after the end of the policyperiod. There is no need to purchase tail coverage(see next page). When factoring the cost of tail coverage,occurrence policies are often less expensivethan claims-made policies.Claim is Madein 20152015 Claims-made PolicyResponds2013201420132012Incident Occursin 20132013 Occurrence PolicyResponds102015
Claims-made CoverageClaims-made coverage is triggered when the claim is filed. This means that a policy must be in effectwhen the claim is filed.EXAMPLEIf a claim is filed in 2015 based on treatment rendered in 2013, the 2015 claims-made policy willrespond as long as the treatment occurred after the policy’s retroactive date.Benefits of Claims-made Coverage Initially, claims-made policies are less expensive than occurrence policies.TAIL COVERAGE?Because claims-made coverage is triggered when a claim is filed, these policies do not cover claimsfiled after the termination or cancellation of the policy. To extend coverage after termination orcancellation of a claims-made policy, you will need to secure an extended reporting endorsement(called tail coverage) or your new insurance company must cover your prior acts.Many who purchase claims-made coverage assume that they will someday qualify for free tailcoverage. However, each year more than 75% of tail coverage that is issued at Medical Protective ispurchased.3Tail coverage is generally very expensive. In fact, depending on thestate, tail coverage can cost 140–220% of your current, undiscountedannual claims-made premium. Payment for tail coverage is typicallydue in full and must be paid within 30–60 days of policy cancellation.Some companies will offer tail coverage at no charge in the eventof death, permanent disability, or, in some cases, at retirement. Lookfor the questions to ask regarding claims-made policies and tailcoverage in the “How to Choose the Right Malpractice InsuranceCompany” section on page 35.3Medical Protective internal data, 2014.11
Common Circumstances That Require thePurchase of a Tail:12MOONLIGHTINGRELOCATIONLEAVE OF ABSENCEIf you choose to moonlightduring residency with aclaims-made policy, youmay need to purchase tailcoverage when you are readyto leave. This covers theexposure that remains afteryou move on.If you move toa state whereyour insurancecompany does notoffer coverage orwhere the costof malpracticeinsurance issignificantly lowerthan the originalstate, you mayneed to purchasetail coveragefrom your currentinsurance company.You may want to terminatecoverage while taking a leaveof absence from practice.If you are insured under aclaims-made policy, it mayrequire the purchase of tailcoverage. Examples of a leaveof absence include maternity/paternity leave, poor health, asabbatical, and medical missiontrips.
NON-RENEWALMOBILITYFACULTYIf your insurerdoes not renewyour policy, andif that policy wasa claims-madepolicy, you mayneed to purchasea tail policy tomaintain coveragefor all proceduresperformed duringthe claims-madecoverage.An increasing number ofnew oral and maxillofacialsurgeons are joining dentalfranchises. Statistics haveshown that the policiesprovided are often claimsmade. The average lengthof employment withthese organizations is1.5 to 2 years. You maybe required to buy tailcoverage when you leavethe franchise, unless yournew employer commitsto pay for tail coverage inyour employment contractor another insurancecompany covers your prioracts.More dentalspecialists aredeciding to work in afaculty setting priorto retirement. Whatif you leave privatepractice to work fora university? In orderto ensure coveragefor proceduresperformed duringyour time spent inprivate practice,you must purchasetail coverage if youwere insured under aclaims-made policy.Key TakeawayTo eliminate the above-listedcomplexities involving tail coverage,you may want to purchase anoccurrence policy.13
Policy LimitsPolicy limits are written as two numbers, such as 1 million/ 3 million. The first number, 1 million, reflects what the insurance company will pay per claim/occurrence. Thesecond number, 3 million, is the aggregate limit for the policy year.There is no universal agreement on how much malpractice insurance coverage issufficient, so most insurance companies currently provide a variety of policy limitsranging from 100,000 to 5 million per claim (“per claim limit”). Depending onyour state, you may have a required minimum limit of liability. Check with yourpersonal attorney prior to deciding on policy limits.HOW DOES THE TYPE OF COVERAGEAFFECT THE POLICY LIMITS I PURCHASE EVERY YEAR?Policy limits dictate the maximum amount of money your insurance company will payon your behalf. How a policy’s limits of liability respond to claims is one of the majordistinctions between occurrence and claims-made coverage. The difference betweenoccurrence and claims-made policy limits becomes even more relevant once the claimsmade coverage is terminated and tail coverage is purchased or earned.OCCURRENCEOccurrence coverage provides a separateset of limits for each year you buy thepolicy, with respect to alleged errorsoccurring during the policy period,regardless of when a claim is made againstyou. Occurrence coverage doesn’t endwhen the policy terminates; instead, thelimits under the policy remain available topay future claims based upon incidents thatoccurred during that policy period.CLAIMS-MADEContrast this with claims-made coverage, which onlyprovides limits for claims made during the currentpolicy year, so only the current set of limits isavailable to pay claims arising from all your previousyears of practice. For a claims-made policy thatoffers a standard 1 million/ 3 million policy limit,only 1 million is available to pay any single claim,and only 3 million total to pay all claims arisingduring the span of the policy period.14YR 22 1/ 3YR 16 1/ 3YR 23 1/ 3YR 17 1/ 3YR 11 1/ 3YR 18 1/ 3YR 12 1/ 3YR 7 1/ 3YR 24 1/ 3YR 4 1/ 3YR 19 1/ 3YR 13 1/ 3YR 8 1/ 3YR 20 1/ 3YR 14 1/ 3YR 9 1/ 3YR 5 1/ 3YR 2 1/ 3YR 25 1/ 3YR 21 1/ 3YR 15 1/ 3YR 10 1/ 3YR 6 1/ 3YR 3 1/ 3YR 1 1/ 3Limits available to you after 25 years of occurrencepolicies. Subject to any payments of claims.25 YRTOTAL 1/ 3Limits available to you after 25 years of claimsmade policies. Subject to any payments of claims.
Did you know?Claims-made policies increasein price each year for the first 5years until the rate is “mature,”after which the annualpremium is very close to thatof an occurrence policy.EXAMPLEOver the course of a 30-year career,an oral and maxillofacial surgeon willtreat approximately 135,000 patients,presenting 135,000 opportunities for apatient to allege malpractice. With tailcoverage, a single set of limits coversback to the retroactive date. This meansthe oral and maxillofacial surgeon willhave only one set of limits (for example, 1 million/ 3 million) to pay all potentialmalpractice claims that are made duringthe extended reporting period (basedon all the incidents that occurred overan entire 30-year career).In contrast, if the same oral andmaxillofacial surgeon had purchasedoccurrence coverage each year for thesame 30-year period, he or she wouldhave 30 separate sets of limits over thesame time span — one for each policyyear.With regard to tail coverage, limits maydiffer according to the policy provisions.In some instances, the tail coverage (orextended reporting period) will havelimits that are reinstated and equal tothose limits in effect during the mostrecent policy period. In other instances,the limits of liability are not reinstatedfor the extended reporting period;instead, the tail coverage actuallyshares the limits of liability from themost recent policy period.As another example, some carriersmay set the limits of liability for yourextended reporting period to the lowestlimits you had during any of your lastfive policy periods. Be sure to reviewyour policy for the limits of liabilityavailable for tail coverage.15
Patient’s Compensation FundWhat is a Patient’s Compensation Fund, andhow does a state-mandated cap on damagesaffect policy limits?A number of states have established a Patient’s Compensation Fund (PCF), which is designedto increase availability and/or affordability of healthcare liability insurance. Of those states,Indiana and Louisiana have unique policy limit options for oral and maxillofacial surgeonsparticipating in the PCF.LOUISIANAPolicy Limits 250,000/ 750,000Fund Limits 1 million/ 3 millionIn Louisiana, your malpracticeinsurance company and thePCF work together. Oral andmaxillofacial surgeons in Louisianapurchase malpractice insurance witha 100,000 per claim/occurrencelimit and 300,000 aggregatelimit of liability from an insurancecompany. If a claim arises withdamages above these amounts,the PCF will provide excesscoverage up to 400,000, plusmedical expenses. Your malpracticeinsurance company will submit yourPCF surcharge to the Louisiana PCF.INDIANAIn Indiana, your malpractice insurancecompany and the PCF work together.Oral and maxillofacial surgeons inIndiana are insured by a malpracticeinsurance company for 250,000 perclaim/occurrence and 750,000 in theaggregate limit. If you participate inthe PCF, you also receive an additional 1 million per claim/occurrence fromthe PCF. Your malpractice insurancecompany will submit your PCFsurcharge to the Indiana PCF.Policy Limits 100,000/ 300,000Fund Limits 400,00016
ARE THERE ANY OTHER STATES WITH LIMIT REQUIREMENTS?Many other states require minimum limits of liability for oral and maxillofacial surgeons.In some states, minimum limits are not required, but maximum damages caps are set.HOW DOES A STATE-MANDATED CAP ON DAMAGES AFFECT POLICY LIMITS?EXAMPLEIn Virginia, the cap for malpractice damages for oral and maxillofacial surgeons is 2.20 million,effective July 1, 2015. The cap is adjusted annually by 50,000 until the total cap reaches 3million, which will be in 2031. Most oral and maxillofacial surgeons in Virginia select a limit ofliability equal or greater than the cap of damages. Check with your personal attorney beforechoosing a limit of liability.17
Consent to SettleWhat is consent to settle?Your policy sets forth the rights, duties, and obligations of both the insurer andthe insured with regard to settlement of a claim. This part of the policy is typicallycalled the consent to settle provision. You will typically find your consent to settleprovision embedded in your malpractice policy’s language.Marketing material or company philosophy may state you have rights, but you shouldinvestigate the actual policy language to determine if you have a pure consent tosettle clause. A pure consent to settle provision will require the insurance company toobtain your approval before settling any claim. There are no exceptions and no stringsattached. Instead of a pure consent to settle provision, you may find exceptions thatgive all authority regarding settlement back to the insurance company.will not compromise anyclaim hereunder without theconsent of the insured.pure consentMedPro’s consent provision18
Common consent to settle exceptions01050206HAMMER CLAUSEIf you refuse to consent to a settlementand elect to contest or continue tocontest a claim, the company’s liabilityfor loss shall not exceed the amountfor which they could have settled suchclaim had you consented, plus claimexpenses incurred prior to the time thecompany made such recommendation.0304BOARD APPROVALYou have consent authority as long asthe company’s review panel or boardagrees with you that your performancemet the standard of care. If theydisagree, the board assumes consentauthority on your behalf.NO LONGER INSURED BYTHE COMPANYYou have consent authority unlessyou are no longer insured by thecompany at the time settlement ortrial occurs.LICENSE SUSPENDEDYou have consent authority unlessyour professional license has beensuspended, revoked, or surrenderedat any time during the claim process.0708UNREASONABLEYou have consent authority unlessthe insurance company deems youunreasonable in withholding yourconsent.BINDING ARBITRATIONYou have consent authority unless thecompany disagrees, at which time theysubmit your refusal to consent to bindingarbitration.UNAVAILABLE OR CANNOTBE LOCATEDYou have consent authority unless thecompany cannot locate you or you areotherwise unavailable at the time ofsettlement or jury trial.DECEASED OR INCOMPETENTYou have consent authority unless youare deceased or deemed incompetent.Key TakeawayMake sure you understand how yourinsurance company defines consent. If anyof the above conditions or exceptions arepresent, your policy does not have a pureconsent to settle provision.19
Entity Coverage (Covering Your Practice)It is important to know that, just like you, yourpractice can be named in a malpractice lawsuit.If you are planning on owning a practice, youshould consider two important coverageoptions: separate limits or shared limits.Separate Limits CoverageIf you own all or a portion of your practice,your practice may be eligible for an entitymalpractice insurance policy with separatelimits of liability. This allows defense costsand indemnity payments to be paid onbehalf of your practice — separately fromyour individual policy limits.Shared Limits CoverageIf you have a solo corporation or are theonly one in your practice, own 100% ofyour practice, and have no employed orcontracted oral and maxillofacial surgeons,dentists or dental specialists, then youmay request to share your individualpolicy limits with your practice. This meansdefense costs and indemnity payments willbe paid on behalf of both you and yourpractice under one shared set of limits.20
Notes:21
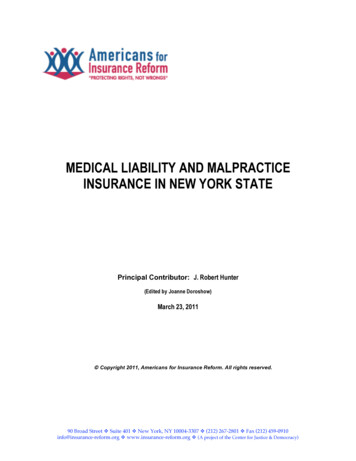
Malpractice ClaimsWhy should I care how a malpractice claimmade against me is handled?An oral and maxillofacialsurgeon in the United States issued, on average, four times inhis or her 30-year career (moreor less depending on locationand scope of practice).4 Itis important to rememberthat your premium dollarsare paying for the insurancecompany’s claims defense.After all, settlement of a claiminvolves more than money — itcan have a long-term negativeeffect on your reputation,practice, license, mobility, andfuture 11%Top allegations for oraland maxillofacial surgeryFailure toDiagnose6%Implant 1%4%Cosmetic &Esthetic wnThese charts show whichprocedures lead to the mostmalpractice allegations, and theaverage indemnity associatedwith each (based on closedclaims analysis).5Average indemnity ofdental and oral surgeryDentoalveolar45,209 9,333Endodontic Treatment 52,46445,086Orthognathic Surgery 57,500TMJ 57,464Failure to Diagnose Implant Anesthesia20,000 Cosmetic & Esthetic Surgery 13,500422Medical Protective internal data. 5 Medical Protective Closed Claims Analysis, 2003-2012.
What types of situations lead to malpractice claims?When many think of malpractice, they think ofthe potential for a million-dollar verdict that couldcripple their reputations and ruin them financially.Here are a few examples of situations that have ledto large malpractice claims.Surgery negligence resulting in disfigurement and the patient’s jaw being fused shut. Verdict: 14.8 million5Complications from wisdom tooth extractions resulting in death. Verdict: 11 million6Failure to diagnose oral cancer. Verdict: 15 million7Severe nerve damage during wisdom tooth extraction. Settled for: 425,0008Negligence in third molar extraction (failure to obtain informed consent resulted in liability). Settled for: 9.8 million9Unethical treatment of osteomylitis resulting in death. Verdict: 1.8 million10Key TakeawayThere certainly is a tangible riskfor these “exceptional events.”However, the most commonmalpractice claims come fromroutine procedures performed inoffices every single day.Medical Protective internal data. 6 http://www.nj.com/news/index.ssf/2009/03/oral surgeon guilty of medical.html p?id 1202551566212&Medmal cap blocks 15 million jury verdict&slreturn 20130914063607 ttlement/ 9 http://www.drbicuspid.com/index.aspx?sec sup n&sub rst&pag dis&ItemID 311697 10 tudy-on-oral-maxillofacial-surgeon/523
Claims DefenseDo all insurance companies handle the defenseof malpractice claims the same way?The short answer is no. It is extremely important to select an insurancecompany that has expertise in malpractice liability litigation. They shouldunderstand the venue, specific state laws, as well as clinical issues and howthey apply to the laws of your state.THE SUCCESSFUL DEFENSE OFMALPRACTICE LAWSUITS REQUIRESA CLAIMS TEAM WITH: An understanding of the scope of malpractice asdetermined by professional societies and/or statelicensure boards A grasp of technical clinical concepts Access to highly qualified experts The financial resources necessaryto aid an aggressive defense Expert knowledge of the lawMock TrialTo get a sense for what a malpracticetrial experience is really like for an oraland maxillofacial surgeon, visitwww.medpro.com/mock-trial-omsThe strongest malpractice insurance coverage will not only provide superb defense in alawsuit, but also arm you with tools to help prevent a lawsuit in the first place.Key TakeawayYou are purchasing theinsurer’s promise to defendyou and pay for damagesshould you be sued. Nothingis more important than yourconfidence that your insurancecompany will provide you withthe strongest claims defense24
Risk Management 101RISK0202
Risk Management 101
What is Clinical Risk Management?Risk management is a process by whichan individual or organization assesses theirenvironment to identify challenges that couldpotentially lead to a “loss.”Many oral and maxillofacialsurgeons may beconvinced that clinicalcompetence is the mostimportant element of asuccessful practice.While it is certainly importantto practice within the standardof care, communication skills,business acumen and a professionalmindset are equally important. Thefollowing section provides a brief list ofrisk management considerations thatmay prove useful for the newly-graduatedoral and maxillofacial surgeon.Did you know? oss comes in a variety ofLforms, including the loss of: Good employees Long-term patients New market opportunities Highly-qualified associates/partners Peer review or disciplinary action Income potential Malpractice lawsuitEvery practice needs a sound riskmanagement program — one that focuseson patient safety and satisfaction.MedPro is committed to supporting itscustomers with risk management productsand services that support this approachand reduce the possibility of financial loss,professional liability exposure and damageto their reputations.27
Why is Risk Management Important?Newly graduated oral and maxillofacial surgeons oftenunderestimate the importance of risk management services.When a patient is in the chair and you are faced with a seriousconcern, it is too late to realize the value of specialized riskmanagement services.HOW WOULD I USE RISK MANAGEMENT?Many times, oral and maxillofacial surgeons call their malpractice companies’ riskmanagement teams when an area of concern presents itself. Here are a few scenarios inwhich a risk management team should be able to provide you with guidance:DEALING WITH AN ADVERSE EVENTWhile performing a routine fully impacted thirdmolar extraction, a portion of the tooth breaksoff and cannot be located. How should this behandled from a risk management standpoint?RECORDS MANAGEMENTAn oral and maxillofacial surgeon is runningout of storage space and wants to dispose ofrecords for some inactive patients. Can this bedone, and if so, how should it be completed?CHILD CUSTODY AND TREATMENTAn oral and maxillofacial surgeon is treatingan 8-year-old child for an orthognathiccondition. The mother has been compliantwith instructions, including keeping allappointments. The father of the child hascalled the office and stated he does not wantthe child to receive any further treatment. Maythe child continue to be treated?28NONCOMPLIANCE WITHRECOMMENDATIONSAn oral and maxillofacial surgeon has a patientwith a worsening oral infection as a resultof his poor oral hygiene and noncompliancewith the recommendations. The oral andmaxillofacial surgeon wishes to dischargethis patient from the practice even though heneeds continuing care. How can this beaccomplished without the potential ofabandoning the patient?
10 Ways to Reduce Your Liability RiskBEFORE YOU BEGIN:01Don’t sign anemployment contractor a practice purchaseagreement without first havingit reviewed by an attorney whospecializes in employment law orbusiness transaction law. Whetheryou are joining a practice as anassociate or an independentcontractor, your employmentcontract contains a variety ofimportant contract terms to whichyou will be bound. These includesuch things as the term of yourcontract, your work hours andconditions, your compensationformula, who will pay for yourmalpractice insurance and others. Itis critical that you understand whatyou are signing.02Don’t accept anemployment offerwithout having reviewedthe practice’s documentation andwritten communications. Thismight include a random review ofpatient files, the practice’s policyand procedure manual (includingthe practice’s infection preventionand control manual), the practice’spatient education materials andall of the practice’s standardwritten documents (noncompliancenotices, discharge letters, latepayment reminders, etc.).03Don’t accept anemployment offerwithout having observedthe business and clinical careactivities over the course of atleast one full business day.1 Ideally,you would be able to observe thestaff’s interaction with each otherand with patients. This will give youimportant insights in to whetherthis is a culture in which you will becomfortable.1A review of Personal Health Information may require the guest doctor’s signature on a confidentiality agreement – basically promising thatany patient information he or she obtains during the course of the visit will remain confidential.29
AFTER YOU START:04Have an emergencypreparednessplan. Your planshould contemplate medical,environmental, and violenceemergencies. Periodically conductdrills so that all members of theoffice staff understand theirrespective roles and responsibilitiesin an emergency. Your localemergency services agenciescan be a source of valuableconsultative assistance.05Prepare for difficultconversations inadvance. Don’t assumethat good clinical skills are anadequate substitute for goodlistening, negotiation, and dispute.06Always obtain writteninformed consent totreatment. Informedconsent serves many impo
company they should purchase their insurance.1 New-to-practice oral and maxillofacial surgeons may be poorly 64% of first-time malpractice insurance buyers allow others to either recommend or decide from which malpractice insurance company they should purchase their insurance. 1 Medical Protective internal dental malpractice data, 2013 07 .