Transcription
ActPlanStudyDoA MILLION HEARTS ACTION GUIDETobaccoCessationCHANGE PACKAGE
The Tobacco Cessation Change Package was created by the Centers for Disease Control and Prevention (CDC) with the purpose ofhelping healthcare professionals in outpatient, inpatient, and behavioral health settings, as well as public health professionals whopartner with these groups, to implement systems and strategies that improve care for patients who use tobacco.AuthorsThis document was conceptualized and authored by Brenna VanFrank, MD, MSPH*; Kaitlin Graff, MSW, MPH*; Gillian Schauer, PhD,MPH (McKing Consulting)*†; Rob Adsit, MEd‡; Lauren Owens, MPH (IHRC, Inc.)*; Stephen Babb, MPH*; Danielle McCarthy, PhD‡; AnnaSchecter, MPH*; and Hilary K. Wall, MPH*.ReviewersThe following individuals provided review and feedback on this document: Steven L. Bernstein, MD (Yale Schools of Medicine andPublic Health); Carol Essenmacher, DNP, NCTTP (Battle Creek VA Medical Center); Tim McAfee, MD, MPH (University of Washington,School of Public Health, Department of Health Services; SEED Consulting [Plowshare Group]); Kait Perry, MPH (American Academyof Family Physicians); Sarah Price, MSN-Ed, RN (National Association of Community Health Centers); Nancy Rigotti, MD (TobaccoResearch and Treatment Center, Massachusetts General Hospital and Harvard Medical School); and Catherine Saucedo (Universityof California, San Francisco, Smoking Cessation Leadership Center).Graphic Design and Editorial AssistanceGraphic and HTML design support was provided by Shelby Barnes, MPH, CHES*; Booker Daniels, MPH*; Susan Davis (NorthropGrumman Corporation)*; and Jessica Spraggins, MPH*.Website Hosting AssistanceWebsite hosting support of tools and resources was provided by the National Association of Chronic Disease Directors.We would like to extend special thanks to the following organizations for their willingness to share tools and resources to improvesmoking cessation, as further denoted within the Tobacco Cessation Change Package: American Academy of Family Physicians (AAFP)American College of Cardiology (ACC)American Lung AssociationArizona Smokers’ Helpline (ASHLine)California QuitsCalifornia Smokers’ HelplineCayuga Medical CenterCenter of Excellence for Health Systems Improvementfor a Tobacco-Free New YorkEssentia HealthGroup Health Cooperative of South Central WisconsinHealthyHearts NYCHeart Health Now!Hospitals Helping Patients QuitInstitute for Clinical Systems Improvement (ICSI)Institute for Healthcare Improvement (IHI)Kansas Health FoundationLegacy (now Truth Initiative )MultiCare Health SystemNational Alliance on Mental Illness Kansas (NAMI KS)National Behavioral Health Network for Tobacco &Cancer Control National Cancer Institute (NCI)National Quality Forum (NQF)Navy and Marine Corps Public Health CenterNew York City Department of Health and MentalHygiene (NYC DOHMH)New York City Health Hospitals (NYC Health Hospitals)New York State Department of HealthNew York State Smokers’ QuitlineNorth American Quitline Consortium (NAQC)Northern Lakes Community Mental HealthOklahoma Health Care AuthorityOklahoma State Department of Health, Center forChronic Disease Prevention and Health PromotionOklahoma Tobacco Settlement Trust (OK TSET)Oregon Health AuthorityPartnership for PreventionPlymouth Family PhysiciansSouthwest Orlando Family MedicineSubstance Abuse and Mental Health ServicesAdministration (SAMHSA)Telligen University of California Quits (UC Quits) University of California, San Francisco Schoolsof Pharmacy and Medicine (UCSF Schools ofPharmacy & Medicine) University of California, San Francisco, SmokingCessation Leadership Center (UCSF SCLC) University of Colorado, Anschutz Medical Campus(CU Anschutz Medical Campus) University of Maryland School of Medicine(UM Medicine) University of Wisconsin Health (UW Health) University of Wisconsin – Madison, School ofMedicine and Public Health (UW-Madison SMPH) University of Wisconsin Center for Tobacco Researchand Intervention (UW-CTRI) US Department of Veterans Affairs (VA) Wisconsin Hospital Association Wisconsin Nicotine Treatment Integration Project(WiNTiP)For More InformationSuggested CitationBrenna VanFrank, MD, MSPHOffice on Smoking and Healthbvanfrank@cdc.govCenters for Disease Control and Prevention. Tobacco CessationChange Package. Atlanta, GA: Centers for Disease Control andPrevention, US Department of Health and Human Services; 2020.Centers for Disease Control and PreventionUniversity of Washington, School of Public Health, Department of Health Services‡University of Wisconsin, Center for Tobacco Research and Intervention*†
CHANGE PACK AGE iiiForeword from the Surgeon GeneralAs the nation’s doctor, I’m committed to advancing the health of the American people. Tobacco useremains the number one cause of preventable disease, disability, and death in the United States.Smoking harms nearly every organ of the body and causes multiple chronic diseases. Nearly one inseven American adults currently smokes cigarettes. Depending on the composition of your practiceor clinic, this number may be even higher, given the marked disparities in smoking that exist acrosspopulation groups. But the good news is that most adults who smoke want to quit and that, every year,more than half make a serious quit attempt. As health care professionals, we can and must do more tohelp them quit smoking for good.Research shows that any health care professional, in any type of care setting, can help motivate a personto make a quit attempt and connect them to resources that can help. Research also shows that patientsexpect health care professionals to address their tobacco use and that their overall satisfaction withcare increases when tobacco dependence treatment is addressed. Therefore, health professionals in allmedical disciplines and in all health care settings should encourage their patients to quit smoking andconnect them to proven treatments shown to increase the likelihood of success. This is true whetheryou work in primary care or a subspecialty; in outpatient, inpatient, or behavioral health; or in acute orlong-term care.You may be asking yourself where you can find the time in your already busy day to address tobaccocessation. As a clinician myself, I am acutely aware of the many demands on your time and on ourhealth care systems. The good news is that Million Hearts has a suite of tools to make it easier foryou to integrate tobacco dependence treatment into your routine care delivery. Putting processesin place can mitigate the burden on individual clinicians and ensure this critical health issue is beingaddressed systemwide.The Million Hearts Tobacco Cessation Change Package provides a list of evidence-based processimprovements clinicians and health systems can implement to deliver optimal treatment to patientswho use tobacco. It contains road-tested resources, shared by health systems and clinicians, thatyou can adapt to fit your setting and patient population. The change package complements existingprotocols and guidance, creating a suite of practical materials you and your team can put into action.As health care professionals, we strive to save lives and help people get and stay healthy. Addressingtobacco use with your patients is an essential step to accomplishing that mission, and the toolsprovided by Million Hearts can help you get there.Jerome M. Adams, MD, MPHVice Admiral, U.S. Public Health ServiceSurgeon General
ContentsTobacco Cessation Change Package — Quick Reference . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1The Importance of Treating Tobacco Use and Dependence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3About the Tobacco Cessation Change Package . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Figure 1. Tobacco Cessation Change Package Focus Areas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4How to Use the Tobacco Cessation Change Package . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Figure 2. Institute for Healthcare Improvement (IHI) Model for Improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5How to Measure Quality Improvement Efforts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Figure 3. Example of a Run Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Change Concepts, Change Ideas, and Tools and Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Table 1. Key Foundations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Table 2. Equipping Care Teams . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Table 3. Screening . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Table 4. Treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Table 5. Referral and Follow-Up . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Appendix A: Additional Resources for Quality Improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Appendix B: Additional Resources for Electronic Health Records Changes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Appendix C: Case Studies in Health Systems Change for Tobacco Cessation Interventions . . . . . . . . . . . . . . . . . . . . . . 25Appendix D: Resources for Community-Level Tobacco Prevention and Control Strategies. . . . . . . . . . . . . . . . . . . . . . . 25Acronyms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Website addresses of nonfederal organizations are provided solely as a service to readers. Provision of an address does notconstitute an endorsement for this organization by CDC or the federal government, and none should be inferred. CDC is notresponsible for the content of other organizations’ web pages.
CHANGE PACK AGE 1Tobacco Cessation Change Package — Quick ReferenceFocus AreasKeyFoundationsEquippingCare TeamsScreeningTreatmentReferral andFollow-UpChange Concepts and Change IdeasKey FoundationsApproaches and tools to assess the current status of tobacco dependence treatment in your practice or system and to make tobaccodependence treatment a priority.Make Tobacco Cessation a Practice and System PriorityIdentify one or two key champions and assemble a multidisciplinary teamAs a multidisciplinary group, conduct an assessment of your clinic/system and develop an action plan to address the current gapsAdopt or update a unit, practice, or system-wide policy to reflect prioritization of tobacco treatmentCreate a Supportive Environment for CessationImplement and strengthen hospital or clinic-wide tobacco-free or smoke-free campus policiesLeverage mass-reach media campaigns to encourage and normalize quitting (e.g., with media in waiting rooms, throughout clinicor hospital system)Support employees and their family members in quitting smoking by providing health benefits for tobacco cessationEquipping Care TeamsApproaches and tools to prepare and motivate healthcare staff to consistently address tobacco use.Equip All Staff to Engage in Tobacco Cessation EffortsAdopt a clinician/staff training policy to train and retrain staffConduct onboarding and annual trainings on tobacco policies, systems, and proceduresOptimize billing practices by leveraging existing codes to capture all billable servicesProvide Clinician and System-Level Feedback on Progress and ImpactSet and communicate specific, measureable performance and quality goalsMake tobacco cessation a quality improvement measure at the clinician or system levelTrack clinician, clinic, hospital, and system performance to provide feedback to clinicians and decision-makers
2 TOBACCO CESSATIONScreeningApproaches and tools that promote consistent universal screening for tobacco use (i.e., asking about tobacco use) as a prerequisite forintervening with patients or clients who use tobacco.Make Tobacco Use a Vital Sign: Screen Every Patient for Tobacco Use at Every VisitAdopt a tobacco use screening protocolEstablish a workflow and determine roles for tobacco use screening and documentationEmbed a tobacco use status prompt in the EHR or other patient record-keeping systemEmbed decision support scripts for screening into the EHR or other patient record-keeping systemTreatmentApproaches and tools to help ensure that patients or clients who use tobacco are consistently advised to quit, assessed for willingnessto make a quit attempt, and offered assistance in quitting tobacco use.Establish a Tobacco Treatment ProtocolImplement a treatment interventionEstablish a workflow to determine roles for delivering the treatment interventionEnhance Clinical Decision SupportEmbed treatment intervention prompts into the EHR or other patient record-keeping systemEmbed decision support scripts for each intervention step into the EHR or other patient record-keeping systemImplement standard order sets for counseling and medicationAdopt tools to guide medication selectionImplement Standardized Approaches to Support Cessation EffortsDeliver standard patient education regarding cessation medicationAdopt a clinical decision support tool for helping patients plan their quit attemptReferral and Follow-UpApproaches and tools for arranging follow-up for patients or clients who use tobacco and for providing referral to internal or externalresources that can serve as an adjunct to treatment provided by the clinician.Establish Protocols to Identify and Connect Patients to Referral ResourcesImplement a protocol or workflow to ensure clinician follow-up with patientsIdentify and partner with referral services that can serve as an adjunct to careSet up direct referrals to internal and external resources by creating standard referral ordersEstablish two-way communication with referral services to get information on whether referrals were accepted by the patientEmploy Population Management Strategies to Better Identify and Reach Patients Who Use TobaccoUse tobacco registries or other methods to track patients who use tobaccoConduct proactive follow-up with patients who use tobacco
CHANGE PACK AGE 3The Importance of TreatingTobacco Use and DependenceTobacco use is the leading preventable cause ofdisease and death in the United States and is asignificant driver of healthcare costs.1-3 Morethan 16 million people in the U.S. live with atleast one serious disease caused by smoking.1Additionally, approximately 480,000 deathsand more than 300 billion in healthcare andlost productivity costs are attributable to smokingevery year.1,3 Future smoking-related illnesses,deaths, and costs can be prevented by helpingindividuals who use tobacco to quit.4 Tobaccodependence is a chronic, relapsing conditionthat often requires repeated interventionand long-term support.5 Evidence-basedtreatments, including counseling and FDAapproved medications, are available4-9 but areunderutilized.4,10-15E-cigarettesE-cigarettes have potential to benefit nonpregnant adults who smoke if used as acomplete substitute for smoked tobaccoproducts, such as cigarettes. However,these products are still fairly new, andevidence on their long-term health effects,as well as their potential effectivenessas a cessation aid, is still developing.4,27E-cigarettes are not currently approved bythe FDA as a smoking cessation aid, andmany adult e-cigarette users continue toalso smoke cigarettes (known as dual use).Additionally, there is little current evidenceabout how to help people quit e-cigaretteuse. For more information, visit www.cdc.gov/e-cigarettes.Clinicians play a critical role in deliveringcessation support; at least 70% of persons whosmoke see a physician each year.5 Patients expectphysicians to address tobacco use, and consistentinterventions from clinicians improve patientoutcomes.5 Even brief advice to quit from aclinician increases quit rates, and more intensiveclinical interventions have progressively greaterimpact.5 In addition to the patient-level benefits,addressing tobacco use and dependence inhealth systems is cost-effective across a varietyof settings,16-18 can help meet certain qualitymeasures,19-21 can reduce rehospitalizationand readmission,22-24 and can increase patientsatisfaction with the care they receive.25,26Integrating tobacco dependence treatmentinto routine clinical care policies, protocols, andsystems can help clinicians deliver effectivecessation interventions.About the Tobacco CessationChange PackageThe Tobacco Cessation Change Package (TCCP)presents a list of process improvements thatclinicians can implement as they seek to deliveroptimal treatment to patients who use tobacco.§It was developed to give clinical teams a practicalresource to increase the reach and effectivenessof tobacco cessation interventions and toincorporate these interventions into theclinical workflow.The TCCP is intended to be used by healthcareprofessionals in outpatient, inpatient, andbehavioral health settings. The TCCP is nota comprehensive clinical guide on treating§The primary focus of the TCCP is cessation from combustible tobacco products, since the burden of death and disease from tobacco use inthe U.S. is overwhelmingly caused by cigarettes and other combusted tobacco products.1 However, some tools and resources in Tables 1–5address non-combustible product use, and the Million Hearts Clinician Action Guide contains some guidance on addressing the use ofother tobacco products.
4 TOBACCO CESSATIONThe TCCP is composed of change concepts,change ideas, and tools and resources. Changeconcepts are general notions that are useful fordeveloping more specific strategies for changinga process. Change ideas are actionable, specificideas or strategies that can be rapidly tested ona small scale to determine whether they resultin improvements in the local environment. Eachchange idea is linked to evidence- or practicebased tools and resources that can be adoptedor adapted to implement each change idea.tobacco dependence; rather, it is designed tocomplement other Million Hearts tools: Tobacco Cessation Intervention Protocol Clinician Action Guide on Identifying andTreating Patients Who Use TobaccoWhereas the Protocol and Action Guide focuson the content of clinical interventions, the TCCPfocuses on how to implement such interventionsat a systems level.The purpose of the TCCP is to helpmultidisciplinary healthcare teams put systemsand strategies in place to more efficiently andeffectively integrate treatment of tobacco useand dependence into routine clinical care. TheTCCP is broken down into five main focus areas(Figure 1), which are mapped to the 5As tobaccointervention framework: Ask all patients abouttobacco use at every visit/admission; Advise allpatients who use tobacco to quit; Assess thepatient’s willingness to make a quit attempt;Assist the quit attempt with counseling andmedication; and Arrange follow-up.5The Evolving 5AsAdditional models for treatmentimplementation have evolved sincedevelopment of the 5As. Ask, Advise, Refer(AAR) and Ask, Advise, Connect (AAC)emphasize connection of patients totreatment extenders. Opt-out treatmentmodels are also increasingly utilized;one example of an opt-out model is theAmerican College of Cardiology’s (ACC)Pathway for Tobacco CessationTreatment.28Figure 1. Tobacco Cessation Change Package Focus AreasKeyFoundationsEquippingCare TeamsScreeningTreatmentAskAdvise,Assess, AssistReferral andFollow-UpArrange
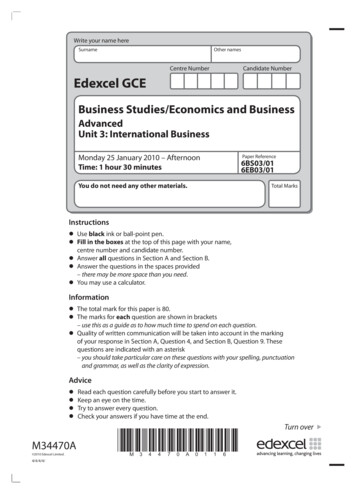
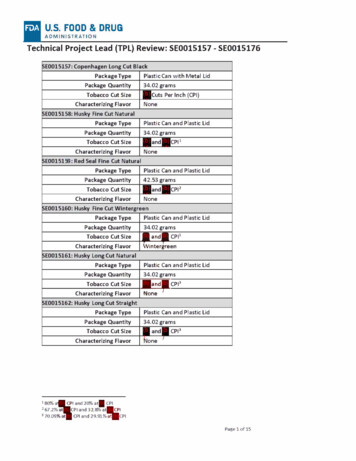
CHANGE PACK AGE 5How to Use the TobaccoCessation Change PackageThe TCCP offers a menu of options that cliniciansand practices can choose from based on theirspecific circumstances and needs. We do notrecommend that any healthcare practice attemptto implement all the interventions described inthe TCCP at once, nor is it likely that all of theseinterventions will be applicable to everyclinical setting.We recommend that you start by bringingtogether a multidisciplinary team of stakeholders(e.g., physicians, pharmacists, nurses, medicalassistants, social workers, care managers, qualityimprovement coordinators, health informaticians,and administrators). The team can look at theelements in Figure 1 and conduct an assessmentto determine the aspects of tobacco dependencetreatment that are most in need of improvementin your health system. You may also benefit fromtalking directly with others who have undertakensimilar efforts to learn from their experience.Once your team has identified and prioritizedthe needs, interventions can be selected fromthe TCCP to create a supportive treatmentenvironment to address those needs.change”) to assess feasibility and allow the teamto evaluate and adjust before instituting thechange on a broader, more permanent scale. Thisapproach can be accomplished using Plan-DoStudy-Act (or PDSA) cycles.Figure 2. Institute for Healthcare Improvement(IHI) Model for ImprovementWhat are we tryingto accomplish?How will we knowthat a change is animprovement?What changes can wemake that will resultin improvement?Figure 2 depicts the Institute for HealthcareImprovement (IHI) Model for Improvement.29This model suggests posing three questions:1.What are we trying to accomplish?2.How will we know that a change isan improvement?3.What changes can we make that willresult in improvement?The answers will point you to your qualityimprovement objectives and related metrics.You can then choose strategies from the TCCPthat have been shown to result in improvement.Each strategy you choose should first be testedon a small scale (i.e., conduct a “small test ofActPlanStudyDo
6 TOBACCO CESSATIONTables 1 through 5 contain a list of changeconcepts and change ideas that clinicians,practices, and systems can implement toenhance their delivery of tobacco cessationinterventions. Each change idea is paired withpractical tools and resources provided by expertsin the field who have successfully used them.Each tool has a key to indicate its applicablesettings (i.e., outpatient, inpatient, behavioralhealth, or multiple settings). Key Foundations (Table 1) includesapproaches and tools to assess the currentstatus of tobacco dependence treatment inyour healthcare practice or system and tomake it a priority. This is likely a good place tostart quality improvement efforts related totobacco cessation interventions. Equipping Care Teams (Table 2) includesapproaches and tools to prepare and motivatehealthcare staff to consistently addresstobacco use. Screening (Table 3) includes approachesand tools that promote consistent universalscreening for tobacco use (i.e., asking abouttobacco use) as a prerequisite for interveningwith patients or clients who use tobacco. Treatment (Table 4) includes approaches andtools to help ensure that patients or clientswho use tobacco are consistently advised toquit, assessed for willingness to make a quitattempt, and offered assistance in quittingtobacco use. Referral and Follow-Up (Table 5) includesapproaches and tools for arranging follow-upfor patients or clients who use tobacco andfor providing referral to internal or externalresources that can serve as an adjunct totreatment provided by the clinician.Additional resources can be found inthe appendices: Appendix A provides resources forquality improvement. Appendix B contains resources forworking with electronic health records. Appendix C highlights case studiesin health systems change for tobaccocessation interventions. Appendix D provides resources forengaging in community-level tobaccoprevention and control strategies.The tools in this TCCP have been successfullyused in the field to systematize and improvethe delivery of treatment for tobacco useand dependence. Some clinical details incertain tools may reflect models of treatmentand management that differ from thosein your practice. You may need to modifythese tools to adapt them to your patientpopulation and practice. In addition, becausethe science of treating tobacco use anddependence continues to evolve, some toolsmay become outdated over time. The TCCPwill be periodically updated accordingly.
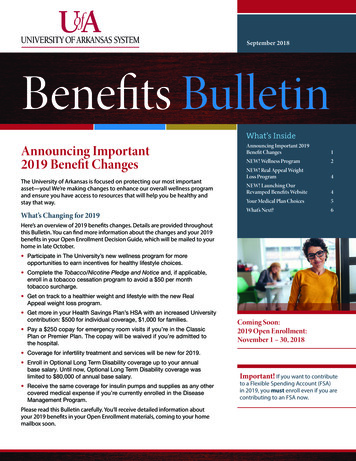
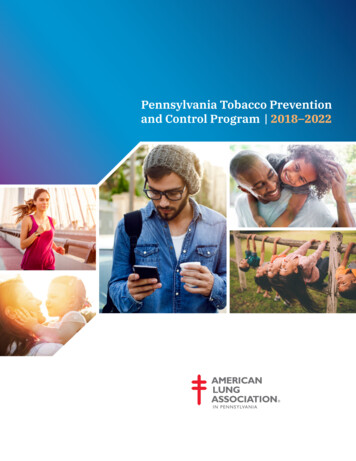
CHANGE PACK AGE 7How to Measure QualityImprovement EffortsMonitoring and measuring quality improvementefforts, including both outcomes and processes,is essential. Process measures, such as theproportion of patients who use tobacco and areoffered treatment and follow-up, can provideearly indications of whether interventions arebeing successfully carried out. Longer-termoutcomes, such as reduced prevalence of tobaccouse in the system’s patient population, can alsoprovide valuable feedback. You can begin bycollecting baseline data on a process you areseeking to improve. Then test your change ideason a small scale in order to identify potentialbarriers to implementation. This approach allowsclinical staff to make needed refinements toaddress these barriers before implementingthe change idea on a broader scale.One very helpful tool for monitoring efforts is arun chart. A run chart is a graph that displaysperformance on a process or outcome over time.It can help show decision makers and otherstakeholders why recommended changes areneeded. You can then use the chart to documentwhen specific changes were made in order toshow how these changes impacted performance(Figure 3). See Appendix A for additional qualityimprovement tools and resources.Figure 3. Example of a Run ChartPercent of Eligible Patients Counseled on Cessation Medication, Clinic A,March–December 2019Cessation medicationorder set and clinicaldecision supportimplemented in EHR100%90%80%70%60%50%CME presentation toclinicians on tobaccouse and dependencetreatment strategies40%30%20%10%0%Mar 2019 Apr 2019 May 2019 Jun 2019Jul 2019 Aug 2019 Sep 2019 Oct 2019 Nov 2019 Dec 2019
8 TOBACCO CESSATIONChange Concepts, Change Ideas, and Tools and ResourcesTable 1. Key FoundationsChange ConceptChange IdeaTools and ResourcesCenter of Excellence for Health SystemsImprovement for a Tobacco-Free NY — SupportingEvidence-Based Tobacco Dependence Screening &Treatment (p. 155)ICSI — Tobacco Health Systems Change StarterToolkit for Clinics (pp. 5–6)Identify one or twokey championsand assemble amultidisciplinary teamUW Health, UW-Madison SMPH, and UW-CTRI— Quit Connect Health: A Specialty Staff Protocolto Improve Referrals to Tobacco Quit Lines(pp. 12–13)UW-CTRI — Treating Tobacco Use and Dependencein Hospitalized Patients: A Practical Guide (p. 9)UCSF SCLC — Destination Tobacco Free: A PracticalTool for Hospitals and Health Systems (p. 19)SAMHSA — Implementing Tobacco CessationPrograms in Substance Use Disorder TreatmentSettings: A Quick Guide for Program Directors andClinicians (p. 8)Make TobaccoCessation a Practiceand System PriorityCenter of Excellence for Health SystemsImprovement for a Tobacco-Free NY — SupportingEvidence-Based Tobacco Dependence Screening &Treatment (pp. 154–160)As a multidisciplinarygroup, conduct anassessment of yourclinic/system anddevelop an actionplan to address thecurrent gaps(continued onnext page)Key:Outpatient:ICSI — Tobacco Health Systems Change StarterToolkit for Clinics (pp. 5–6)AAFP — Treating Tobacco Dependence PracticeManual: A Systems-Change Approach (pp. 4–6, 19)UW-CTRI — Treating Tobacco Use and Dependencein Hospitalized Patients: A Practical Guide (p. 9,Appendix 1)OK Health Care Authority and OK State Departmentof Health, Center for Chronic Disease Preventionand Health Promotion· Primary Care Practice Facilitation Curriculum,Module 12 – An Introduction to AssessingPractices: Issues to Consider· TSET Clinical Practice Self-EvaluationSummaryInpatient:Behavioral Health:Settings
CHANGE PACK AGE 9Table 1. Key Foundations (continued)Change ConceptMake TobaccoCessation a Practiceand System PriorityChange IdeaAs a multidisciplinarygroup, conduct anassessment of yourclinic/system anddevelop an actionplan to address thecurrent gapsAdopt or update a unit,practice, or systemwide policy to reflectprioritization of tobaccotreatmentTools and ResourcesCU Anschutz Medical Campus — Build a ClinicLearning Community: Summary Report andPlaybook (pp. 65–84)KS Health Foundation and NAMI KS —Implementation Self-Assessment: KansasTobacco Guideline for Behavioral Health CareUCSF SCLC — Destination Tobacco Free: APractical Tool for Hospitals and Health Systems(Appendix N)CU Anschutz Medical Campus — DIMENSIONS:Tobacco-Free Policy ToolkitUCSF SCLC — Destination Tobacco Free: A PracticalTool for Hospitals and Health Systems (pp. 2–12,30–31, Appendix C, Appendix D, Appendix M)National Behavioral Health Network for Tobacco &Cancer Control — How to Implement a TobaccoFree Policy InfographicCreate a SupportiveEnviro
The Tobacco Cessation Change Package was created by the Centers for Disease Control and Prevention (CDC) with the purpose of . helping healthcare professionals in outpatient, inpatient, and behavioral health settings, as well as public health professionals who