Transcription
Public health approachesin policingA discussion paperHelen Christmas and Justin Srivastava
College of Policing Limited (2019) Crown copyright - Public Health England (2019)This publication (excluding logos, photographs and third party content) is available for re-use under the Non-Commercial College Licence, except where otherwise stated.Any enquiries regarding this publication please contact us at: contactus@college.pnn.police.uk
ContentsExecutive Summary41. Introduction62. Population Approach93. The ‘causes of the causes’114. Prevention145. Data, evidence base, epidemiologyand outcomes176. Partnerships, communities andsystem leadership197. What can and does it look likein practice?218. Contributors229. References23
Executive Summaryi. IntroductionThe purpose of this resource is to explorewhat is meant by “a public health approach”in the context of policing. It has beendeveloped by an expert reference group ofpolice, public health and voluntary sectorprofessionals based on the existing evidencebase and their expertise and experiences. Itis part of a programme of work to implementthe national Policing, Health and Social CareConsensus.Public health approaches, whilst differentfrom traditional models of response policingwhich often focus on individuals andenforcement, build on police experiences ofneighbourhood policing and problem solving.Public health approaches in policing supportthe Policing Vision 2025, which talks aboutproactive preventative activity, working withpartners to problem-solve, vulnerability,cohesive communities, improving datasharing, evidence-based practice and wholesystem approaches.The idea of applying public healthapproaches to areas such as road safety,drugs and violence is not new; but the termis being used to mean different things and nonationally or internationally agreed definitionsof ‘public health approaches in policing’currently exist.This paper is intended to support police andtheir partners in understanding and applyingpublic health approaches to policing.ii. What are public healthapproaches?Population focusPublic health approaches start with the needsof the public or population groups ratherthan with individual people. This is differentto healthcare where the focus is on the4individual patient, or reactive policing whereofficers respond to calls about individualvictims or perpetrators. Public healthapproaches involve interventions deliveredat population level and targeting resourceseffectively through increased understandingof the population.The causes of the causesTaking public health approaches meanslooking behind an issue or problem or illnessto understand what is driving it. Often called‘social determinants’ or ‘structural factors’,these are the circumstances such as housing,education, indebtedness and income thatunderpin people’s lives and make them moreor less likely to: experience criminal victimisation have poor health outcomes, have lessaccess to health services, and dieprematurely have contact with the police and otherservices; and enter the criminal justice system.PreventionPublic health approaches start from theprinciple that prevention is better than cure.A three-tier approach is often used, whichrecognises that there are opportunities tobe preventative even after a problem hasemerged: primary prevention is preventing theproblem occurring in the first place; secondary prevention is intervening earlywhen the problem starts to emerge toresolve it; and tertiary prevention is making sure anongoing problem is well managed to avoidcrises and reduce its harmful consequences.
Data, evidence and outcomesA key element of public health approaches isskilled use and interpretation of data and theevidence base to ensure that interventionsare designed, delivered and tailored to be aseffective as possible. This links closely to afocus on population outcomes. Both policingand public health share a commitment toevaluation of new or untested interventions.Epidemiology is a quantitative public healthdiscipline which looks at the frequency andpatterns of events in a group of people andwhat the risk and protective factors are. Thisis often the starting point for public healthapproaches to violence prevention, some ofwhich use epidemiology to understand thepatterns of violent events.Partnerships, communities and systemsPartnership is central to public healthapproaches because the breadth ofpopulation need requires response(intervention) across many disciplines andservices. Different partners have access todifferent skills, levers and mechanisms toeffect change. A key public health skill isinfluencing partners to use their time andresources in a way that improves populationhealth, safety and wellbeing, as well asunderstanding and championing communityassets. Public health approaches are alwaysconsciously located within a wider system– which includes communities - rather thanthought of in isolation.iii. Challenges andopportunitiesChallenges to adopting public healthapproaches in a policing context includethe difficulty of evidencing the impact ofpreventative intervention and of investing forlong term outcomes. Using approaches thatare already well-evidenced and evaluatinginterim progress can assist with this.The police cannot tackle the root causes ofproblems at a population level on their ownand understand the benefits of working inpartnership. This is particularly the casewhen demand from the public is risingand the complexity of need is increasinglyrecognised. Over 80% of all calls to thepolice are not about crime, and many relateto issues of vulnerability and people withcomplex social needs.iv. Tools and case studiesExamples of tools and case studies as wellas background reading are available on theEmergency Services Hub.5
1. IntroductionA healthy society is not one that waits for people to becomeill, but one that sees how health is shaped by social, cultural,political, economic, commercial and environmental factors, andtakes action on these for current and future generations.Bibby 2018, p7The test of police efficiency is the absence of crime and disorder,not the visible evidence of police action in dealing with it.Peelian PrinciplesThe purpose of this resource is toexplore what is meant by a publichealth approach in the context ofpolicing. There is currently no singleagreed national or internationaldefinition of public health approachesin policing. It is not a new concept, butit is a developing field and the samephrase is used to refer to a variety ofapproaches: from treating violencelike an infectious disease to holisticupstream population level interventions.This paper brings together differentideas and approaches that have beenshown to work in achieving sharedoutcomes or are similar to otherevidence-based strategies and thereforemay be of use to police forces and theirpartners. Not all are unique to publichealth. Some concepts will be easierto relate to everyday policing activitythan others. Some are about strategicplanning and use of resources; othersare about issues that impact directly orindirectly on police demand but wherepolice forces will want to influence otherpartners to take collective action.The paper has been developed by areference group of policing, public healthand third sector professionals, to reflectthe current evidence base and their6collective organisational and personalexpertise. It is part of a programme ofwork to implement the national Policing,Health and Social Care Consensus.Definitions andstarting pointsThe UK Faculty of Public Health’sdefinition of public health is:“the art and science of preventingdisease, prolonging life and promotinghealth through the organized efforts ofsociety” (Acheson 1988).The World Health Organisation(WHO) defines health as:“a state of complete physical, mentaland social wellbeing and not merely theabsence of disease or infirmity”(WHO, 1948).This definition has been criticised forbeing mostly unachievable – but thepoint is that health is not just a medicalconcept, it is much broader. The work ofpolicing impacts directly and indirectlyon health; and health conversely impactsboth directly and indirectly on policing (egGilmour 2018, van Dijk 2019,Anders 2017).
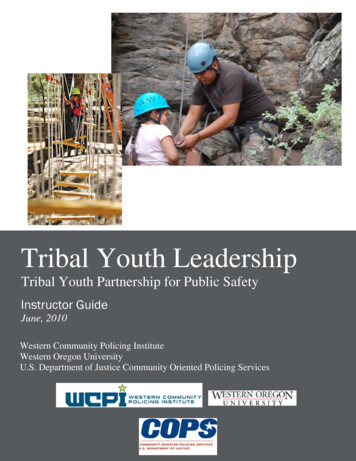
The mission of policing is:“to make communities safer by upholding the law fairly and firmly;preventing crime and antisocial behaviour; keeping the peace;protecting and reassuring communities; investigating crime andbringing offenders to justice” (NPCC 2016).BACDEVIDENNTIONIOEVENTC AU S E SPREVENOPARTN E R S HIPPOFTESNAPRRY PRIMAH E C AUSARYONDSEC ENTIONVERPED ATAIARYTERT NTIONVEPRESEThis paper takes five elements that are common to public healthapproaches and applies them to a policing context:PU L TIONA7
Why should we consider public health approaches?The Policing Vision 2025 is a ten-year plan for policing. It talks about “increasingly diverseand complex [communities], necessitating a more sophisticated response to the challengeswe face now and in the future” (NPCC 2016, p2) with the public at the heart of this. Theguidance it gives on how local policing should react to this is aligned with public healthapproaches (p7): Ensuring policing is increasinglyfocused on proactive preventativeactivity as opposed to reacting to crimeonce it has occurred. Working with our partners to helpresolve the issues of individuals whocause recurring problems and crime inthe communities they live in; reducingthe requirements that these peopleplace on the public sector and policingspecifically. Using an improved understandingof vulnerability, both in physicaland virtual locations, as a means ofimproving and differentiating serviceand protection. This may meanadapting to evidence of what workslocally in targeting vulnerability andareas of high demand and need. Supporting multi-agencyneighbourhood projects that build morecohesive communities and solve localproblems - it will often not be realisticfor police to play the central role.These initiatives must be enhancedby working with the Government toensure projects are not undermined bydiffering boundaries, multiple serviceproviders and incompatible datasharing policies. Improving data sharing and integrationto establish joint technologicalsolutions and enabling the transferof learning between agencies andforces so we can work more effectivelytogether to embed evidence basedpractice, especially those determinedby partners such as academia andthe College of Policing. We mustunderstand the wide ranging concernsof citizens and be able to communicateacross all forms of public contact(including new technologies and socialmedia), which will require significantanalytical and forecasting capabilities,which must be reflected within theworkforce. Working with partners to foster aculture shift around the deliveryof public protection, away from asingle organisation mentality towardsbudgeting and service provision basedon a whole-system approach, poolingfunds where appropriate to achievecommon aims for the benefit of thepublic.The key concepts from the above list are: proactive preventative activity, working with partners toresolve issues (problem-solving), understanding of vulnerability, cohesive communities, improvingdata sharing, evidence-based practice, and whole-system approaches. These are central tenetsof public health approaches in policing.8This common purpose around improvingpeople’s lives and preventing harm isrecognised (and formalised) in the nationalPolicing, Health and Social Care Consensus,which was published by the National PoliceChief’s Council in 2018. It sets out a jointcommitment to prioritising preventionand improving collaborative working tosupport vulnerable people. Supporting theimplementation of public health approachesin policing is one of the workstreams of theConsensus.Public health approaches in policing offera different lens to understand what liesbehind the increasing recognition thatfocusing on crisis is not cost-effective(EIF 2016) and cannot on its own reducedemand. They also provide a way forwardto realise the commitment to proactivepreventative activity.
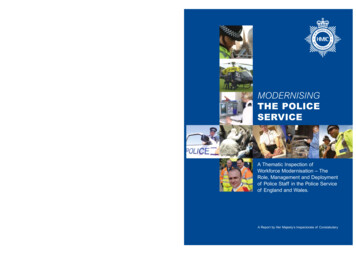
2. Population approachPublic health approaches start with the needs of the public or population groups rather thanwith individual people. This is different to healthcare where the focus is on the individual patient,or reactive policing where officers respond to call about individual victims or perpetrators.This wide lens helps to capture the bigger picture – including the different repercussions orpotential impact from an event or issue and the people who are or might be involved. It is alsovital for understanding outcomes. This may involve interventions delivered at population level ortargeting resources effectively through increased understanding of the population.Taking a step back and asking “who, what,where, when, how, why” type questionshelps to understand an issue as fully aspossible from different perspectives and avoidunintended consequences or assumptionsbased on a small number of experiences.Sometimes action that might help to achieveone aim can undermine progress for othergroups. For example, putting up barriers toprevent motorbikes getting onto green spacescan sometimes make access harder for peoplewho use wheelchairs or motor scooters, orthose with buggies and prams.Public health approaches maintain a focuson population outcomes, however dependingon the aims and population of interest,interventions may target the whole population(universal) or target specific groups.Population interventionOne important theory behind population levelintervention argues that reducing harm bya small amount across a whole populationgroup is more effective overall at reducing thenumber of ‘events’ than targeted interventionsthat reduce harm by a greater amount inthe highest risk group (Rose 1985). Theclassic example in health is strokes: loweringblood pressure by a small amount acrossthe population as a whole will prevent morestrokes than reducing blood pressure by agreater amount in those with the highest bloodpressure. This is known as “shifting the curve”.An example of a population level or ‘universal’approach in police forces such as LancashireConstabulary (and others, for exampleschools and healthcare) is having traumainformed workforces. These ensure that allstaff understand the impact of trauma, ratherthan restricting this to specialist services forindividuals whose needs have already beenidentified (NHS Education Scotland 2017,pp12-14). It enables a more empatheticapproach, reduces the risk of retraumatising,and increases the likelihood of understandingwhat’s behind the presenting issue.Figure 1: shifting the curveNumber of individualsWhat’s behind this?LowRisk factor e.g. ACE, Drugs,criminal historyHighProactive, population-focused approachesare not new in policing, and there is evidencein support of proactive prevention. GeorgeMason University’s evidence-based policingmatrix (GMU 2018) plots evaluations of policeinterventions according to their type andtheir effectiveness at crime reduction. Thematrix shows that place-based, proactive andspecific approaches generally demonstratebetter results than interventions that are aimedat individuals, are reactive, or are more generalin focus (Lum 2011).9
Targeted intervention aspart of a wider strategySometimes interventions need to betailored and proactively targeted atparticular high risk groups with specificneeds, for example, repeat domesticabuse perpetrators (for example ProjectMirabel). The Devon strategy to enddomestic and sexual violence and abuse2016-21 demonstrates well how thistargeted approach fits within a widerpopulation approach (DSVA 2016, p26).Other examples of targeted interventionsare available from the College of Policing’scrime reduction toolkit.Inequality andeffectivenessSome groups are more disadvantaged thanothers, and public health approaches willalways monitor the impact for the widerpopulation and aim to reduce inequalityrather than widen it. The publicationRebalancing Act sets out in detail howhealth and social inequality can impact onpeople in contact with the criminal justicesystem (Anders 2017).Public health approaches look for abalance between universal and targeteddelivery. To avoid achieving improvementsfor some people but leaving othergroups behind, services should ideallybe available to all but weighted moreheavily to those with the greatest need.This is known as “proportionateuniversalism” (Marmot 2010).10Careful design and evaluation ofinterventions based on a goodunderstanding of population needand assets (such as skills, resources,knowledge, capacity, enthusiasm andexperience) is key. Community involvementis central to making sure an interventiondoes not miss the mark (Myhill 2012).
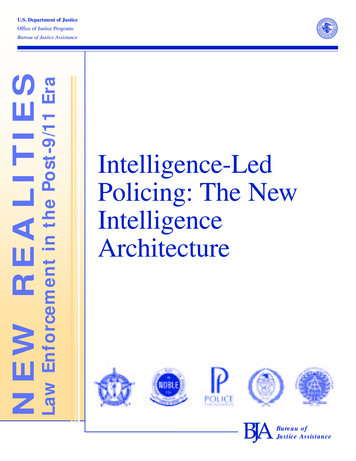
3. The ‘causes of the causes’Public health approaches look behind an issue, problem or illness to understand what is drivingit. Often called social determinants or structural factors, these are the circumstances such ashousing, education and income that underpin people’s lives and make them more or less likely to: experience poor health outcomes, criminal victimisation and premature death have contact with the police and other services; and enter the criminal justice system. (FrameWorks Institute 2018, pp6-12; Bibby 2018).ral and environutlmecu,IncomentACEs/lifeicand workPastalexperiencessmexperexperienceof CJSHousinggIndividual factors: age sexethnicitygenetics Access toservicesPhysical/mentalhealthFamily &sociali l supportCommunitycohesionEducationLifestyleindit onscocioecoonoSFigure 2: Social determinantsLivingConditionsAdapted from the Dahlgren and Whitehead model, 1991What’s behind this?There is good evidence that the circumstances of your life have a cumulative impact on yourlife chances and your life expectancy (Marmot 2010). There is also strong evidence that themore unequal a society is, the worse health and social outcomes it has - such as violenceand incarceration (Wilkinson and Pickett 2009). Social mobility is limited in the UK, so there isalso an intergenerational aspect to social circumstances (Social Mobility Commission 2017).It is important to remember that this evidence is at population level – it does not mean that anindividual is destined for poor outcomes because of their circumstances, but it might meanthey have more barriers to overcome than someone from a less disadvantaged background.College of Policing demand research has identified that over 80% of calls to the police are notdirectly about crime (2015). Many of these are about complex social needs or vulnerability.Understanding and influencing the ‘causes of the causes’ gives policing an opportunity toreduce need and demand from the public, and help achieve its mission.Often, the wider determinants listed may not be for police to tackle directly themselves, andmany police colleagues will already have experience of influencing action collectively with otherpartners through existing local partnerships.11
Sometimes the outcome of interest will be the same for different partners – such as injury fromviolence. Even when it is not, the causes behind police demand or poor health and wellbeingare often an area of common ground when partners start to look at what lies behind the storyof an individual or a group of people.A local policing team in South Yorkshire chose to focus its attention on a particular estate becauseof high crime and anti-social behaviour, and community dissatisfaction with police and other publicservices. They worked with the community to understand their priorities and used a problem-solving methodology to understand the issues, what lay behind them and potential solutions. Togetherwith the community, they developed a series of tailored solutions and crucially were able to securethe involvement of – and action from – other local partners, such as the Housing Association. Theactions included enforcement, target hardening, environmental improvements, use of communitypayback and play activities for children. The team evaluated the impact and improvements includedlarge reductions in police incident demand, large increases in community satisfaction measures,and the initiation of some longer-term projects for young people in the area.Adverse ChildhoodExperiences (ACEs),vulnerability and traumaThe impact of childhood adversity is both apublic health and policing issue and providesa good example of common ground. Areview of collaborative working in Englandand Wales found that the three highestranking issues that police wanted to work onwith health colleagues were homelessness,social isolation and ACEs (PHE 2018).The impact of adversity in childhood hasbeen described in an ‘ACE Model’ settingout 10 specific traumatic events occurringbefore the age of 18 which, given highor frequent exposure can lead to toxicstress, which itself is associated withimpacts including negatively altered braindevelopment (Sweeny 2018).It is important to note that the evidencebase around ACEs is still emerging (Bateson2019). ACEs are not predictive at theindividual level and ACEs do not coverthe whole picture of risk and resilience.However, research in the US and thenEngland and Wales provided population levelevidence that people who have experiencedfour or more ACEs from the specific list havea much greater risk of poor social and healthoutcomes than people who experienced noACEs (Felitti 1998, Bellis 2014). For example,this group are seven times more likely to12have been involved in violence in the lastyear, and eleven times more likely to haveused crack or heroin or been incarcerated(Bellis 2014b). This does not mean thatevery person who experiences ACEs willstruggle in adulthood, or that ACEs are theonly cause of social and health problems.Clearly, preventing ACEs occurring in thefirst place is the best way to prevent theharm they can cause. The most importantmitigating factor to prevent harm developingfrom experiencing ACEs is the bufferingeffect of a supportive relationship with atleast one trusted adult.The Early Action Together (EAT)programme is funded by the PoliceTransformation Fund and run jointly withPublic Health Wales. Its mission is “tofacilitate the transformation of policing inWales to a multi-agency, ACE informedapproach that enables early interventionand root cause prevention” and itoperationalises a public health approachto achieve this. The programme is trainingstaff to build their understanding andconfidence; developing organisationalcapacity; developing a single integrated‘front door’ for vulnerability and workingtowards a whole system approach. Italso has a strong research team. Moreinformation is available from the EATLearning Network
There are also many other adversities and traumas that children can face which were not partof the original ACEs studies, such as racism and bereavement (van Woerden 2018). It can behelpful, therefore, to consider ACEs and their impact as one aspect of wider vulnerabilities thatpeople can experience.Preventing ACEs should be seen within the wider context of tackling societal inequalities.While ACEs are found across the population, there is more risk of experiencing ACEs in areasof higher deprivation. Adverse childhood experiences are therefore often described alongsideadverse community environments as a ‘pair of ACEs’ (Ellis 2017).Figure 3: The Pair of ACEsAdverse Childhood ExperiencesMaternalDepressionPhysical &Emotional NeglectDivorceEmotional &Sexual AbuseMental IllnessSubstance AbuseIncarcerationDomestic ViolenceHomelessnessAdverse Community EnvironmentPovertyViolenceDiscriminationPoor HousingCommunityDisruptionQuality &AffordabilityLack of Opportunity, EconomicMobility & Social CapitalAdapted from Ellis, W., Dietz, W. (2017) A New Framework for Addressing Adverse Childhood and Community Experiences: The Building CommunityResilience (BCR) Model. Academic Pediatrics. 17 (2017) pp.S86-S93. DOI information: 10.1016/j.acap.2016.12.011Public Health England are in the process of publishing Collaborative Approaches toPreventing Offending and Reoffending in Children (CAPRICORN): a resource for the localhealth and justice system to support collaborative working for vulnerable children andyoung people. It describes the importance of understanding health and social care needs,identification of risk and protective factors to support individual and population levelinterventions and supports the development of a whole system approach to tackle complexproblems (PHE forthcoming).Trauma can be thought of as an umbrella term under which ACEs belongs. A trauma-informedapproach will encompass an ACE-informed approach, giving people a common language withwhich to talk about the impact of trauma and adversity, through embedding the approach intomulti-agency organisational thinking (Whitfield 1998).From a service perspective, a trauma-informed approach asks: ‘What happened to you?’ ratherthan, ‘What’s wrong with you?’ and goes on to ask, ‘How has this affected you?’ and ‘Who is thereto support you?’. Several police forces are working with partners to develop these approaches, forexample Lancashire Constabulary is a key partner in the Trauma Informed Lancashire project.13
4. MARY PREVENTIONPublic health approaches start from the principle that prevention is better than cure. A core roleof the police service is to prevent crime, and the phrase “you can’t arrest your way out of ” isoften used: for example, the title of the Local Policing Conference 2019 was, “You can’t arrestyourself out of a crisis”.A hurdle in persuading funders to back a preventative approach is that it is much harder toshow evidence of effectiveness in the short term. This is particularly true when the problemand/or intervention is complex (see Centre for Health Economics 2019).What’s behind this?Public health approaches often use a threetier model which recognises that there areopportunities to be preventative even after aproblem has emerged: primary prevention is preventing theproblem occurring in the first place; secondary prevention is intervening earlywhen the problem starts to emerge toprevent it becoming established; and tertiary prevention is making sure anongoing problem is well managed toavoid crises and reduce its harmfulconsequences.It is also important to note that the sameintervention - for example providing supportto a parent with an alcohol problem - mightbe secondary or tertiary prevention forthem, but at the same time could be primaryprevention for their children.14There is also a long history of the samethree tier model being used in a policingcontext – for example Brantingham andFaust created a conceptual three tier modelfor crime prevention in 1976. The NationalPolice Crime Prevention Strategy outlinesthe aim of preventative policing as, “fewervictims, fewer offences, and less demandon policing achieved by addressing thecauses of crime, utilising sophisticatedpartnership-oriented problem solving”(NPCC 2015). It utilises Brantingham andFaust’s public health model and articulatesthe inputs, outputs, and outcomesassociated with successful delivery.Thames Valley Police and PublicHealth England’s Health and Justiceteam are key partners in “the ReadingModel” which includes a preventionand early intervention strategy andpartnership. The model was developedwith no additional funding. Partners arecommitted to providing holistic supportfor families early on, to prevent issuesescalating.
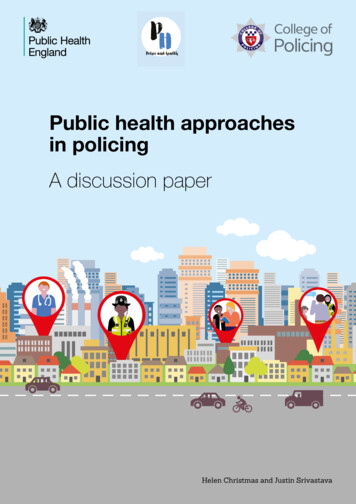
Problem solvingProblem solving or problem oriented policing (POP) is an approach where a problem or issueis examined from different perspectives before potential solutions are identified, implementedand evaluated (College of Policing, 2017b). A four step technique, SARA, is used, and partnerinvolvement is critical.SARA problem solving model: Scanning: the identifiying and prioritising of potential crime and disorder problems Analysis: the analysis of potential problems, by gathering information and intelligenceto identify underlying causes of the problem Response: the development and implementation of tailored activities to address thecauses of the problem, as identified in the analysis phase Assessment: the measurement of the impact of the response to test if it had thedesired effect and to make changes to the response if requiredAlthough POP was not designed as a public health approach, the two are compatible when partnerinvolvement is prioritised and problem solving techniques are geared towards prevention within abroader public health framework.The World Health Organisation Violence Prevention Alliance’s four step public health model forviolence prevention is highly consistent with POP: both share a commitment to understandingproblems; their causes; and the impact of interventions designed to tackle them (WHO 2019). TheWHO model – which can be applied to problems other than violence – places stronger emphasis onscaling up interventions shown to have a positive impact.Figure 4: WHO public health approach to violence1. SurveillanceWhat is the problem?2. Identify riskand protectivefactorsWhat are thecauses?Define the violenceproblem throughsystematic datacollectionConduct research to findout why violence occursand who it affects4. Implementation3. Develop andevaluate interventionsScaling up effectivepolicy & programmesScale-up effective andpromising interventionsand evaluate theirimpact and costeffectiveness.What works andfor whomDesign, implement andevaluate interventionsto see what worksSource: WHO 201915
Table 1: Examples of preventative approaches1PrimaryPreventionPreventing aproblem fromoccurring in thefirst place arly years family-basedEintervention Early years school-basedinterventions Training in social andemotional skills, problemsolving and angermanagement for at-riskchildren Alcohol pricing Firearms laws Neighbourhood watchSecondaryPreventionInterveningearly when aproblem startsto emergeto preventit
police, public health and voluntary sector professionals based on the existing evidence base and their expertise and experiences. It is part of a programme of work to implement the national Policing, Health and Social Care Consensus. Public health approaches, whilst different from traditional models of response policing