Transcription
CUA GUIDELINECanadian Urological Association recommendations on prostatecancer screening and early diagnosisRicardo A. Rendon, MD1; Ross J. Mason, MD2; Karim Marzouk, MD3; Antonio Finelli, MD4; Fred Saad, MD5;Alan So, MD6; Philippe D. Violette, MD7,8; Rodney H. Breau, MD9Department of Urology, Dalhousie University, Halifax, NS, Canada; 2Department of Urology, Mayo Clinic, Rochester, MN, United States; 3Division of Urology, Memorial Sloan Kettering Cancer Centre,New York, NY, United States; 4Division of Urology, University of Toronto, Toronto, ON, Canada; 5Department of Surgery (Urology), University of Montreal, Montreal, QC, Canada; 6Department of UrologicSciences, University of British Columbia, Vancouver, BC, Canada; 7Department of Surgery, Western University, London, ON, Canada; 8Departments of Surgery and Health Research Methods, Evidence, andImpact, McMaster University, Hamilton, ON, Canada; 9Division of Urology, University of Ottawa, Ottawa, ON, Canada1Cite as: Can Urol Assoc J 2017;11(10):298-309. http://dx.doi.org/10.5489/cuaj.4888See related editorial on page 295IntroductionProstate cancer remains the most commonly diagnosed noncutaneous malignancy among Canadian men and is the thirdleading cause of cancer-related death. In 2016, an estimated21 600 men were diagnosed with prostate cancer and 4000men died from the disease;1 however, prostate cancer is aheterogeneous disease with a clinical course ranging fromindolent to life-threatening.Identifying and treating men with clinically significantprostate cancer while avoiding the over-diagnosis and overtreatment of indolent disease remains a significant challenge.Several professional associations have developed guidelineson prostate cancer screening and early diagnosis, but thereare conflicting recommendations on how best to approachthese issues. With recent updates from several large, randomized, prospective trials, as well as the emergence ofseveral new diagnostic tests, the Canadian UrologicalAssociation (CUA) has developed these evidence-basedrecommendations to guide clinicians on prostate cancerscreening and early diagnosis for Canadian men. The aimof these recommendations is to provide guidance on thecurrent best prostate cancer screening and early diagnosispractices and to provide information on new and emergingdiagnostic modalities.Evidence synthesis and recommendations developmentIn order to develop these recommendations, the followingquestions related to prostate cancer screening and diagnosis were defined, a priori, to guide the specific literaturesearches and evidence synthesis:2981. Should Canadian men undergo prostate cancerscreening?2. At what age should prostate cancer screening begin?3. When can prostate cancer screening be stopped?4. How frequently should prostate cancer screening beperformed?5. What diagnostic tests, in addition to prostate-specificantigen (PSA), are available for the early diagnosis ofprostate cancer?The aim of answering the first four questions is to provideguidance on prostate cancer screening in general. The aimof the fifth question is to provide information on additionalavailable tests. Therefore, a different search strategy wasused for these questions. For the first four questions, weemployed a two-step approach in order to synthesize thebest available evidence to develop these recommendations.First, recognizing that several other professional organizations have developed evidence-based guidelines on prostatecancer screening and diagnosis, a complete bibliographicreview of existing guidelines on prostate cancer screeningand diagnosis was performed. Studies related to questions1‒4 were reviewed at full length. Second, in order to identifystudies not captured by existing guidelines, a search of theliterature was conducted using MEDLINE to identify articlesrelated to the screening and diagnosis of prostate cancerthat were published between January 1, 2016 and February2, 2017. To identify articles not yet indexed, a search wasalso performed using PubMed without MEDLINE filters (seeAppendix 1 for search strategy). For the fifth question related to additional diagnostic tests beyond PSA, which canpotentially aid in the early detection of prostate cancer, asystematic search was performed in a similar fashion with nodate restriction for tests not covered by existing guidelines.Case series, case reports, non-systematic reviews, editorials, and letters to the editor were excluded and thesearch strategy was restricted to English language articles.Trained methodologists implemented the specific searchCUAJ October 2017 Volume 11, Issue 10 2017 Canadian Urological Association
Guideline: PSA screening and early diagnosisstrategy and two authors reviewed the titles and abstractsof potential studies to identify their relevance for full-textreview. Levels of evidence and grades of recommendationare provided according to the International Consultation onUrologic Diseases modification of the 2009 Oxford Centrefor Evidence-Based Medicine grading system.2PSA screening1. The CUA suggests offering PSA screening to men witha life expectancy greater than 10 years. The decisionof whether or not to pursue PSA screening should bebased on shared decision-making after the potentialbenefits and harms associated with screening havebeen discussed (Level of evidence: 1; Grade of recommendation: B).Justification: Prostate cancer screening is one of the mostcontroversial issues in urology and preventative medicine.With varying recommendations on PSA screening, no consensus is established among several professional and government organizations (Supplementary Table 1). Many professional associations, including the American UrologicalAssociation,3 National Comprehensive Cancer Network,4European Association of Urology,5 and the American Collegeof Physicians6 recommend offering PSA screening to interested men after a thorough discussion of the benefits andharms. In addition, the United States Preventative ServicesTask Force (USPSTF) recently recommended a similar shareddecision-making approach in men aged 55–69 (currently indraft form at the time of this publication) after previouslyrecommending against screening.7 Conversely, the CanadianTask Force on Preventative Health Care (CTFPHC) weaklyrecommends against PSA screening in men of any age;8however, several important updates of large, populationbased studies have been released since the time of this taskforce publication and herein we include a summary of theevidence for and against screening for prostate cancer.There have been six randomized, controlled trials investigating the role of PSA screening in adult men;9-14 however,three of these studies are at significant risk of bias and aregenerally not considered when weighing the evidence foror against prostate cancer screening. Thus, three randomized, controlled trials, all with recent updates, constitutethe credible Level 1 evidence concerning prostate cancerscreening; the Prostate, Lung, Colon, and Ovarian screeningtrial (PLCO),9 the European Randomized Study of Screeningfor Prostate Cancer (ERSPC),10 and the Goteborg randomizedtrial of PSA screening (Table 1).11The PCLO was a North American trial including 76 683men aged 55‒74 accrued from 10 centres where subjectswere randomized to organized screening or standard care.9In the recently published update, with 15 years of followup,there continues to be no difference in prostate cancer-specif-Table 1. Most recent results from three randomized,controlled trials investigating PSA screeningPLCO(2017 update)15nAge76 68355–74Site10 US centresPSA annually xIntervention 6 years AnnualDRE x 4 yearsCurrentmedianfollowup15 yearsERSPC(2014 update)16162 24355–698 EuropeancountriesPSA q4 years(in mostcentres)Some centresoffered DREGoteborg(2014 update)1720 00050–641 city (Goteborg,Sweden)13 years18 yearsPSA q2 yearsDefinitionof positivetestPSA 4 ng/mlAbnormal DREPSA 3 ng/ml(most centres)PSA 2.5 ng/ml(from 2005 on)PSA 2.9 ng/ml(from 1999–2004)PSA 3.4 ng/ml(from 1995–98)ProstatecancerdeathsControl: 244Screened: 255Control: 545Screened: 355Control: 122Screened: 790.79 (0.69–0.91)0.58 (0.46–0.72)21% relativerisk reductionin favour ofscreening1:7811:2742% relativerisk reductionin favour ofscreening1:1391:13Rate ratiofor CSS(95% CI)NNSNND1.04 (0.87–1.24)N/AN/ACSS: Prostate cancer-specific survival; DRE: digital rectal exam; ERSPC: EuropeanRandomized Study of Screening for Prostate Cancer; NNS: number needed to screen; NND:number needed to diagnose; PLCO: Prostate, Lung, Colon, and Ovarian screening trial; PSA:prostate-specific antigen.ic mortality between patients in the intervention (screening)and control arms;15 however, several important limitationsmay mitigate this finding. Foremost, there was considerable contamination between study arms, with over 80% ofsubjects in the control arm having at least one PSA measurement during the study period. This high contamination ratebiases the result toward finding no difference in mortalityfrom prostate cancer.The ERSPC study is a collection of randomized trialsconducted across eight European countries and includes162 243 men aged 55‒69. While there were some differences between the individual trials, men were randomizedto organized PSA screening or standard care. 10 With 13years of followup, there was a 21% relative risk reduction in prostate cancer mortality.16 In terms of absoluterisk reduction, this equates to 1.28 less prostate cancerdeaths for every 1000 men screened or 781 men undergoing screening and 27 men undergoing treatment to preventone prostate cancer death. In the Swedish Goteborg studyof 20 000 patients aged 50‒64 at enrollment, a similarCUAJ October 2017 Volume 11, Issue 10299
Rendon et alreduction in prostate cancer mortality was seen at up to18 years of followup, with a relative risk reduction of 42%and 139 patients being invited for screening to prevent oneprostate cancer death.17 Although there was also contamination of the control arms in both the ERSPC and Goteborgtrials, the estimated proportion of control patients receivingPSA testing is significantly lower than those in the PLCOtrial.11,18,19 Overall, based on currently available evidencefrom randomized, controlled trials, it appears as thoughorganized PSA screening results in a reduction in prostate cancer mortality. To add to these currently availablestudies, the initial results from the cluster randomized trialof PSA testing for prostate cancer (CAP trial), a large randomized trial including over 400 000 patients in the U.K.randomized to PSA screening or standard care, will likelyprovide further information on the effects of PSA screeningin the near future.20There is also weaker evidence from epidemiological studies on the effect of PSA screening. Prostate cancer mortality has declined since the introduction of PSA screening inNorth America.21-23 While we cannot know with certaintywhy mortality has declined, modelling studies indicate thatthe most plausible and largest contribution to mortalityreduction is from screening.23-27 Additionally, there has beena decrease in the incidence of prostate cancer diagnosis inrecent years in the U.S., which is likely a result of decreasedscreening use.28-30 This has been associated with a stagemigration towards higher stage and more frequent metastatic disease.30,31 While more time is required to determinewhether this recent stage migration will result in an increasein prostate cancer mortality, we believe that reducing themorbidity of advanced and metastatic prostate cancer is initself an important outcome. Although these observationswere not directly used by the guideline panel when considering recommendation for PSA screening, the underlying riskof under-diagnosis of high-risk disease remains a concern.Although the available evidence suggests there are benefits to prostate cancer screening in terms of reduction inmortality, there are also significant potentials harms of overdiagnosis and over-treatment. Indeed, up to 67% of mendiagnosed with prostate cancer by screening will be identified as having clinically insignificant prostate cancer, which,if never detected, would be unlikely to lead to increasedmorbidity or mortality.32-36 Thus, if screened, men with insignificant disease may be unnecessarily exposed to the potential harms of both prostate biopsy and treatment in additionto the psychological effects accompanying a prostate cancerdiagnosis. The increased use of active surveillance for lowrisk prostate cancer in Canada has been an important stepin reducing the over-treatment of prostate cancer; however,active surveillance does not eliminate the issue of overdiagnosis and itself is associated with significant potentialdetriments to quality of life.37 With these risks in mind, it is300imperative that we not only separate the diagnosis of prostatecancer from the treatment of prostate cancer, but that weinstitute improved screening and early detection practices todecrease the risk of detecting clinically insignificant disease.The CUA recognizes that PSA screening may not be thebest option for all men. Balancing the known benefits andrisks of PSA screening is difficult and is significantly influenced by personal values. As such, the decision of whetheror not to undergo prostate cancer screening is, and will likelyremain, an individualized decision. In order to reach thisdecision, the CUA recommends that healthcare providersengage in a thorough discussion on the potential risks andbenefits of PSA screening with their patients and that shareddecision-making be performed.Best screening practicesWhen prostate cancer screening is performed, the overarching goal should be the early detection of clinically significantprostate cancer in healthy men while minimizing the detection and treatment of low-risk disease. Screening studiesare challenging to conduct because of the large numbersof participants required, risk of contamination, loss to followup, and many other pitfalls. It is not feasible to evaluate most questions regarding timing and administration ofPSA directly. In this context, the CUA provides the following recommendations based upon the inclusion criteria ofrandomized trials and high-quality observational studies toencourage “smart” screening. Our aims are to maintain benefits and mitigate potential harms associated with screening.2. For men electing to undergo PSA screening, we suggest starting PSA testing at age 50 in most men andat age 45 in men at an increased risk of prostatecancer (Level of evidence: 3; Grade of recommendation: C).Justification: Although the optimal age for starting PSAscreening has not been vigorously studied, our recommendation for starting PSA screening at age 50 comes from theGoteborg trial, which provides randomized data on thebenefits of screening in men starting at this age;11 however,evidence from observational studies suggests that certainmen may benefit from PSA screening at an earlier age, witha nearly 5% risk of developing lethal prostate cancer within15 years for men aged 45‒49 with a PSA 4 ng/ml.38,39Although it remains unclear which men will benefit fromearly PSA screening, family history imparts a substantiallyincreased risk of prostate cancer diagnosis at a younger age.Particularly, men aged 50 with a family history of prostatecancer in a first- or second-degree relative have an approximately five-fold and two-fold increased risk of receiving aprostate cancer diagnosis, respectively.38The potential benefits and harms of PSA screening formen less than age 45 has not been prospectively studied;CUAJ October 2017 Volume 11, Issue 10
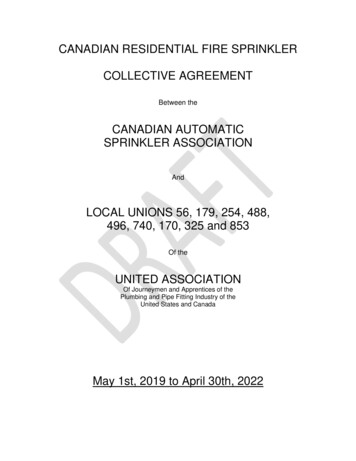
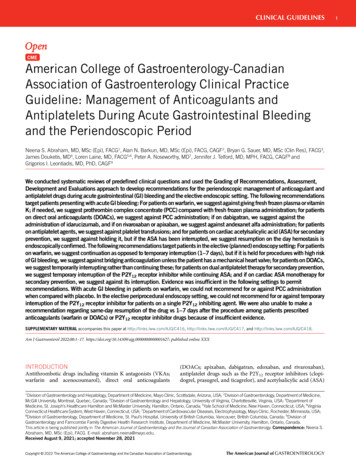
Guideline: PSA screening and early diagnosishowever, a recently published case-control study nestedwithin the Physicians Health Study cohort identified thatthe risk of developing metastatic prostate cancer within 15years among men in this age group was very low, evenamong men with PSA levels in the top decile.38 Thus, PSAtesting in these men may lead to biopsies and diagnosesthat are unlikely to provide benefit. The potential delay indiagnosis in the small proportion of men at this age withclinically significant prostate cancer seems unlikely to leadto a missed opportunity for curative treatment.These recommendations are not directed towards menwith known germ-line mutations associated with prostatecancer development (e.g., BRCA1, BRCA2, HOXB13). Inthese cases, an individualized testing strategy after consultation with a clinical geneticist is most appropriate.3. For men electing to undergo PSA screening, we suggest that the intervals between testing should beindividualized based on previous PSA levels (Fig. 1).a. For men with PSA 1 ng/ml, repeat PSA testing every four years (Level of evidence: 3;Grade of recommendation: C).b. For men with PSA 1–3 ng/ml, repeat PSA testing every two years (Level of evidence: 3;Grade of recommendation: C).c. For men with PSA 3 ng/ml, consider morefrequent PSA testing intervals or adjunctivetesting strategies (Level of evidence: 4; Gradeof recommendation: C).Justification: Although the frequency at which PSA screening should be performed has not been rigorously studiedto date, we can extrapolate from the existing clinical trialsand observational studies to provide some guidance on thisissue. In particular, men in the screening arms of the ERSPCtrial and Goteborg trial underwent testing at intervals offour and two years, respectively, providing the basis for ourrecommendations.For men with a PSA level 1ng/ml, longer intervals betweenPSA testing are appropriate. Indeed, a large prospective cohortRepeat testingevery 4 yearsa,bPSA 1Prostate cancerscreening shareddecision-making(ages 50–70)Repeat testingevery 2 yearsaPSA 1–3PSA 3study including men undergoing annual PSA screening identified that men with a PSA 1 ng/ml had a 10-year prostatecancer detection rate of only 3.4%, of which 90% were considered low-risk.40 Furthermore, the nested case-control studyreferenced above identified that the risk of developing metastatic disease within 15 years for a man of any age with PSA 1 ng/ml is very low.39 As such, allowing a longer intervalbetween PSA testing for these men is unlikely to result in anincrease in prostate cancer morbidity or mortality and willpotentially reduce the risk of over-detection as a result of leadtime bias or natural fluctuations in PSA levels.On the other hand, as baseline PSA levels rise above 1ng/ml, the intermediate-term risk of developing both anyprostate cancer and clinically significant prostate cancerincreases substantially.39-41 As such, we recommend thatthese men, if electing PSA screening, should undergo testing every two years. The ERSPC trial considered a positivetest to be a PSA level of 3 ng/ml, while the Goteborg trialconsidered a positive test to be between 2.5 and 3.4 ng/ml(depending on the year of study). Thus, the optimal frequency of PSA testing in men above these levels is unknown. Formen with PSA 3 ng/ml, more frequent PSA testing intervalscan be considered. In addition, adjunctive testing strategiesthat estimate the risk of clinically significant disease may behelpful for biopsy decision-making in these men (see below).4. For men electing to undergo PSA screening, we suggest that the age at which to discontinue PSA screening should be based on current PSA level and lifeexpectancy.a. For men aged 60 with a PSA 1 ng/ml, consider discontinuing PSA screening (Level ofevidence: 2; Grade of recommendation: C).b. For all other men, discontinue PSA screeningat age 70 (Level of evidence: 2; Grade of recommendation: C).c. For men with a life expectancy less than 10years, discontinue PSA screening (Level of evidence: 4; Grade of recommendation: C).More frequentPSA testingcPSA elevatedConsider adjunctivestrategiesdAbnormalBiopsy shareddecision-makingFig. 1. Prostate cancer screening pathway. aDiscontinue screening if life expectancy 10 years; bconsider discontinuation of screening if age 60 and PSA 1 ng/ml;cmore frequent testing interval can be considered; the optimal frequency is unknown; di.e., risk calculators, % free PSA, etc. PSA: prostate-specific antigen.CUAJ October 2017 Volume 11, Issue 10301
Rendon et alJustification: For men at age 60 with a PSA level 1 ng/ml,the risk of developing or dying from metastatic prostate cancer is low.39,42,43 In a large, population-based study comparing two cohorts of men (one screened and one unscreened),the 15-year cumulative incidence of metastatic prostate cancer was low in both cohorts among men with a PSA 1ng/mlat age 60 (0.4% and 0%, respectively).42 In addition, a casecontrol study nested within the unscreened cohort foundthat the risk of being diagnosed with metastatic prostatecancer by age 85 was 0.5% for men with a PSA 1 ng/ml atage 60.43 In contrast, for men at this age with a PSA above1 ng/ml, the risk of developing potentially lethal prostatecancer increases substantially according to PSA level andthus screening can reasonably be continued.Men at age 70 have the highest incidence of prostatecancer over-diagnosis and several studies have suggestedthat screening in this age group is likely not beneficial.16,27,44Indeed, a large population-based study identified that therisk of prostate cancer over-diagnosis increases substantially with age and is highest in men greater than age 70.Additionally, the ERSPC trial identified that starting screeningat age 70 did not result in a reduction in prostate cancermortality.16 Furthermore, a well-performed modelling studyusing data from the ERSPC found that any potential benefitto screening in men over 70 was offset by the detrimentsto quality of life.27 Thus, we recommend that PSA testing inasymptomatic men be discontinued at age 70; however, forinterested men in excellent health at age 70, PSA testing canbe considered, recognizing the lack of empirical data in thisage group. As such, for these men, continued PSA testingis a matter of clinical judgment and personal preferences.For men with a high risk of mortality from competingcauses, PSA testing is unlikely to provide benefit.45 The CUArecognizes that estimating life expectancy is challenging.46Nonetheless, it is recommended that physicians take intoaccount a patient’s general health status and competing risksof mortality when considering whether or not to offer PSAtesting. If life expectancy is limited by other serious illnessesor comorbidities, PSA screening should not be initiated orcan be discontinued.Adjunctive strategies for improving prostate cancerearly diagnosisThe past two decades have seen the development or evaluation of several potential adjunctive measures that mayincrease the benefits or reduce the harms associated withscreening in addition to PSA. Specifically, PSA kinetics, PSAdensity, percent free PSA, biomarker panels, and prostaterisk calculators may help select patients at higher or lowerrisk of significant cancer. The refinement of prostate multiparametric magnetic resonance imaging (mpMRI) may also302benefit selected individuals. Below we provide a summaryof the most commonly used modalities currently available.mpMRIRecently, Cancer Care Ontario (CCO) published recommendations on the use of mpMRI in the initial diagnosis ofprostate cancer based on a systematic review of the literature.47 The CUA endorses these guidelines and their recommendations are summarized below.5a. In patients with an elevated risk of clinically significant prostate cancer (according to PSA levels and/or nomograms) who are biopsy-naive, mpMRI followed by targeted biopsy (biopsy directed at cancersuspicious foci detected with mpMRI) should not beconsidered the standard of care.Qualifying statement: The CCO guidelines panel identifiedthat there is limited evidence on the utility of mpMRI in thebiopsy-naive setting and that the studies that do exist areof poor- to moderate-quality. In addition, they found thatthe currently available studies indicate that that the diagnostic characteristics of mpMRI in this setting are poor tomoderate (particular with regards to specificity and positivepredictive value).Since the publication of the CCO guidelines, an additional large, multicentre, prospective cohort study has beenpublished evaluating the diagnostic utility of mpMRI in menat risk for prostate cancer.48 The PROMIS study comparedthe accuracy of mpMRI with transrectal ultrasound (TRUS)biopsy to determine the utility of mpMRI as a triage test todecide which men with an elevated PSA may be able toavoid biopsy. In total, 576 men with a clinical suspicion ofprostate cancer (PSA 15 ng/ml) underwent mpMRI followedby TRUS and template prostate mapping biopsy. Overall,mpMRI displayed a moderate sensitivity and negative predictive value for predicting Gleason 3 4 disease (88% and76%, respectively), but the specificity and positive predictive value were poor (45% and 65%, respectively). Overall,we believe that the results of this study do not modify theconclusions of the CCO, and the CUA guidelines committeeagrees with the recommendation that mpMRI should not beroutinely used in the biopsy-naive setting.5b. In men who had a prior negative TRUS-guidedsystematic biopsy who demonstrate an increasingrisk of having clinically significant prostate cancersince prior biopsy (e.g., continued rise in PSA and/or change in findings from digital rectal examination[DRE]), mpMRI followed by targeted biopsy maybe considered to help in detecting more clinicallysignificant prostate cancer patients compared withrepeated TRUS-guided systematic biopsy.Qualifying statement: The CCO guidelines panel identifiedthat patients with a prior negative TRUS-guided systematicCUAJ October 2017 Volume 11, Issue 10
Guideline: PSA screening and early diagnosisbiopsy who demonstrate increasing risk of clinically significant prostate cancer may benefit from undergoing mpMRIprior to repeat biopsy. Although the quality of evidenceagain ranged from poor to moderate, a persistent trendemerged showing that mpMRI followed by targeted biopsydetects a higher number of clinically significant prostatecancers relative to repeat systematic TRUS biopsy alone.Thus, we agree with the CCO that mpMRI can be consideredprior to undergoing repeat prostate biopsy; however, theCUA acknowledges that there may be practical limitationsto this approach, such as timely access to MRI and variationsin quality and interpretation.PSA kineticsAnnual PSA velocity (PSAV) or PSA doubling time (PSADT)can be established from serial measurements of PSA overtime. Historical reports have identified that a PSAV greaterthan 0.75ng/ml/year may indicate an increased risk of prostate cancer.49 Additionally, data from longitudinal studieshave illustrated that PSAV greater than 0.35ng/ml/year (whentotal PSA is 4.0 ng/ml) is associated with a higher relativerisk of prostate cancer death,50 suggesting that PSAV can beused as potential prognostic marker for aggressive disease;however, other studies, including a large systematic reviewof 64 articles, identified that there is conflicting evidenceon the incremental value of PSAV over absolute PSA levelalone.51-53 It is clear that a sustained and substantial rise inPSA over time is a concerning finding and warrants investigation. Furthermore, a stable or declining PSA is reassuringin men with PSA levels that slightly exceed PSA thresholds.The CUA does not recommend using PSAV alone for clinical decision-making in men undergoing routine screening;however, PSAV can provide additional information abouta patient’s risk of prostate cancer.PSA densityPSA density (PSAD) is the serum PSA divided by prostatevolume. A PSAD threshold of 0.15 ng/ml/cm3 has been suggested to distinguish men at risk from prostate cancer, andstudies have also linked higher PSAD with adverse pathological features at the time of prostatectomy;54,55 however,others have failed to validate these findings.56,57 Substantialinter-observer variability from the estimation of prostate volume on ultrasound also raises further questions regarding thereliability of PSAD.58,59 Due to the lack of empirical validation, the use of PSAD alone for clinical decision-makingis discouraged; however, use of PSAD can be consideredadjunctively in men with known prostate volumes.Percent free PSAThe measurement of percent free PSA has been studied as arisk-stratifying tool aimed at distinguishing men at risk fromprostate cancer vs. those with elevations in PSA from benigncauses. Several studies have illustrated the potential utilityof percent free PSA for identifying men with disease.60-64 Ina large, multicentre, prospective study, prostate cancer (allgrades) was detected in 56% of men with a free-to-totalPSA ratio of less than 0.10 (for men with a PSA between 4and 10 ng/ml), whereas cancer was detected in 8% of menwith a ratio greater than 0.25.65 In a recent publication, atotal of 6982 percent free and total PSA measurements wereobtained over a 12-year time span from a single institution.Percent free PSA used as a reflex marker demonstrated highlevels of performance, with the capability of sparing 66% ofunnecessary prostate biopsies.66 Additionally, it was identified that similar to PSA, percent free PSA can also fluctuate,therefore stressing the need for repeat confirmatory testingprior to clinical decision-making. The use of percent freePSA alone for clinical decision-making is not recommended; however, percent free PSA can be useful in estimatingthe risk of underlying disease in men with elevations inPSA (Level of evidence: 2; Grade of recommendation : C).Biomarkers1. Four-kallikrein panel (4Kscore )The four-kallikrein panel, or 4Kscore is a commerciallyavailable test combining total PSA, free PSA, intact PSA, andhuman kallikrein 2 with age, DRE results, and prior biopsystatus in order to generate a risk estimate of harbouringGleason 7 disease. Originally developed using data fromthe ERSPC and the Prostate Testing for Cancer and Treatment(ProtecT) studies,6
Canadian Urological Association recommendations on prostate cancer screening and early diagnosis. CUAJ October 2017 Volume 11, Issue 10 299 Guideline: PSA screening and early diagnosis strategy and two authors reviewed the titles and abstracts of potential studies to identify their relevance for full-text