Transcription
POSITION PAPER ON ADOLESCENT DRUG POLICYAdolescent Substance Abuse:A Public Health PriorityAn evidence-based, comprehensive,and integrative approach
Physician Leadership on National Drug PolicyPLNDP National Project OfficeCenter for Alcohol and Addiction StudiesBrown UniversityBox G-BH Providence, RI 02912phone 401-444-1817fax401-444-1850email plndp@brown.eduwww.PLNDP.org August 2002All Rights ReservedPLNDP National Office Project StaffDavid C. Lewis, MD, Project DirectorKathryn L. Cates-Wessel, Associate DirectorMaureen Mooney, Administrative CoordinatorLaura Sporcic, Research AssistantKirsten Spalding, Student Research AssistantAngela Feraco, Student Research Assistant
Adolescent Substance Abuse:A Public Health PriorityAn evidence-based, comprehensive,and integrative approach
TABLE OF CONTENTSPAGE NO.i111233141495563PLNDP: LEADERSHIP & HISTORY1. INTRODUCTION OF THE PROBLEM2. CONTINUUM OF CARE: PREVENTION3. CONTINUUM OF CARE: SCREENING, ASSESSMENT, REFERRAL, AND TRAINING4. CONTINUUM OF CARE: TREATMENT5. FINANCING OF CARE6. THE CO-OCCURRENCE OF MENTAL AND SUBSTANCE USE DISORDERS7. THE INTERFACE OF YOUTH WITH JUVENILE JUSTICE8. APPENDICES, REFERENCES, CHART LIST
ACKNOWLEDGEMENTSThe individuals whose work, presented at the November 29, 2001 meeting, providesthe basis from which the report is writtenSuzanne Colby, PhDResearch Faculty Coordinator –November MeetingAssistant ProfessorCenter for Alcohol and AddictionStudies, Brown UniversityHoover Adger Jr., MD, MPhPediatricianJohns Hopkins HospitalJean Callahan, JD, MSWProject DirectorAdolescent Portable Therapy,Vera Institute of JusticeMichael French, PhDAssociate ProfessorDepartment of Epidemiology and PublicHealth, University of MiamiHarvey Skinner, PhDChairDepartment of Public Health Sciences,University of TorontoJ. David Hawkins, PhDDirectorSocial Development Research Group,University of WashingtonEric Wagner, PhDAssociate ProfessorCollege of Urban and Public Affairs,Florida International UniversityPeter Monti, PhDDirectorCenter for Alcohol and AddictionStudies, Brown UniversityKen Winters, PhDSenior Research AssociateDepartment of Psychiatry,University of MinnesotaLaura Burney Nissen, PhDCo-DirectorReclaiming FuturesMichael Dennis, PhDSenior Research PsychologistChestnut Health SystemsThe individuals who graciously reviewed sections of themany versions of this report; their work and commentsare greatly appreciatedThe organizations whosematerial we relied heavilyon in the preparation ofthis reportAmerican Academy of PediatricsAmerican Bar AssociationDoreen Cavanaugh, PhDSenior Research AssociateSchneider Institute for Health Policy,The Heller School, Brandeis UniversityBob DowningConvenorNational Coalition to Increase Accessand Parity for Addiction TreatmentCenter for Substance Abuse TreatmentSuzanne Colby, PhDAssistant ProfessorCenter for Alcohol and AddictionStudies, Brown UniversityShelly GehshanProgram DirectorNational Conference of State LegislaturesNational Institute on Drug AbuseMichael Dennis, PhDSenior Research PsychologistChestnut Health SystemsGary De Carolis, MEdPublic Health AdvisorPerformance Partnership Grant ProgramBranch, Center for Substance AbuseTreatmentJoan Dilonardo, PhDSocial Science AnalystOffice of Quality Improvementand Financing, Center for SubstanceAbuse TreatmentRandolph Muck, MEdTeam Leader/Public Health AdvisorCenter for Substance Abuse TreatmentHerman Diesenhaus, PhDPublic Health AnalystOffice of Evaluation, Scientific Analysisand Synthesis, Center for SubstanceAbuse TreatmentNational Institute on Alcohol Abuseand AlcoholismNational Mental Health AssociationOffice of Juvenile Justice andDelinquency Prevention
An Evidence-Based, Comprehensive and IntegrativeApproach to Adolescent Substance AbuseSubstance abuse is a major national public health problem that creates impairedhealth, harmful behaviors, and major economic and social burdens.but there areeffective medical and public health approaches to the problem.JUNE E. OSBORN, MD, CHAIRSixth President of the Josiah Macy, Jr. Foundation. Former Chair of the U.S.National Commission on AIDS. Former Dean, University of Michigan, School ofPublic Health. Professor Emerita, Pediatrics and Communicable Disease, andEpidemiology, University of Michigan.GEORGE D. LUNDBERG, MD, VICE CHAIREditor-in-Chief Emeritus, Medscape. Special Healthcare Advisor to CEO andChair, WEBMD. Former Editor, Journal of American Medical Association.Adjunct Professor of Health Policy, Harvard. Former Professor and Chair ofPathology at the University of California-Davis. Former President of theAmerican Society of Clinical Pathologists.ERROL R. ALDEN, MDDeputy Executive Director of the American Academy of Pediatrics.JEREMIAH A. BARONDESS, MDPresident of the New York Academy of Medicine and Professor Emeritus ofClinical Medicine at the Cornell University Medical College.LONNIE R. BRISTOW, MD, MACPMember, Board of Regents of the Uniformed Services University of HealthSciences and Former President of American Medical Association.CHRISTINE CASSEL, MDDean, School of Medicine, Oregon Health & Science University. FormerChair of the American Board of Internal Medicine. Former President of theAmerican College of Physicians.LINDA HAWES CLEVER, MDChief of Occupational Health at California Pacific Medical Center, SanFrancisco. President, Renew! Former Editor, Western Journal of Medicine.GEORGE D. COMERCI, MDClinical Professor of Pediatrics, University of Arizona College of Medicine.Former President of the American Academy of Pediatrics and the AmbulatoryPediatric Association.FLOYD E. BLOOM, MDChair and Professor, Department of Neuropharmacology, The Scripps ResearchInstitute, La Jolla, California. Former Editor, Science.RICHARD F. CORLIN, MDPresident, American Medical Association. Former Speaker of the AmericanMedical Association House of Delegates. Assistant Clinical Professor at theUniversity of California - Los Angeles, School of Medicine. Former President ofthe California Medical Association.THOMAS F. BOAT, MDChair, Department of Pediatrics at the University of Cincinnati College ofMedicine. Director of the Children’s Hospital Research Foundation. FormerChair, American Board of Pediatrics.JAMES E. DALEN, MDVice-President for Health Sciences and Dean, College of Medicine at theArizona Health Sciences Center. Editor, Archives of Internal Medicine. FormerPresident, American College of Chest Physicians.EDWARD N. BRANDT, JR., MD, PhDDirector of the Center for Health Policy. Regents Professor of Internal Medicineand of Health Administration and Policy at the University of Oklahoma HealthSciences Center. Former Assistant Secretary for Health in the U.S. Dept. ofHealth and Human Services (Reagan Administration).CATHERINE D. DEANGELIS, MD, MPhEditor, Journal of American Medical Association.PLNDP Leadership and History i
SPENCER FOREMAN, MDPresident of Montefiore Medical Center and Former Chair of the Association ofAmerican Medical Colleges (AAMC).WILLARD GAYLIN, MDClinical Professor of Psychiatry at Columbia College of Physicians and Surgeons.Co-founder of the Hastings Center. Former President and Chair of the HastingsCenter and currently a member of the Board of Directors.H. JACK GEIGER, MDArthur C. Logan Professor Emeritus and former Chair, Department of CommunityHealth and Social Medicine, City University of New York Medical School.Founding member and Former President of Physicians for Human Rights andPhysicians for Social Responsibility. Former Chair, Departments of CommunityMedicine, SUNY-Stonybrook and Tufts Medical School.ALFRED GELLHORN, MDDirector, Aaron Diamond Foundation Post Doctoral Research Fellowships inAIDS and Drug Abuse. Former Director of Medical Affairs, NY State Departmentof Health. Founding Director Sophie Davis School of Biomedical Education, VicePresident Health Affairs-City College of New York.DAVID S. GREER, MDDean and Professor Emeritus of the Brown University School of Medicine andFounding Director of International Physicians for the Prevention of Nuclear War.HOWARD H. HIATT, MDProfessor of Medicine at Harvard Medical School. Senior Physician at theBrigham and Women’s Hospital. Founder and Former Director of Initiatives forChildren Program of the American Academy of Arts and Sciences. Former Deanof the Harvard School of Public Health.JEROME P. KASSIRER, MDFormer Editor, New England Journal of Medicine. Professor and Former ViceChair, Department of Medicine at Tufts University School of Medicine. FormerChair, American Board of Internal Medicine. Distinguished Professor, TuftsUniversity School of Medicine. Professor (Adjunct) of Medicine, Yale UniversitySchool of Medicine.DAVID A. KESSLER, MDDean, Yale Medical School. Former Commissioner, Food and Drug Administration(Bush and Clinton Administrations).PHILIP R. LEE, MDSenior Advisor, Institute for Health Policy Studies and Professor of SocialMedicine (Emeritus), School of Medicine, University of California-San Francisco(UCSF). Consulting Professor, Program in Human Biology, Stanford University.Former Assistant Secretary for Health, U.S. Dept. of Health and Human Services(Clinton Administration). Former Director and Founder of the Institute for HealthPolicy Studies at UCSF. Former Chancellor, UCSF.JOSEPH B. MARTIN, MD, PhDDean, Harvard Medical School. Former Chancellor, University of California San Francisco.ANTONIA COELLO NOVELLO, MD, MPH, DrPhHealth Commissioner, State of New York. Visiting Professor of HealthPolicy and Management at the Johns Hopkins University School of Hygieneand Public Health. 14th Surgeon General of the U.S. Public Health Service(Bush Administration).CLAUDE H. ORGAN, JR., MDProfessor and Chair of the Department of Surgery, University of California,Davis-East Bay. Editor, Archives of Surgery. Former Director and Chair ofthe American Board of Surgery.ROBERT G. PETERSDORF, MDDistinguished Professor of Medicine and Senior Advisor to the Dean,University of Washington. Formerly Distinguished Physician, Veterans’ HealthAdministration. Former President of the Association of American MedicalColleges, the Association of American Physicians, the Association ofProfessors of Medicine, and the American College of Physicians.P. PRESTON REYNOLDS, MD, PhDAssociate Professor of Medicine, Vice Chair of the Department of Medicine andChief of the Division of General Internal Medicine, Johns Hopkins University.FREDERICK C. ROBBINS, MDFormer Director, Center for Adolescent Health of Case Western ReserveUniversity. Dean Emeritus at Case Western Reserve School of Medicineand University Professor Emeritus. Nobel Laureate in Physiology andMedicine. Former President, Institute of Medicine.ALLAN ROSENFIELD, MDDean of the Mailman School of Public Health, DeLamar Professor of PublicHealth and Professor of Obstetrics and Gynecology at Columbia University.Chair, NY State Department of Health AIDS Advisory Council. Former ActingChair, Department of Obstetrics and Gynecology, Columbia University.STEPHEN C. SCHEIBER, MDExecutive Vice President, American Board of Psychiatry and Neurology. AdjunctProfessor of Psychiatry at Northwestern University Medical School, and theMedical College of Wisconsin.SEYMOUR I. SCHWARTZ, MDDistinguished Alumni Professor and Chair of the Department of Surgery at theUniversity of Rochester School of Medicine and Dentistry. President-elect andChair of the Board of Regents of the American College of Surgeons. Editor,Journal of the American College of Surgeons. Former President, Society forClinical Surgery and the American Surgical Association. Member, AmericanPhilosophical Society.HAROLD SOX, JR., MD, MACPEditor, Annals of Internal Medicine. Formerly Joseph M. Huber Professor ofMedicine and Former Chair of the Department of Medicine, Dartmouth MedicalSchool. President Emeritus of the American College of Physicians-AmericanSociety of Internal Medicine. Chair of the Medicare Coverage AdvisoryCommittee.ROBERT D. SPARKS, MDFormer President and Chief Executive Officer, California MedicalAssociation Foundation. President Emeritus and Senior Consultant for theW.K. Kellogg Foundation.LOUIS W. SULLIVAN, MDPresident, Morehouse School of Medicine. 17th Secretary, U.S. Department ofHealth and Human Services (George H. W. Bush Administration). FoundingPresident, Association of Minority Health Professions Schools.ALLAN TASMAN, MDProfessor and Chair, Department of Psychiatry and Behavioral Sciences at theUniversity of Louisville School of Medicine. Former President, AmericanPsychiatric Association. Former President, American Association of Chairs ofDepartments of Psychiatry. Associate Editor, American Journal of Psychotherapy.DONALD D. TRUNKEY, MDProfessor Emeritus, Department of Surgery, Oregon Health Sciences University.Former Chief and Chairman of Surgery at San Francisco General Hospital.The PLNDP project is supported by generous contributions from individuals and foundations, primarilyThe Robert Wood Johnson Foundation and The John D. and Catherine T. MacArthur Foundation.ii PLNDP Leadership and History
PLNDP LeadershipSince this report is focused on youth, several PLNDP leaders have contributed statements and pictures of themselves with family members or involving activities withyoung people. This approach was taken to emphasize our mission to support the needfor prevention and treatment of our nation’s most cherished resources—our children.PLNDP LEADERS AS PICTURED ABOVE.First Row Seated (left to right)Linda Hawes-Clever, MDGeorge Comerci, MDCatherine DeAngelis, MDKenneth Shine, MD(invited facilitator)David C. Lewis, MD(PLNDP Project Director)June Osborne, MD(PLNDP Chair)Antonia Novello, MDPreston Reynolds, MDJeremiah Barondess, MDSecond Row (left to right)Richard Corlin, MDChristine Cassel, MDThomas Boat, MDRobert Sparks, MDRobert Petersdorf, MDLouis Sullivan, MDDavid Greer, MDGeorge Lundberg, MD(PLNDP Vice Chair)Allan Tasman, MDHal Sox, MDLonnie Bristow, MDThird Row (left to right)Edward Brandt, MDFrederick Robbins, MDJack Geiger, MDAllan Rosenfield, MDErrol Alden, MDAlfred Gellhorn, MDJerome P. Kassirer, MDDonald Trunkey, MDStephen Scheiber, MDSeymour Schwartz, MDHoward Hiatt, MDFloyd Bloom, MDPLNDP Leadership and History iii
PLNDP HistoryPhysician Leadership on National Drug Policy (PLNDP) was started in July1997 when 37 of the nation’s distinguished physicians, representing virtuallyevery medical specialty, met and agreed on a Consensus Statement. This statement,which stresses the need for a medical and public health approach to national drugpolicy, has served as the underlying framework for all of the project’s activities.Because of their wide range of backgrounds, there is no particular ideological orpolitical perspective that dominates the group. The PLNDP perspective is to use evidence-based studies to inform policy making.Since initiating this project: About 6,000 physicians, 23 state medical societies, and theAmerican Medical Association have endorsed the PLNDPConsensus Statement. (See Appendix A for the PLNDPConsensus Statement, and Appendix B for a list of supportingorganizations); 250 medical students have endorsed PLNDP’s ConsensusStatement; the project also has been endorsed by the AmericanMedical Student Association; Several PLNDP Outreach Partners have been established,including:American Academy of Addiction Psychiatry (AAAP)American Academy of Pediatrics (AAP)American College of Obstetrics-Gynecology (ACOG)lic. One video, entitled Drug Addiction: The Promise of Treatment,discusses the effectiveness and cost-effectiveness of treatment;another, Trial, Treatment and Transformation, examines alternatives to incarceration; and the third video, From Hopelessness toHealing, is a blend of the two above mentioned videos and wasprepared for local cable television viewing. A fourth video on adolescent substance abuse, soon to be released, will focus on theissues covered by this report. Developed the following policy reports, all available on PLNDPwebsite (www.PLNDP.org):Best Practices Initiative: State-level Issues for Medicaid/Welfare and Substance Abuse Treatment, May 2002Effective Methadone Treatment of Heroin Addiction in OfficeBased Practices with a Focus on Methadone Maintenance,November 2000American Medical Student Association (AMSAAmerican Society of Addiction Medicine (ASAM)Join TogetherNational Council on Alcoholism andDrug Dependence, Inc. (NCADD)Society of General Internal Medicine (SGIM)Society of Teachers of Family Medicine (STFM)A Physician’s Guide on How to Advocate for More EffectiveNational and State Drug Policies, September 2000 (publishedwith Join Together)Physician Leadership on National Drug Policy Position Paper onDrug Policy, January 2000Over the five-year life of PLNDP we have seen a growingmajority of Americans support increased funding in the area ofPLNDP has also:treatment and prevention (demand reduction) to more effectively address substance use problems. According to a 2000 Developed and distributed more than 6,000 copies of videoreports to physicians, other healthcare professionals, judges,lawyers, professional organizations, policymakers, and the pub-iv PLNDP Leadership and Historypoll conducted by Peter D. Hart Research Associates for DrugStrategies, three out of five adults said that drug abuse is“more of a public health problem better handled by prevention
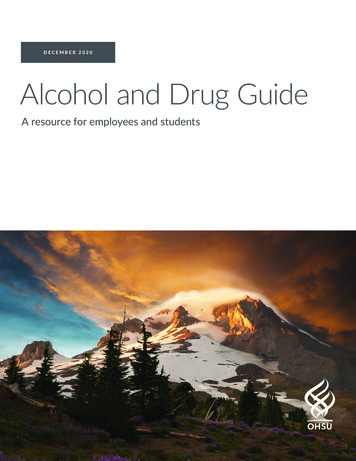
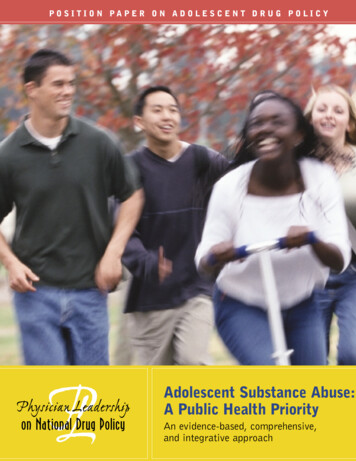
and treatment programs” than by the criminal justice system.1In addition, two surveys from the Harvard School of PublicHealth and the Robert Wood Johnson Foundation give an indication of a shift in public attitudes toward treatment. The first,covering the decade up to 1997,2 found that increased fundingfor treatment was strongly favored by only 19 percent of thosewho responded, whereas another more recent survey (2000)from the same institutions found that 69 percent thought thatillicit drug use can be treated successfully and supportedincreasing funding for treatment.3While Americans’ opinions about how to spend drug controlfunds are shifting toward treatment and preventionapproaches, 80 percent of state and local spending is devotedto enforcement.4 At the federal level, as illustrated in figure 1below, the government also continues to spend considerablymore of the 19.2 billion drug control budget on supplyreduction (67 percent) than on prevention and treatment(33 percent).5 It is the hope of the PLNDP that as public opinion shifts, so will the policy toward prevention and treatment.Lonnie Bristow, MD, PLNDP member“What PLNDP has managed to do is tomarshal the facts—the scientific evidence,Fiscal Year 2003President’s Request, By AreaTotal Resources: 19.2 Billionif you will—that this is the way to go.6%It doesn’t do away with punishment and12%incarceration for those individuals who20%have broken the law. Of course they shouldreceive punishment and incarceration. But13%49%coupled with that should be a broaderperspective which realizes that there is areal illness here which is capable of beingtreated successfully and, if we treat that ill-Domestic Law Enforcement (49%)International (6%)Interdiction (12%)ness, or if we attempt to prevent it, in thePrevention w/Research (13%)Treatmentw/Research (20%)long run society is going to benefit muchmore than they will from building largerand more prisons.”Source: Office of National Drug Control Policy: “Drug Abusein America.” Washington, DC: Executive Office of thePresident, Power Point Presentation. February, 2002. Slide#13. Available www.whitehousedrugpolicy.govfigure 1PLNDP Leadership and History v
INTRODUCTION OF THE PROBLEM1
Adolescent substance abuse is a major national publichealth problem. Research indicates that, despite a recent leveling-off ofsubstance use by adolescents, the current levels remain high. Studies suggest that the younger an individual is at the onset of substance use, thegreater the likelihood that a substance use disorder will develop and continueinto adulthood. In fact, more than 90 percent of adults with current substanceINTRODUCTIONuse disorders started using before age 18; half of those began before age 15.1In the area of prevention, researchers havefactors are discovered and treated early, adoles-established a list of risk and protective factorscent substance use problems and delinquentthat are critical to the development and imple-behavior could be prevented.mentation of effective prevention programs.These risk factors include: the availability ofUnfortunately, many youth are not identified asdrugs in the community, a family history of sub-being involved with substance use until it pro-stance abuse, learning disabilities and othergresses to abuse or dependence. In the 1990s,academic problems, and associating withas rates of frequent use of alcohol, marijuana,friends who engage in problem behaviors,and other drugs escalated, the number of ado-among others. Identifying and addressing theselescents entering the treatment systemfactors early is a critical step in the prevention andincreased by more than 50 percent.5 Despite thisintervention of substance use problems and delin-increase, this figure only represents one in tenquency.2 Today, most youth who enter substanceyouths who needed treatment.5 While it is clearabuse treatment programs do so through thethat treatment benefits this population, adoles-juvenile justice system. One study reports thatcents present a unique challenge to the treat-up to 67 percent of youth involved in the juvenilement community. Compared to adults, adoles-justice system have a substance use problem.3cents have greater problems with marijuana andMany of these youth also have a mental disorder,alcohol, higher rates of binge use, and greaterwhich complicates the administration and efficacycomplications as a result of the developmentalof treatment. One national study found that 73 per-changes they are undergoing.1 Impulsive andcent of youth in correctional facilities reportedrisk-taking behaviors are more pervasive inmental health problems during screening. If riskthis population as well, which complicates4INTRODUCTION OF THE PROBLEM 1
treatment. Treatment for adolescents must betreatment is not always apparent to all health-tailored to these specific needs, as well as gen-care professionals. This lack of knowledge isder and race concerns.primarily due to the fact that physicians are nottrained to recognize these problems in patients,The largest insurer of children and adolescentsas only eight percent of US medical schoolsin this country is Medicaid, covering 16.4 millionoffer a specific required substance abuse com-children under the age of 22.6 Substance abuseponent of their curricula, and this could rangetreatment coverage varies greatly by state. In manyfrom a lecture course to a single grand rounds.8states, services are limited to acute care of substance use problems. This limitation in coverageWith these challenges in mind, Physicianis in contrast to evidence that substance useLeadership on National Drug Policy convened aproblems require a comprehensive continuum ofmeeting on November 29, 2001, “Adolescentscare. For adolescents covered by private insur-and Substance Abuse: Risks, Treatment and theance, a lack of comprehensive substance abuseJuvenile Justice System,” at the National Presscoverage is a major barrier to accessing treat-Club in Washington, DC. The goal of this meet-ment. In order to better address adolescent sub-ing was to identify and present the latest datastance use problems, health insurance coverageon prevalence, prevention, treatment, and themust be equal to that of other chronic diseases.juvenile justice system. While the PLNDP’s earlier activities focused on illicit drugs, this reportThe treatment sector is entering a “renais-on adolescents encompasses alcohol, tobaccosance” of new research. “The number of studiesand other drugs.evaluating formal substance abuse treatmentprograms for adolescents more than doubledThis report is structured as a public health strat-from 1997 to 2001 and promises to double againegy planning report similar to Healthy Peoplewithin the next three years.” 7 This research has2000 and Healthy People 2010 and is an out-translated into advances in treatment methodol-growth of the November PLNDP-sponsoredogy, with promising new approaches that aremeeting. It is organized into initiatives, withincomprehensive and integrative and involve thewhich PLNDP has identified policy recommen-families, schools, healthcare professionals, anddations and priorities for further research.communities. Unfortunately, the promise ofDavid. C. Lewis, MDKathryn Cates-WesselProject DirectorAssociate Director2 INTRODUCTION OF THE PROBLEM
THE DATA ONADOLESCENTSUBSTANCE USEPROBLEMSINTRODUCTION OF THE PROBLEM 3
AMERICANS VIEW DRUG ABUSE ASA MAJOR HEALTH PROBLEMWhen polled about their personal views, 67 percent ranked drugs or drug abuse as among the top two or three problems facing Americanteenagers today, in addition to alcohol at 13 percent, smoking at 6 percent and mental health at 3 percent [table 1]. Eighty-two percent ofrespondents ranked drug abuse as among the top ten serious health problems, ranking it as a “very serious problem,” in addition to drunkdriving at 75 percent, smoking at 68 percent and alcohol abuse at 65 percent [table 2].Americans’ Views Of The 2 Or 3 MostImportant Problems Facing Teenagers TodayAmericans’ Views Of TheSeriousness Of Health Problems(Top ten of thirty-six problems)82% Drug abuse67% Drugs/drug abuse15% Violence/crime/guns78% Cancer13% Alcohol75% Drunk driving13% Peer pressure74% Heart disease13% Sexual activity73% HIV/AIDS10% Breakdown of homelife/related issues71% Violence9% Sexually transmitted disease/HIV/AIDS69% Child abuse9% Education9% Lack of good character/morality68% Smoking8% Teen pregnancy65% Alcohol abuse6% Smoking65% Stress3% Mental health3% Medical problemstable 1% saying “very serious problem”table 2Data Source: Adapted from Blendon, R., Harvard School of Public Health and The Robert Wood Johnson Foundation.“Report on Public Attitudes Toward Illegal Drug Use and Drug Treatment.” September, 2000. Unpublished data.4 INTRODUCTION OF THE PROBLEM
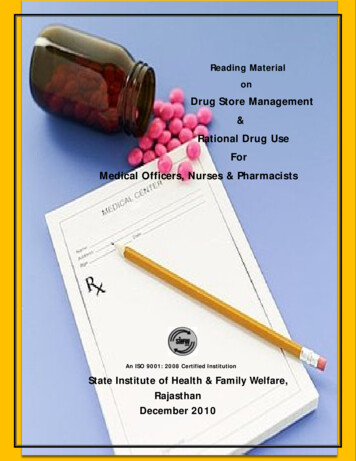
The Monitoring the Future Study, an ongoing study of thebehaviors, attitudes and values of adolescents and young adultsDaily Use PercentagesAmong 12th Graders: 1992 vs. 2001in America reports trends in substance use and abuse. Somehighlights of the latest data follow:19.01992 Data2001 Data17.2ALCOHOLat least once in their lives in 2001. Over one-fifth (21.5 percent) of 8th grade students reportcurrent alcohol use; this percentage increases to 39 percentof 10th grade students and nearly 50 percent of 12th gradestudents.Percent of respondents 23 percent of 8th grade students reported having been drunk5.8 Among 12th grade students, 30 percent report consuming fiveor more drinks in a row in the two weeks prior to the survey.0.81.91.4TOBACCO Over one-fifth of 12th grade students report smoking tobaccocigarettes on a dailybasis.1Being Drunk(on alcohol)SmokingTobaccoUsing MarijuanaData Source: Monitoring the FutureILLICIT SUBSTANCESfigure 2 Over one-half (54 percent) of adolescents have tried an illicitsubstance by the time they have finished high school. 29 percent of 12th grade students tried an illicit substanceother than marijuana in 2001. Among 8th, 10th and 12th grade students, AngloAmericans reported substantially higher rates of use forboth legal and illicit substances than their African Americancounterparts.“Compared to the early '90s, high school studentsare practicing fewer unhealthy behaviors suchas tobacco use, marijuana use, risky sexualbehaviors, and other potentially dangerousbehaviors that increase their risk for injury,illness, and death.”(Source: Centers for Disease Control and Prevention. 2001 Youth RiskBehavior Surveillance System (YRBSS). Fact Sheet. June 27, 2002.Available at www.cdc.gov.) Ecstasy (MDMA) was the primary drug showing an increase inuse among students in all grade levels in 2001.When approaching adolescent substance use, we must be careful notto label or pathologize a young person who has started to use drugs.More recently, there has been a great deal of focus on theAn adolescent who begins using is typically not dependent; the devel“leveling off” of the trends in adolescent substance abuse, butopment of a serious clinical substance use disorder usually takesthis focus ignores the fact that the rates of daily use amongplace no sooner than a year or two from the commencement of use.212th graders in 2001 were substantially higher than those docMany adolescents who drink, smoke, or take illicit drugs will neverumented for 1992. (See figure 2)develop a physical dependency or have negative experiences as aresult of using substances. However, heavier, longer-term, and morefrequent use is likely to result in problems with health, school,INTRODUCTION OF THE PROBLEM 5
Past Month Illicit Drug UseBy Intensity Of Alcohol Use100Percent who report past month drug use908070Heavy Drinker6050Binge Drinker40Other Drinker3020100Non-Drinker19941995199619971998Data Source: National Household Survey on Drug Abuse, 1998figure 3Past Month Illicit Drug Use ByWhether Or Not They Smoke Cigarettes100Percent who report past month drug 1995199619971998Data Source: National Household Survey on Drug Abuse, 1998figure 46 INTRODUCTION OF THE PROBLEM
Change In Past Month Use Of Substances By Age10090Use in the past month (%)8070605040302010121314Alcohol Use151617Tobacco Use18192021AgeBinge Alcohol Use22-2324-2526-29Any Illicit Drug Use30-3435-3950-6465 Marijuana UseSource: Dennis, ML. "Treatment Research on Adolescents Drug and Alcohol Abuse: Despite Progress, Many Challenges Remain(Invited Commentary)." Connection. Washington, DC: Academy for Health Services Research and Health Policy. May, 2002.figure 5work, and/or the law. This is consistent with our understanding ofto alcohol. The general progression typically moves from
President of Montefiore Medical Center and Former Chair of the Association of American Medical Colleges (AAMC). WILLARD GAYLIN, MD Clinical Professor of Psychiatry at Columbia College of Physicians and Surgeons. Co-founder of the Hastings Center. Former President and Chair of the Hastings Center and currently a member of the Board of Directors.