Transcription
Chapter 2:Medicaid and theOpioid Epidemic
Chapter 2: Medicaid and the Opioid EpidemicMedicaid and the Opioid EpidemicKey Points The opioid epidemic, which has reached most communities across the U.S., disproportionatelyaffects Medicaid beneficiaries. For example:–– Medicaid beneficiaries age 18–64 have a higher rate of opioid use disorder than privatelyinsured individuals, comprising about 12 percent of all civilian, non-institutionalizedadults in this age group but about one-quarter of those with an opioid use disorder.–– Medicaid beneficiaries are prescribed pain relievers at higher rates than those with othersources of insurance.–– They also have a higher risk of overdose and other negative outcomes, from bothprescription opioids and illegal opioids such as heroin and illicitly manufactured fentanyl.–– But Medicaid beneficiaries with an opioid use disorder have higher treatment rates thanprivately insured adults with the same condition. 60State Medicaid programs are responding to the opioid crisis by covering treatment, innovatingin the delivery of care, and working to reduce misuse of prescription opioids. Medicaidprograms cover many components of medication-assisted treatment (MAT), therecommended treatment for opioid use disorders under current evidence-based guidelines.However, there is considerable variation in available services across states, since many areoptional under the Medicaid statute.States are using a variety of legal authorities to expand both the availability of treatment andthe number of individuals eligible for such care. They are also working to organize andintegrate physical health and substance use disorder treatment delivery systems to providemore effective care. These mechanisms include Section 1115 waivers, the health homesoption, and the rehabilitation option.States are also focused on identifying opioid overprescribing in order to prevent opioid usedisorders from developing. These approaches include prescription drug monitoring programs,patient review and restriction programs, drug utilization reviews, utilization managementtechniques such as quantity limits or prior authorization requirements for prescription opioids,and the use of non-opioid pain management therapies.Even so, many Medicaid enrollees with an opioid use disorder are still not receiving treatment.Barriers to care include individuals not perceiving the need for treatment or fearing the stigmaof having a substance use disorder, a fragmented and poorly funded delivery system, privacyregulations that limit care coordination, a shortage of Medicaid-participating providers andproviders trained in MAT, and gaps in the continuum of care associated with both restrictivecoverage policies and the institution for mental diseases (IMD) payment exclusion.June 2017
Chapter 2: Medicaid and the Opioid EpidemicCHAPTER 2: Medicaidand the Opioid EpidemicMuch has been written about the opioid epidemicin America and its devastating effects on familiesand communities. In many ways, Medicaid isat its center. The epidemic disproportionatelyaffects Medicaid beneficiaries, and state Medicaidprograms are taking the lead in identifying andtailoring strategies to prevent and treat opioid usedisorder and reduce its adverse effects. In 2015,Medicaid beneficiaries age 18–64 had a higherrate of opioid use disorder than privately insuredindividuals: they comprised about 12 percentof all civilian non-institutionalized adults in thisage group but about one-quarter of those withan opioid use disorder (SHADAC 2017). Medicaidbeneficiaries are prescribed pain relievers at higherrates than those with other sources of insurance.They also have a higher risk of overdose and othernegative outcomes, from both prescription opioidsand illegal opioids, such as heroin and illicitlymanufactured fentanyl (McMullen 2016, Zhou etal. 2016, Sharp and Melnick 2015, Whitmire andAdams 2010, CDC 2009). In addition, Medicaidbeneficiaries with an opioid use disorder havehigher treatment rates than privately insured withthe same condition (SHADAC 2017).Beyond the human toll, opioid misuse and opioiduse disorder have large financial effects. In 2012,81 percent of the estimated 1.5 billion in hospitalcharges related to neonatal abstinence syndromein infants born to women using opioids was billedto Medicaid (Patrick et al. 2015).1 In 2012, inpatienthospital charges for individuals with seriousinfections associated with an opioid use disorderexceeded 700 million, and Medicaid enrolleesaccounted for 43 percent of those hospitalizations(Ronan and Herzig 2016).Opioids are a class of drugs that include manyprescription pain relievers (such as oxycodone,hydrocodone, codeine, morphine, fentanyl, andmethadone) and illegal versions such as heroin andillicitly manufactured fentanyl (CDC 2016a). WhileReport to Congress on Medicaid and CHIPhistorically considered a moral failing, opioid usedisorder—like other substance use disorders—isa chronic brain disease. It typically develops overtime with repeated misuse of opioids and involvesa three-stage cycle: binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation.It is further characterized by clinically significantimpairments in health, social function, and controlover opioid use; development of tolerance; andwithdrawal symptoms. An opioid use disorder canrange from mild to severe and from temporary tochronic. Continued use increases the severity ofeffects and changes brain function, persisting longafter use has stopped. The extent to which thesechanges can be reversed, and how long that mighttake, is unknown. Even so, opioid use disorder canbe effectively treated and managed; recurrencerates (also referred to as relapse rates) are nohigher than those of other chronic illnesses suchas type 2 diabetes, hypertension, or asthma (OSG2016, ASAM 2014).Medicaid is responding to the opioid crisis bycovering treatment, innovating in the delivery ofcare, and working with other state agencies toreduce misuse of prescription opioids. However,there are gaps in the continuum of care, and statesvary in the extent to which they cover neededtreatment. An insufficient supply of providers alsolimits access to treatment in many locations. Thedelivery systems for physical health and behavioralhealth (which encompasses mental illnessand substance use disorders) are traditionallyseparately organized and financed; the resultingfragmentation and lack of coordination can impedeaccess to care and lead to inappropriate andinsufficient use of services, poor health status,and increased costs (OSG 2016). The stigmaassociated with substance use disorders can alsoaffect the willingness of individuals to seek help,providers to offer care, and policymakers to financetreatment.Although the opioid epidemic has cut a broadswath through our society—affecting rich andpoor, as well as urban, suburban, and ruralcommunities—this chapter focuses on how it61
Chapter 2: Medicaid and the Opioid Epidemicaffects Medicaid beneficiaries and state strategiesto address this crisis. The chapter begins bydocumenting the prevalence of opioid use andopioid use disorder among different groups ofbeneficiaries, including children, pregnant women,working-age adults, older adults, and people withdisabilities. It goes on to describe how Medicaidprograms are covering screening and treatmentservices for opioid use disorder, highlighting thelegal authorities that states are using to expandnot only benefits but also the number of enrolleeseligible for such care. It then details how Medicaidprograms are working to reduce inappropriateopioid prescribing, and concludes by describingthe challenges to further improving access totreatment for Medicaid beneficiaries with an opioiduse disorder.Opioid Use, Misuse, andUse Disorders: Prevalence,Comorbidities, and AdverseOutcomesPrescription opioid misuse occurs when a personuses the drug without a prescription; in greateramounts, more often, or longer than prescribed; orin other ways contrary to the prescribing clinician’sdirections (Hughes et al. 2016). Opioid use disorder,an umbrella term for both pain reliever and heroinuse disorders, is a brain disease that typicallydevelops over time with repeated misuse ofopioids. It is characterized by clinically significantimpairments in health, social function, and controlover opioid use; development of tolerance; andwithdrawal symptoms that occur after stopping orreducing use.Below, we describe the prevalence of andsociodemographic characteristics associated withopioid use, misuse, and opioid use disorder. Wealso present information on health conditions thatcan affect or be affected by opioid use, and rates oftreatment for opioid use disorder. While not all the62data in this section are specific to Medicaid, theyare useful in understanding the scope and natureof the epidemic.Prevalence of opioid use, misuse, anduse disorderIn 2015, 2 million people (0.8 percent of civilian,non-institutionalized individuals age 12 andolder in the U.S.) had a prescription pain relieverdisorder, and some 12.5 million people (4.7 percentof individuals age 12 and older) had misusedprescription pain relievers in the previous year(Bose et al. 2016, Hughes et al. 2016). Rates ofprescription opioid use and misuse differed amongpopulation groups (Table 2-1).Link between prescription opioids andheroin usePeople who misuse opioids may turn fromprescription drugs to illegal drugs, which may becheaper and more potent; the share that do so issmall, at less than 5 percent (Compton et al. 2016,Wu et al. 2011). Most heroin users, however, havea history of prescription opioid misuse (Joneset al. 2015a). For example, one study foundthat among people who used both prescriptionopioids for non-medical reasons and heroin duringthe previous year, 77.4 percent reported usingprescription opioids before initiating heroin use(Jones 2013).2 A recent study comparing data from2001–2002 to 2012–2013 found an increase inthe share of white individuals whose heroin usewas preceded by non-medical use of prescriptionopioids. There was, however, a reduction in thepercentage of non-white users who reported nonmedical prescription opioid use before initiationof heroin use over the same time span (Martins etal. 2017). The increase in heroin overdose deathsrates has occurred concurrently with an increase inprescription opioid overdoses (Jones et al. 2015a).June 2017
Chapter 2: Medicaid and the Opioid EpidemicTABLE 2-1. Share of Prescription Pain Reliever Use and Misuse in Past Year among U.S. PersonsAge 12 and Older, by Demographic Characteristics, 2015Demographic groupAll individuals age 12 and olderPrescription pain reliever Prescription pain relieveruse past yearmisuse past year36.4%4.7%12–1722.73.918–2534.88.526 and ack38.34.4Hispanic30.25.0Asian22.01.8American Indian or Alaska Native38.75.6Native Hawaiian or other Pacific Islander32.75.4Two or more races44.88.4Less than high school37.45.7High school graduate38.94.9Some college or associate degree42.85.7College graduate38.13.1Working full time34.94.8Working part e and ethnicityEducation (among persons 18 and older)Employment status (among persons 18 and older)Notes: Prescription pain reliever use means the use of one’s own prescription medication as directed by the prescribing clinician.Prescription pain reliever misuse means taking a prescription medication without a prescription; taking a prescription medicationin greater amounts, more often, or longer than prescribed; or taking a prescription medication in any other way contrary to theprescribing clinician’s directions. Table shows percentage of given U.S. population group with prescription pain reliever use ormisuse in past year, as reported in the 2015 National Survey on Drug Use and Health (SAMHSA 2016a).1Other indicates individuals not in the labor force (e.g., students, homemakers, retirees, or people not working due to disability).Source: SHADAC 2017, Hughes et al. 2016, SAMHSA 2016a.Report to Congress on Medicaid and CHIP63
Chapter 2: Medicaid and the Opioid EpidemicPrevalence of opioid disorders byinsurance statusIn 2015, Medicaid beneficiaries were more likelyto abuse or have a dependency on an opioid in theprevious year than privately insured adults age18–64. Medicaid beneficiaries have similar ratesof opioid abuse and dependence (both consideredan opioid use disorder) as uninsured adults (Table2-2). Medicaid enrollees, however, are more likelythan privately insured and uninsured adults to haveboth used heroin in the past and had a pain relieverdependence in the previous year. They are themost likely to have ever used heroin and misused aprescription pain reliever.Opioid use disorder occurs across all Medicaidbeneficiary groups and demographics, but certaincomorbid conditions, predictors of future usedisorder, and outcomes differ.Geographic differences. There has beensubstantial media attention on opioid misuse andopioid use disorder in rural areas (Bohner 2017,Gliha 2017, Runyon 2017, Tanner 2016). Even so,using national datasets, misuse of prescriptionopioids between rural and more urban areas showeither similar rates of misuse or higher rates inurban and suburban areas (Lenardson et al. 2016,Rigg and Monnat 2015, SAMHSA 2013a). Thesestatistics may mask other important differences,however. For example, studies documented ahigher prevalence of prescription pain relievermisuse in certain vulnerable rural populations,such as adolescents, women who are pregnant orexperiencing partner violence, and persons withco-occurring disorders. One study found highermisuse rates among specific rural subpopulationscompared to their urban counterparts, includingthose who had less than a high school education,were uninsured, were in fair or poor health, or hadlow incomes (Lenardson et al. 2016, Monnat andRigg 2015, Havens et al. 2011).Additionally, there has been a shift in thedemographics of heroin use over the past 50 years.No longer centered in inner cities and among racial64minorities, heroin use is now more widespreadgeographically, involving primarily white men andwomen in their late 20s living outside of largeurban areas (Cicero et al. 2014). States with thehighest opioid overdose death rates also includestates with large rural populations, such asKentucky, New Hampshire, and West Virginia (Ruddet al. 2016).Pregnant women and infants. Opioids are widelyprescribed among women of childbearing age,with over one-third of Medicaid-enrolled womenfilling an opioid prescription annually (Ailes et al.2015). Between 2005 and 2014, nearly 1 percent ofpregnant women and 2.3 percent of non-pregnantwomen of reproductive age reported non-medicaluse of a prescription opioid in the previous 30days. Of these women reporting non-medical useof a prescription opioid, pregnant women weremore likely to receive their opioid from a doctor(46 percent) than were non-pregnant women (28percent) (Kozhimannil et al. 2017). Infants bornto women using opioids during pregnancy mayexperience neonatal abstinence syndrome, whichmanifests in the first few days of life with thefollowing symptoms: difficulty with mobility andflexing; inability to control heart rate, temperature,and other autonomic functions; irritability; poorsucking reflex; impaired weight gain; and, in somecases, seizures (Tolia et al. 2015, Patrick et al.2015). From 2004 to 2013, neonatal intensivecare unit admissions for infants with neonatalabstinence syndrome increased from 7 cases per1,000 admissions to 27 cases per 1,000 admissions(Tolia et al. 2015).Adolescents. Adolescents who have an opioidprescription by 12th grade are more likely tomisuse prescription opioids by the time they are 23than those with no history of an opioid prescription(Miech et al. 2015). A history of prescription opioidmisuse is also associated with initiating heroinuse. Those beginning misuse of prescriptionopioids between the ages of 10 and 12 have thehighest risk of transitioning to heroin use, and thatassociation appears to be consistent across race,ethnicity, and income groups (Cerdá et al. 2015).June 2017
Chapter 2: Medicaid and the Opioid EpidemicTABLE 2-2. Substance Misuse, Abuse, and Dependence in Adults Age 18–64, by Insurance Status,2015Type of useIllicit drug dependence or abuse,past yearNumber ofadults age18–64Percentage ofall adultsage 58,3150.20.20.20.3Illicit drug or alcohol abuse, pastyear7,448,8203.82.73.9*4.7*Pain reliever dependence, past sed pain reliever, past 30 days3,309,2451.72.61.3*2.6Ever misused pain reliever24,194,17112.414.011.7*14.5Misused OxyContin, past 12 months1,581,1810.81.20.6*1.4Ever used heroin1,855,9672.45.21.5*3.2*Heroin dependence, past year555,2910.30.80.1*0.6Ever used heroin and had painreliever dependence, past year535,8530.30.80.2*0.4*Ever used heroin and ever misusedpain reliever1,123,8791.43.30.9*2.3*Ever misused pain reliever and hadheroin dependence, past year164,0510.20.60.1*0.6Illicit drug and alcohol abuse, pastyearPain reliever abuse, past year6,674,356Percentage of adults age 18–64 ineach coverage categoryNotes: Before the 2013 release of the updated Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), substanceuse disorders were split into two categories, abuse and dependence (e.g., an alcohol use disorder could be either a diagnosis ofalcohol abuse or a diagnosis of alcohol dependence). The DSM-5 no longer distinguishes between abuse or dependence and usesone designation for substance use disorders and measures them on a continuum from mild to moderate to severe (e.g., a mildalcohol use disorder or a severe opioid use disorder). The 2015 National Survey on Drug Use and Health (NSDUH), however, usedthe older definition of abuse and dependence. In this survey, pain reliever misuse means taking a prescription medication withouta prescription; taking a prescription medication in greater amounts, more often, or longer than prescribed; or taking a prescriptionmedication in any other way contrary to the prescribing clinician’s directions. We used the following hierarchy to assign individualswith multiple insurance coverage sources to a primary source: Medicare, private, Medicaid, other, or uninsured. Coverage source isdefined as of the time of the most recent survey interview.1Private health insurance coverage excludes plans that pay for only one type of service, such as accident coverage or dental care.* Difference from Medicaid is statistically significant at the 0.05 level.Source: SHADAC 2017.Report to Congress on Medicaid and CHIP65
Chapter 2: Medicaid and the Opioid EpidemicWorking-age adults. Factors that predict misuseby working-age adults include being male,unmarried, low income, and uninsured (Cicero etal. 2014). Available research suggests that opioiddeaths and opioid-related emergency departmentvisits rise when county-level and state-levelunemployment rates increase (Hollingsworth et al.2017). A recent study found that among adults age26 and older, unemployed individuals were mostlikely to misuse prescription opioids, followed bythose employed full-time. Individuals not in thelabor force (e.g., students, homemakers, retirees,or persons not working due to disability) were leastlikely to misuse a prescription opioid (Perlmutter etal. 2017). People involved with the criminal justicesystem, by contrast, have higher rates of substanceuse disorders and heroin use in particular (Evansand Sullivan 2015, Belenko et al. 2013).Older adults. There is relatively little high-qualityresearch on prescription opioid misuse amongolder adults (Maree et al. 2016). One studyfound that in 2012, over one-third of Medicareenrollees with Part D prescription drug coveragefilled at least one prescription for an opioid, andthese individuals had more comorbidities thanthose without an opioid prescription. Those withparticularly high use of opioids were more likelyto be under age 65 and receiving a low-incomesubsidy (MedPAC 2015).3 The Medicare populationhas one of the highest and fastest-growing ratesof diagnosed opioid use disorder. Mortality ratesamong older adults also increased and surpassedrates for younger adults in 2012 and 2013 (Lembkeand Chen 2016, West et al. 2015). Opioids andbenzodiazepines (which are more likely to beprescribed to older adults to treat anxiety andsleep disorders) are also a high-risk combination,particularly in such older individuals (Nuckols et al.2014, AOA and SAMHSA 2012).People with disabilities. People with disabilitiesare more likely to be prescribed opioid pain relieversdue to their higher rates of painful conditions,but there are no nationally representative dataon opioid misuse in populations of people withdisabilities (NCHS 2016). One systematic review66and data synthesis found that rates of opioidmisuse averaged between 21 percent and 29percent among patients with chronic pain, andrates of addiction averaged between 8 percentand 12 percent (Vowles et al. 2015). Anothersystematic review of studies of opioid prescribingfor patients with low back pain found that up to 25percent of patients receiving these medicationsexhibited some signs of medication misuse(Martell et al 2007).Utilization of treatment for opioid usedisorder by insurance statusMedicaid beneficiaries with opioid use disorderare more likely to receive treatment than privatelyinsured adults with the disorder, both inpatient andoutpatient treatment. They are about three timesmore likely to receive drug or alcohol treatmentin a hospital as an inpatient or in a residentialtreatment facility than privately insured adults, andthey are almost twice as likely to receive care onan outpatient basis from a mental health centerthan privately insured adults. Treatment services,however, remain substantially underutilized; this isoften referred to as the treatment gap. In 2015, onlyabout 32 percent of Medicaid enrollees with anopioid use disorder were receiving treatment (Table2-3).It is unclear why Medicaid enrollees are morelikely to receive treatment than privately insuredindividuals. Many factors influence whether anindividual seeks care; for example, a belief thatone does not need treatment, an unwillingness orinability to stop using drugs, concerns about theeffect on one’s job, inability to afford the cost oftreatment, lack of information about treatmentoptions, and lack of available treatment programsin the community (OSG 2016). Another possibleexplanation for the difference in rates of treatmentbetween individuals covered by Medicaid andthose with private insurance is that private plansmay impose higher out-of-pocket costs or morestringent coverage limits, which discourageindividuals from seeking care. Those withJune 2017
Chapter 2: Medicaid and the Opioid Epidemicemployer-sponsored coverage may also worry thattheir employer will find out about their substanceuse disorder, and thus they do not get treatment(Bouchery et al. 2012). Differences in rates oftreatment receipt were also observed by variousdemographic characteristics, such as age, race,and educational level (Bali 2013).TABLE 2-3. Treatment for Substance Use Disorder among Adults Age 18–64 with Past Year OpioidUse Disorder, by Medicaid and Private Insurance Coverage, 2015Treatment characteristicsPercentageof adults age18–64 withpast yearopioid usedisorderPercentage in eachcoverage categoryMedicaidPrivate1Currently receiving treatment or counseling20.2%32.3%17.2%*Ever received alcohol or drug treatment56.064.349.9*Perceived the need for treatment or counseling for alcohol or druguse11.416.06.1*Perceived the need for treatment or counseling for pain reliever usedisorder7.1N/AN/APerceived the need for treatment or counseling for heroin usedisorder3.8N/AN/AReceived treatment in a hospital overnight as an inpatient10.416.46.2*Received treatment in a residential drug rehabilitation facility11.721.87.1*Received treatment in a drug rehabilitation facility as an outpatient19.630.416.2*Received treatment in a mental health center or facility as anoutpatient11.022.08.0*5.89.64.0Received treatment in a private doctor’s office12.715.415.4Participated in a mutual aid group such as Alcoholics Anonymous orNarcotics Anonymous20.226.019.0Received treatment in another place10.7N/A9.8During previous 12 monthsReceived treatment in an emergency roomNotes: N/A indicates that the estimate is based on too small a sample or is too unstable to present. We used the following hierarchyto assign individuals with multiple coverage sources to a primary source: Medicare, private, Medicaid, other, or uninsured. Coveragesource is defined as of the time of the most recent survey interview.1Private health insurance coverage excludes plans that pay for only one type of service, such as accident coverage or dental care.* Difference from Medicaid is statistically significant at the 0.05 level.Source: SHADAC 2017.Report to Congress on Medicaid and CHIP67
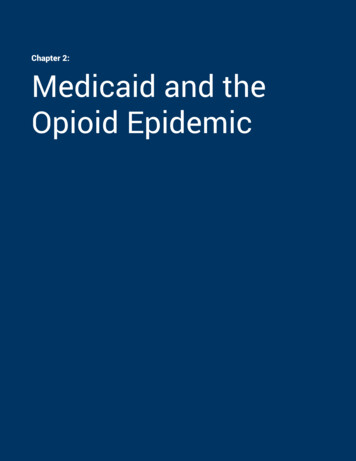
Chapter 2: Medicaid and the Opioid EpidemicOpioid use disorder and comorbiditiesIt is important to note that there are health factorsthat can exacerbate disorders and make effectivetreatment difficult. For example, comorbiditiessuch as mental illness or misuse of othersubstances may interfere with a patient’s abilityto seek care (e.g., they are too weak to travel, orthese conditions interfere with adherence). Inaddition, other conditions may be the main focusof a patient’s treatment, with opioid use disorderbeing ignored or considered less critical to treat.For example: 68Heroin use, in particular, is associated withother serious health conditions. When peopleinject heroin with shared needles, they areat risk of serious, long-term viral infectionssuch as HIV, hepatitis C, and hepatitis B.Intravenous drug use can also cause bacterialinfections of the skin, bloodstream, and heart(CDC 2015).People who use other substances are morelikely to misuse pain relievers (Bose et al.2016). For example, 5.9 percent of past-yearalcohol users also misused prescriptionpain relievers during the same time period.Among past-year heroin users age 12 andolder, 72.1 percent had misused prescriptionpain relievers during the same time period. Ofpeople age 12 and older who used marijuanain the past year, 16.2 percent also misusedprescription pain relievers during the sametime period (Bose et al. 2016). A significantpercentage of heroin users meet diagnosticcriteria for disorders involving other drugs(Jones et al. 2015a).There is a higher prevalence of opioid usedisorder among individuals with anxiety ormood disorders, such as major depressivedisorder or bipolar disorder, than in individualswithout these conditions (NIDA 2010). Amongthe 19.6 million adults age 18 and older in2015 with a past-year substance use disorder,2.3 million (11.9 percent) also had a seriousmental illness during the same period (Bose etal. 2016).Mortality associated with opioid useAlthough opioids are useful for pain control whenused appropriately, their mood-enhancing effectsand addictive properties can lead to misuse,opioid use disorder, and negative outcomes, suchas increased risk of brain and organ damageand death. National statistics on opioid-relateddeath rates specific to the Medicaid populationare not available, but drug overdose deaths inthe United States overall nearly tripled from 1999to 2014 (Rudd et al. 2016). During this period,overdose death rates were highest among the 25to 54 age group. Overdose death rates for nonHispanic whites and American Indian or AlaskanNatives were higher than rates for non-Hispanicblacks and Hispanics, and men were more likelyto die from an overdose than women (althoughthe mortality gap between men and women isclosing) (CDC 2016b). State-level data on opioidoverdose deaths show Medicaid beneficiarieshave a higher risk of overdose and adverse effectsfrom both prescription opioids and illegal versions,including heroin and illicitly manufactured fentanyl(McMullen 2016, Zhou et al. 2016, Sharp andMelnick 2015, Whitmire and Adams 2010, CDC2009).Death rates vary by type of opioid. There isprogress in preventing methadone deaths: deathrates declined by 9.1 percent from 2014 to 2015(Figure 2-1). During the same time period, however,overdose deaths associated with other syntheticopioids increased by 72.2 percent (most likelydue to greater availability of illicitly manufacturedfentanyl), while natural or semisynthetic opioiddeath rates increased by 2.6 percent (Rudd et al.2016, Gladden et al. 2016).4 Heroin death ratesincreased by 20.6 percent overall and acrossall demographic groups and regions. Of the 28states with high-quality data permitting state-levelanalysis, 16 experienced increases in death ratesinvolving synthetic opioids other than methadone,June 2017
Chapter 2: Medicaid and the Opioid Epidemicand 11 saw increases in heroin death rates. WestVirginia had the highest death rate associatedwith opioid use, followed in descending order byNew Hampshire, Kentucky, Ohio, and Rhode Island.The largest overall changes in rates of deathfrom synthetic opioids other than methadoneoccurred in Massachusetts, New Hampshire,Ohio, Rhode Island, and West Virginia; the largestoverall changes in rates of heroin deaths werein Connecticut, Massachusetts, Ohio, and WestVirginia. New Mexico, Oklahoma, and Virginia sawdecreases in rates of deaths due to natural orsemisynthetic opioids, while increases occurredin Massachusetts, New York, North Carolina, Ohio,and Tennessee (Rudd et al. 2016).FIGURE 2-1. Opioid Overdose Death Rates by Opioid Type, 2005–2015Notes: Other opioids in this figure include natural opioids (e.g., morphine and codeine), semisynthetic opioids(e.g., oxycodone, hydrocodone, hydromorphone, and oxymorphone), and synthetic opioids other than methadone(e.g., tramadol and fentanyl).Source: MACPAC, 2017, analysis
sources of insurance. - They also have a higher risk of overdose and other negative outcomes, from both prescription opioids and illegal opioids such as heroin and illicitly manufactured fentanyl. - But Medicaid beneficiaries with an opioid use disorder have higher treatment rates than privately insured adults with the same condition.