Transcription
Leader’s GuideCognitive Behavioural & RelapsePrevention StrategiesTreatnet Training Volume B, Module 3: Updated 18 September 20071
Training goals1.Increase knowledge of cognitive behaviouraltherapy (CBT) and relapse prevention (RP)strategies and resources.2.Increase skills using CBT and RP strategiesand resources.3.Increase application of CBT and RP strategiesfor substance abuse treatment2
Module 3: WorkshopsWorkshop 1: Basic Concepts of CBT and RPWorkshop 2: Cognitive BehaviouralStrategiesWorkshop 3: Methods for Using CognitiveBehavioural Strategies3
Workshop 1:Basic Concepts of CBT and RP4
Pre-assessment10 Min.Please respond to the pre-assessmentquestions in your workbook.(Your responses are strictly confidential.)5
IcebreakerIf you had to move to an uninhabited island,what 3 things would you take with you andwhy? (food and water are provided)6
Training objectivesAt the end of this workshop, you will:1.Understand that substance use is a learned behaviour thatcan be modified according to principles of conditioning andlearning2.Understand key principles of classical and operantconditioning and modelling3.Understand how these principles apply to the treatmentsdelivered in cognitive behavioural therapy and relapseprevention training4.Understand the basic approaches used in cognitivebehavioural therapy and how they apply to reducing druguse and preventing relapse5.Understand how to conduct a functional analysis and knowabout the 5 Ws of a client’s drug use7
What are CognitiveBehavioural Therapy (CBT)and Relapse Prevention(RP)?8
What is CBT and how is it used inaddiction treatment?¾CBT is a form of “talk therapy” that is used toteach, encourage, and support individualsabout how to reduce / stop their harmful druguse.¾CBT provides skills that are valuable inassisting people in gaining initial abstinencefrom drugs (or in reducing their drug use).¾CBT also provides skills to help people sustainabstinence (relapse prevention)9
What is relapse prevention (RP)?Broadly conceived, RP is a cognitive-behaviouraltreatment (CBT) with a focus on the maintenancestage of addictive behaviour change that has twomain goals: To prevent the occurrence of initial lapses aftera commitment to change has been made and To prevent any lapse that does occur fromescalating into a full-blow relapseBecause of the common elements of RP and CBT, wewill refer to all of the material in this training moduleas CBT10
Foundation of CBT:Social Learning TheoryCognitive behavioural therapy (CBT)¾ Provides critical concepts of addiction and howto not use drugs¾ Emphasises the development of new skills¾ Involves the mastery of skills through practise11
Why is CBT useful? (1)¾CBT is a counseling-teaching approachwell-suited to the resource capabilities ofmost clinical programs¾CBT has been extensively evaluated inrigorous clinical trials and has solidempirical support¾CBT is structured, goal-oriented, andfocused on the immediate problems facedby substance abusers entering treatmentwho are struggling to control their use12
Why is CBT useful? (2)¾CBT is a flexible, individualized approach thatcan be adapted to a wide range of clients aswell as a variety of settings (inpatient,outpatient) and formats (group, individual)¾CBT is compatible with a range of othertreatments the client may receive, such aspharmacotherapy13
Important concepts in CBT (1)In the early stages of CBT treatment, strategiesstress behavioural change. Strategies include:¾planning time to engage in non-drug relatedbehaviour¾avoiding or leaving a drug-use situation.14
Important concepts in CBT (2)CBT attempts to help clients: Follow a planned schedule of low-risk activities Recognise drug use (high-risk) situations andavoid these situations Cope more effectively with a range of problemsand problematic behaviours associated withusing15
Important concepts in CBT (3)As CBT treatment continues into later phasesof recovery, more emphasis is given to the“cognitive” part of CBT. This includes: Teaching clients knowledge about addictionTeaching clients about conditioning, triggers, andcravingTeaching clients cognitive skills (“thoughtstopping” and “urge surfing”)Focusing on relapse prevention16
Foundations of CBTThe learning and conditioning principlesinvolved in CBT Modelling17
Classical conditioning: ConceptsConditioned Stimulus (CS) does not produce aphysiological response, but once we have stronglyassociated it with an Unconditioned Stimulus (UCS) (e.g.,food) it ends up producing the same physiologicalresponse (i.e., salivation). 18
Classical conditioning: Addiction¾Repeated pairings of particular events,emotional states, or cues with substance usecan produce craving for that substance¾Over time, drug or alcohol use is paired withcues such as money, paraphernalia, particularplaces, people, time of day, emotions¾Eventually, exposure to cues alone producesdrug or alcohol cravings or urges that are oftenfollowed by substance abuse19
Classical conditioning: Application toCBT techniques (1)Understand and identify “triggers”(conditioned cues)¾ Understand how and why “drug craving”occurs¾20
Classical conditioning: Application to CBTtechniques (2)Learn strategies to avoid exposure totriggers¾ Cope with craving to reduce /eliminate conditioned craving overtime¾21
Operant conditioning: Addiction (1)Drug use is a behaviour that is reinforcedby the positive reinforcement that occursfrom the pharmacologic properties of thedrug.22
Operant conditioning: Addiction (2)Once a person is addicted, drug use isreinforced by the negative reinforcement ofremoving or avoiding painful withdrawalsymptoms.23
Operant conditions (1)Positive reinforcement strengthens aparticular behaviour (e.g.,pleasurable effects from thepharmacology of the drug; peeracceptance)24
Operant conditions (2)Punishment is a negative condition thatdecreases the occurrence of a particularbehaviour (e.g., If you sell drugs, you willgo to jail. If you take too large a dose ofdrugs, you can overdose.)25
Operant conditions (3)Negative reinforcement occurs when a particularbehaviour gets stronger by avoiding or stopping anegative condition (e.g., If you are having unpleasantwithdrawal symptoms, you can reduce them bytaking drugs.).26
Operant conditioning: Application to CBTtechniques¾Functional Analysis – identify highrisk situations and determinereinforcers¾Examine long- and short-termconsequences of drug use toreinforce resolve to be abstinent¾Schedule time and receive praise¾Develop meaningful alternativereinforcers to drug use27
Modelling: DefinitionModelling: To imitate someone or to follow theexample of someone. In behaviouralpsychology terms, modelling is a process inwhich one person observes the behaviour ofanother person and subsequently copies thebehaviour.28
Basis of substance use disorders: ModellingWhen applied to drug addiction, modelling is amajor factor in the initiation of drug use. Forexample, young children experiment withcigarettes almost entirely because they aremodelling adult behaviour.During adolescence, modelling is often the majorelement in how peer drug use can promoteinitiation into drug experimentation.29
Modelling: Application to CBT techniques¾¾¾¾Client learns new behaviours through roleplaysDrug refusal skillsWatching clinician model new strategiesPractising those strategiesObserve howI say “NO!”NO thanks, Ido not smoke30
CBT Techniques forAddiction Treatment:Functional Analysis / the 5Ws31
The first step in CBT: How does drug usefit into your life?¾One of the first tasks in conducting CBTis to learn the details of a client’s druguse. It is not enough to know that theyuse drugs or a particular type of drug.¾It is critical to know how the drug use isconnected with other aspects of a client’slife. Those details are critical to creatinga useful treatment plan.32
The 5 Ws (functional analysis)The 5 Ws of a person’s drug use (alsocalled a functional analysis) When? Where? Why? With / from whom? What happened?33
The 5 WsPeople addicted to drugs do not use them atrandom. It is important to know: The time periods when the client uses drugs The places where the client uses and buys drugs The external cues and internal emotional statesthat can trigger drug craving (why) The people with whom the client uses drugs orthe people from whom she or he buys drugs The effects the client receives from the drugs the psychological and physical benefits (whathappened)34
Questions clinicians can use to learnthe 5 Ws¾What was going on before you used?¾How were you feeling before you used?¾How / where did you obtain and use drugs?¾With whom did you use drugs?¾What happened after you used?¾Where were you when you began to think aboutusing?35
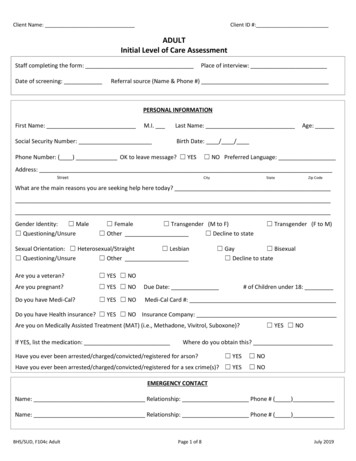
Functional Analysis or High-Risk Situations RecordAntecedentSituationThoughtsFeelings andSensationsBehaviourWhere was I?What was Ithinking?How was Ifeeling?What did I do?Who was withme?What washappening?What signalsdid I get frommy body?ConsequencesWhathappenedWhat did I use? after?How much did Iuse?How did I feelright after?Whatparaphernaliadid I use?How did otherpeople react tomy behaviour?What did otherpeople aroundme do at theAny othertime?consequences?
Activity 3: Role-play of a functionalanalysis25 Min.Script 1Conduct a role-play of a functional analysis:1. Review 5 Ws with client2. Provide analysis of how this information willguide treatment planning37
?Questions?Comments?38
Thank you for your time!End of Workshop 139
Workshop 2: Cognitive BehaviouralStrategies40
Training objectivesAt the end of this workshop, you will be able to:1.Identify a minimum of 4 cognitive behavioural techniques2.Understand how to identify triggers and high- and lowrisk situations3.Understand craving and techniques to cope with craving4.Present and practise drug refusal skills5.Understand the abstinence violation syndrome and howto explain it to clients6.Understand how to promote non-drug-relatedbehavioural alternatives41
CBT Techniques forAddiction Treatment:Functional Analysis &Triggers and Craving42
“Triggers” (conditioned cues)One of the most important purposes ofthe 5 Ws exercise is to learn about thepeople, places, things, times, andemotional states that have becomeassociated with drug use for your client.¾ These are referred to as “triggers”(conditioned cues).¾43
“Triggers” for drug use¾A “trigger” is a “thing” or an event or atime period that has been associated withdrug use in the past¾Triggers can include people, places,things, time periods, emotional states¾Triggers can stimulate thoughts of druguse and craving for drugs44
External triggers¾People: drug dealers, drug-using friends¾Places: bars, parties, drug user’s house,parts of town where drugs are used¾Things: drugs, drug paraphernalia, money,alcohol, movies with drug use¾Time periods: paydays, holidays, periodsof idle time, after work, periods of stress45
Internal triggersAnxiety¾ Anger¾ Frustration¾ Sexual arousal¾ Excitement¾ Boredom¾ Fatigue¾ Happiness¾46
Triggers & CravingsTriggerThoughtCravingUse47
Activity 3: Role-playing35 Min.Using the Internal and External TriggerWorksheets: Observe the role-play and how the clinicianidentifies triggers.Practise the role-play for 10 minutes48
CBT Techniques forAddiction Treatment:High-Risk & Low-RiskSituations49
High- and low-risk situations (1)¾ Situationsthat involve triggers andhave been highly associated withdrug use are referred to as high-risksituations.¾ Otherplaces, people, and situationsthat have never been associated withdrug use are referred to as low-risksituations.50
High- and low-risk situations (2)An important CBT concept is to teachclients to decrease their time in high-risksituations and increase their time in lowrisk situations.51
Activity 4: Role-playing35 Min.Using the “high-risk vs. low-risk”continuum (see Triggers charts), useinformation from the functional analysis(5Ws) and the trigger analysis toconstruct a high-risk vs. low-riskexercise. Role-play the construction ofa high- vs. low-risk analysis.52
CBT Techniques for AddictionTreatment: Strategies to Cope withCraving53
Understanding cravingCraving (definition)¾To have an intense desire for¾To need urgently; requireMany people describe craving as similar to ahunger for food or thirst for water. It is acombination of thoughts and feelings. There is apowerful physiological component to cravingthat makes it a very powerful event and verydifficult to resist.54
Craving: Different for different peopleCravings or urges are experienced in a variety ofways by different clients.For some, the experience is primarily somatic.For example, “I just get a feeling in my stomach,”or “My heart races,” or “I start smelling it.”For others, craving is experienced morecognitively. For example, “I need it now” or “Ican’t get it out of my head” or “It calls me.”55
Coping with craving¾Many clients believe that once they beginto crave drugs, it is inevitable that theywill use. In their experience, they always“give in” to the craving as soon as itbegins and use drugs.¾In CBT, it is important to give clients toolsto resist craving56
Triggers & cravingsTriggerThoughtCravingUse57
Strategies to cope with cravingCoping with Craving:1.2.3.4.5.6.Engage in non-drug-related activityTalk about craving“Surf” the cravingThought stoppingContact a drug-free friend or counsellorPray58
Activity 5: Role-playing20 Min.Use the “Trigger-Thought-Craving-Use”sheet to educate clients about craving anddiscuss methods for coping with craving.Role-play a discussion of techniques tocope with craving.59
CBT Techniques forAddiction Treatment:Drug Refusal Skills—Howto Say “No”60
How to say “No”: Drug refusal skills¾One of the most commonrelapse situations is when aclient is offered drugs by afriend or a dealer.¾Many find that they don’t knowhow to say “No.”¾Frequently, their ineffectivemanner of dealing with thissituation can result in use ofdrugs.61
Drug refusal skills: Key elementsImproving refusal skills/assertiveness:There are several basic principles ineffective refusal of drugs:1.2.3.4.5.Respond rapidly (not hemming and hawing, nothesitating)Have good eye contactRespond with a clear and firm “No” that does notleave the door open to future offers of drugsMake the conversation briefLeave the situation62
Drug refusal skills: Teaching methodsAfter reviewing the basic refusal skills,clients should practise them through roleplaying, and problems in assertive refusalsshould be identified and discussed.1.2.Pick an actual situation that occurred recently forthe client.Ask client to provide some background on thetarget person.63
Role-play: Drug-offer situationRole-play a situation where a drug userfriend (or dealer) makes an offer to give orget drugs. Role-play an ineffectiveresponse and role-play an effective use ofhow to say “No.”64
CBT Techniques forAddiction Treatment:Preventing theAbstinence ViolationEffect65
Abstinence Violation SyndromeIf a client slips and uses drugs after a period ofabstinence, one of two things can happen. He or she could think: “I made a mistake and now Ineed to work harder at getting sober.Or He or she could think: “This is hopeless, I will neverget sober and I might as well keep using.” Thisthinking represents the abstinence violation syndrome.66
Abstinence Violation Syndrome: Whatpeople say¾ One lapse means a total failure.¾ I’ve blown everything now! I may as well keep using.¾ I am responsible for all bad things.¾ I am hopeless.¾ Once a drunk / junkie, always a drunk / junkie.¾ I’m busted now, I’ll never get back to being straightagain.¾ I have no willpower I’ve lost all control.¾ I’m physically addicted to this stuff. I always will be.67
Preventing theAbstinence Violation SyndromeClients need to know that if they slip anduse drugs / alcohol, it does not mean thatthey will return to full-time addiction. Theclinician can help them “reframe” thedrug-use event and prevent a lapse inabstinence from turning into a full returnto addiction.68
Abstinence violation effect: Examplesof “reframing” (1)I used last night, but I had been sober for30 days before. So in the past 31 days, Ihave been sober for 30. That’s betterthan I have done for 10 years.69
Abstinence violation effect: Examplesof “reframing” (2)Learning to get sober is like riding abicycle. Mistakes will be made. It isimportant to get back up and keep trying.70
Abstinence violation effect: Examplesof “reframing” (3)Most people who eventually get sober dohave relapses on the way. I am notunique in having suffered a relapse, it’snot the end of the world.71
CBT Techniques forAddiction Treatment:Making LifestyleChanges72
Developing new non-drug-relatedbehaviours: Making lifestyle changes¾ CBT techniques to stop drug use must beaccompanied by instructions andencouragement to begin some new alternativeactivities.¾ Many clients have poor or non-existentrepertoires of drug-free activities.¾ Efforts to “shape and reinforce” attempts to trynew behaviours or return to previous non-drugrelated behaviour is part of CBT.73
?Questions?Comments?74
Thank you for your time!End of Workshop 275
Workshop 3: Methods forUsing Cognitive BehaviouralStrategies76
Training objectivesAt the end of this workshop, you will be able to:1. Understand the clinician’s role in CBT2. Structure a session3. Conduct a role-play establishing aclinician’s rapport with the client4. Schedule and construct a 24-hourbehavioural plan77
Role of the Clinician inCBT78
The clinician’s roleTo teach the client and coach her or himtowards learning new skills for behaviouralchange and self-control.79
The role of the clinician in CBT¾CBT is a very active form of counselling.¾A good CBT clinician is a teacher, acoach, a “guide” to recovery, a source ofreinforcement and support, and a sourceof corrective information.¾Effective CBT requires an empatheticclinician who can truly understand thedifficult challenges of addiction recovery.80
The role of the clinician in CBTThe CBT clinician has to strike a balancebetween: Being a good listener and asking goodquestions in order to understand the clientTeaching new information and skillsProviding direction and creating expectationsReinforcing small steps of progress andproviding support and hope in cases ofrelapse81
The role of the clinician in CBT¾¾The CBT clinician also has to balance: The need of the client to discuss issuesin his or her life that are important. The need of the clinician to teach newmaterial and review homework.The clinician has to be flexible todiscuss crises as they arise, but notallow every session to be a “crisismanagement session.”82
The role of the clinician in CBT¾The clinician is one of the most importantsources of positive reinforcement for theclient during treatment. It is essential forthe clinician to maintain a nonjudgemental and non-critical stance.¾Motivational interviewing skills areextremely valuable in the delivery of CBT.83
How to Conduct aCBT Session84
CBT sessionsCBT can be conducted in individual orgroup sessions.¾ Individual sessions allow more detailedanalysis and teaching with each clientdirectly.¾ Group sessions allow clients to learnfrom each other about the successful useof CBT techniques.¾85
How to structure a sessionThe sessions last around 60 minutes.86
How to organise a clinical session withCBT: The 20 / 20 / 20 rule¾¾¾CBT clinical sessions are highly structured,with the clinician assuming an active stance.60-minute sessions divided into three 20-minutesub-sessionsEmpathy and acceptance of client needs mustbe balanced with the responsibility to teach andcoach. Avoid being non-directive and passiveAvoid being rigid and machine-like87
First 20 minutes¾¾¾¾¾¾Set agenda for sessionFocus on understanding client’s current concerns(emotional, social, environmental, cognitive, physical)Focus on getting an understanding of client’s level ofgeneral functioningObtain detailed, day-by-day description of substanceuse since last session.Assess substance abuse, craving, and high-risksituations since last sessionReview and assess their experience with practiseexercise88
Second 20 minutes¾¾¾¾Introduce and discuss session topicRelate session topic to current concernsMake sure you are at the same level as clientand that the material and concepts areunderstoodPractise skills89
Final 20 minutes¾¾¾¾Explore client’s understanding of and reactionto the topicAssign practise exercise for next weekReview plans for the period ahead andanticipate potential high-risk situationsUse scheduling to create behavioural plan fornext time period90
Challenges for the clinician¾¾¾¾Difficulty staying focused if client wants tomove clinician to other issues20 / 20 / 20 rule, especially if homework has notbeen done. The clinician may have to problemsolve why homework has not been doneRefraining from conducting psychotherapyManaging the sessions in a flexible manner, sothe style does not become mechanistic91
Principles of UsingCBT92
Match material to client’s needs¾CBT is highly individualised¾Match the content, examples, and assignmentsto the specific needs of the client¾Pace delivery of material to insure that clientsunderstand concepts and are not bored withexcessive discussion¾Use specific examples provided by client toillustrate concepts93
Repetition¾Habits around drug use are deeply ingrained¾Learning new approaches to old situationsmay take several attempts¾Chronic drug use affects cognitive abilities,and clients’ memories are frequently poor¾Basic concepts should be repeated intreatment (e.g., client’s “triggers”)¾Repetition of whole sessions, or parts ofsessions, may be needed94
PractiseMastering a new skill requires time and practise.The learning process often requires makingmistakes, learning from mistakes, and tryingagain and again. It is critical that clients have theopportunity to try out new approaches.95
Give a clear rationaleClinicians should not expect a client topractise a skill or do a homework assignmentwithout understanding why it might behelpful.Clinicians should constantly stress theimportance of clients practising what theylearn outside of the counselling session andexplain the reasons for it.96
Activity 7: Script 1“It is very important that you give yourself a chance totry new skills outside our sessions so we can identifyand discuss any problems you might have puttingthem into practise. We’ve found, too, that people whotry to practise these things tend to do better intreatment. The practise exercises I’ll be giving you atthe end of each session will help you try out theseskills.”97
Communicate clearly in simple terms¾Use language that is compatible with theclient’s level of understanding andsophistication¾Check frequently with clients to be surethey understand a concept and that thematerial feels relevant to them98
MonitoringMonitoring: to follow-up by obtaininginformation on the client’s attempts topractise the assignments and checking ontask completion. It also entails discussingthe clients’ experience with the tasks sothat problems can be addressed in session.99
Praise approximationsClinicians should try to shape the client’sbehaviour by praising even small attemptsat working on assignments, highlightinganything that was helpful or interesting.100
Example of praising approximationsI did not work on myassignments sorry.Well Anna, you couldnot finish yourassignments but youcame for a secondsession. That is a greatdecision, Anna. I amvery proud of yourdecision! That was agreat choice!Oh, thanks!Yes, you are right. Iwill do my best toget all assignmentsdone by next week.101
Overcoming obstacles to homeworkassignmentsFailure to implement coping skills outsideof sessions may have a variety of meanings(e.g., feeling hopeless). By exploring thespecific nature of the client’s difficulty,clinicians can help them work through it.102
Example of overcoming obstaclesBut it wassomethingvery easy.I understand,Anna. How canwe make theassignmentseasier to completetomorrow?I could not do theassignments I am very busyand, besides, my children areat home now so I do not havetime .Well, I think that if Ijust start by doing oneor two days ofassignments nomore.103
What makes CBT ineffectiveBoth of the following two extremes ofclinician style make CBT ineffective: Non-directive, Overlypassive therapeutic approachdirective, mechanical approach104
Activity 6: Observe a role-play15 Min.Observe clinician A and clinician Bconducting a session with a client: How did they do in session?What would you do differently and why?105
Creating a DailyRecovery Plan106
Develop a plan (1)Establish a plan for completion of the nextsession’s homework assignment.107
Develop a plan (2)¾Many drug abusers do not plan out theirday. They simply do what they “feel likedoing.” This lack of a structured plan fortheir day makes them very vulnerable toencountering high-risk situations andbeing triggered to use drugs.¾To counteract this problem, it can beuseful for clients to create an hour-tohour schedule for their time.108
Develop a plan (3)¾Planning out a day in advance with a clientallows the CBT clinician to work with the clientcooperatively to maximise their time in low-risk,non-trigger situations and decrease their timein high-risk situations.¾If the client follows the schedule, they typicallywill not use drugs. If they fail to follow theschedule, they typically will use drugs.109
Develop a plan (4)A specific daily schedule:¾¾¾Enhances your client's self-efficacyProvides an opportunity to consider potentialobstaclesHelps in considering the likely outcomes ofeach change strategyNothing is more motivating than beingwell prepared!110
Stay on schedule, stay sober¾Encourage the client to stay on theschedule as the road map for stayingdrug-free. Staying on schedule Staying sober Ignoring the schedule Using drugs111
Develop a plan: Dealing withresistance to scheduling¾Clients might resist scheduling (“I’m not ascheduled person” or “In our culture, wedon’t plan our time”).¾Use modelling to teach the skill.¾Reinforce attempts to follow a schedule,recognizing perfection is not the goal.¾Over time, let the client take overresponsibility for the schedule.112
Activity 7: Exercise25 Min.Have pairs of participants sit togetherand practise the creation of a 24-hourbehavioural plan using the Daily /Hourly Schedule form.113
?Questions?Comments?114
Post-assessment10 Min.Please respond to the post-assessmentquestions in your workbook.(Your responses are strictly confidential.)115
Thank you for your time!End of Workshop 3116
1. Identify a minimum of 4 cognitive behavioural techniques 2. Understand how to identify triggers and high- and low-risk situations 3. Understand craving and techniques to cope with craving 4. Present and practise drug refusal skills 5. Understand the abstinence violation syndrome and how to explain it to clients 6.