Transcription
Comparing Leanand IHI Quality ImprovementRichard Scoville, PhDIHQI Speaker SeriesFebruary 9, 2015Richard Scoville, PhD Improvement Advisor for Institute for HealthcareImprovement Dentaquest Institute Cincinnati Children’s Hospital NHS UK Adjunct Associate Professor, Dept. HealthPolicy & Management, UNC Chapel Hill
ComparingLeanandQualityImprovement.aspx"Do not seek to follow in the footsteps of theold masters. Seek instead what the oldmasters sought."–Basho (1644-1694)
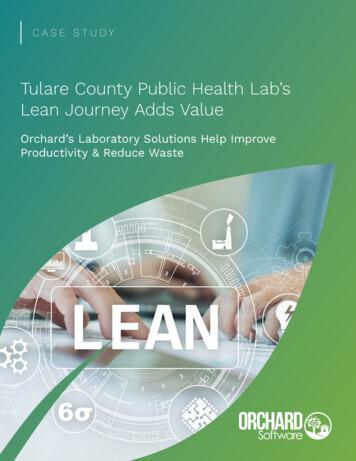
Knowledge for ImprovementSubject MatterKnowledge:Subject Matter KnowledgeKnowledge basic to thethings we do in life.Professional knowledge.ProfoundKnowledgeQI:Combining subjectmatter knowledge withimprovement scienceto develop effectivechanges.Improvement ScienceImprovement ScienceThe interaction of thetheories of systems,variation, knowledge, andpsychology.Some Healthcare QI MilestonesFrederick Taylor Experiments in workplace Process analysis, measurement Top-down design: unskilled labor Japanese trainees visit U.S.Henry Ford Assembly line Standard product Vertical integrationJoseph Juran Student of Shewhart Quality as a system ofmanagement Lectures to JUSE 1954Walter Shewhart At Western Electric Statistical process control PDSA cycle190019101920Don Berwick founds IHI Curing Healthcare 1989 API: Tom Nolan, LloydProvost are QI mentorsEdwards Deming Student of Shewhart Statistician/ mathematician SPC lectures in Japan 195019301940Kiichiro Toyoda Toyota Motors founded 193719501960Ford Motors Invests in SPC1980s, Mazda Lean LessonsDeming Consults in U.S. API Principals are students TV show 19801970Shigeo Shingo TPS rapid turnoverTaiichi Ohno Toyota Production System 1950s-70s Kanban, andon, JIT, ‘pull’, Kaizen Workers solve problems198019902000Virginia Mason, Seattle Adopts Lean methods ‘Virginia Mason ProductionSystem 2000Womack et al. Machine That Changed The World 1990
Profound Knowledge“A system cannot understand itself. [That] requires a viewfrom outside – a lens – that I call a system of tionDomains of Profound Knowledge Appreciation of a System“System” an interdependent group of items, people or processes workingtogether to a common purpose. PsychologyHow do people respond to change? How can we encourage constructivechange and commitment to excellence? How does human perception anddecision making shape process design? Understanding VariationHow should we interpret and respond to the variation that continuallyoccurs in every system? Theory of KnowledgeHow can we learn to predict the impact of planned changes? How can wedevelop sustainable changes that will lead to improvement?
Appreciation of a SystemA system is an interdependent group of items, people orprocesses working together to a common purpose.“Every system isperfectly designed toachieve the resultsthat it gets.”- Paul BataldenSystemsPhysical systemsSocial networksFunctional systems(processes)
Sizing the SystemSource: Commonwealth Fund
5S5S seiri, seiton, seiso, seiketsu, shitsuke(sort, straighten, shine, standardize, sustain)Where Do We Lay the ing4.asp
Understanding VariationVariability is an inherent characteristic of any system. Measures and data areuseful to guide future action, provided we can discern patterns in such variationand respond appropriately A key distinction [is] between common causevariation produced by a stable, predictable process and special cause variationthat results either from unstandardized, uncontrolled operations or from intentionalprocess changes.“Variation is a thief The enemy is notconsidered, intentional variation, butrather unintended or misinterpretedvariation.”- Don Berwick“Management is prediction!”- W. Edwards Deming
Schechter, M. S. and P. Margolis (2005). "Improving subspecialty healthcare: lessons from cysticfibrosis." J Pediatr 147(3): 295-301.Schechter, M. S. and P. Margolis (2005). "Improving subspecialty healthcare: lessons from cysticfibrosis." J Pediatr 147(3): 295-301.
Improvement is TemporalPercent of ER patients with Chest Pain Seen by aCardiologist within 10 minDid we improve?What will happen next?Should we do something?Source: R. LloydDid We Improve?Percent of ER patients with Chest Pain Seen by aCardiologist within 10 min100%Changehere95%90%85%80%75%70%65%60%55%What will happen next?Source: R. LloydShould we do something?3/5/20083/19/20082/6/2008Did we 00750%
Run ChartsMedian2/5 Project Start2/6 New datasystem, nodata available2/12 Visualcontrol for patientflow8/6 New triageprocedureIndividualmeasurevaluesTime-Ordered DataRun ChartsNonparametric rules for significant change (p .05):Shift – 6 or more consecutive points above or below the medianTrend – 5 or more consecutively increasing or decreasing pointsAstronomical Point – A dramatically different valueRuns – Too many or too few runs if only by chance
Shewhart Control Chart3-sigma controllimitsMeanPercent of Patients with Pressure Ulcers100%90%80%70%60%50%40%30%20%10%0%123456789 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28WeekSubgroup (1 or moreobservations)Shewhart Control ChartPercent of Patients with Pressure Ulcers100%90%?80%70%60%50%40%30%20%10%0%123456789 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28WeekTests for special cause- One data point that falls outside the limits- Eight or more consecutive subgroups above or below the mean- Six points all going up or all going down.- Two out of three consecutive points in either outer third of the limits.
PsychologyPsychology deals with the behavior of humans as social actors, theirinteractions with one another, and their interactions with the systems ofwhich they are a part.“First we build people,then we build cars.”- Toyota saying“Drive out fear.”- W. Edwards Deming“Doh!”- Homer SimpsonHomo Economicus? Who are we really?Are we rational actors whoevaluate options carefully anddispassionately?Or are our actions driven byappetites, reflexes, and faultylogic?
Adhere to Best Practice?%10080%YESDo you use lung protective strategy Inventilating acute lung injury patients?8060Results of A Level 1Reliability Processes.4020The Gap between Perception and Practice ofSepsis Therapy. FM Brunkhorst et al. for theGerman Competence Network Sepsis –Crit Care Med 2008;36(10):2719-25.Audit2.6%0Slide courtesy of Terry Clemmer, MD“Of course we do it every iewAuditSlide courtesy of Terry Clemmer, MDThe Gap between Perception andPractice of Sepsis Therapy. FMBrunkhorst et al. for the GermanCompetence Network Sepsis – Crit CareMed 2008;36(10):2719-25.
‘Heuristics’ Anchoring‘Manufacturers suggested retail price’ AvailabilityHigh salience events over-predicted RepresentativenessPatterns, patterns everywhere OptimismAll the children are above average Loss AversionLosing is worse than not winning Status Quo PreferenceThaler, R. and C. Sunstein (2008). Nudge.New York, Penguin.The ‘whatever’ principle The Herd Instinct‘Everybody’s doing it!’A Choice Architecturehttp://www.youtube.com/watch?v 2lXh2n0aPyw
‘Culture’Culture BeliefsIdeas and values that the group accepts as ‘selfevident’, ‘reasonable’, ‘right’, ‘just’, etc. RitualsThings we do together: work, play, worship, etc. NormsWhat’s right? cool? polite? bad? pitiable?disgusting? etc.To change culture, change behavior; the rest will follow.An Effective Improvement Culture Requires Transparency!P39
Principles from Social PsychologyAsch: “Collective Conservatism” People are likely to conform when theyknow that other people will observe whatthey have to say Newly formed groups establish beliefs andnorms quicklyGilovich: “Spotlight Effect” We tend to believe that others areattending to and care about what we do orbelieveAsch, S. E. (1955). "Opinions and Social Pressure." Scientific American 193(5): 31-35.Gilovich, T., V. Medvec, et al. (2000). "The spotlight effect in social judgment." Journal of Personality and SocialPsychology 78(2): 211-222.Lots of Advice Out There
One Actually Worth ReadingTheory of KnowledgeThe development of practical knowledge of “what works,” grounded inpredictions about the results to be achieved through system changes.Knowledge is gained through a process of stating a theory, making aprediction based on the theory, comparing observations with predictions,and revising or abandoning the theory accordingly.“If you don’t try,you’ll never know”
The Model for Improvement“A heuristic for learning from experience and guiding purposeful action.”The Model for Improvement What it’s NOT: The (entire) IHI-QI approach toimprovement A project plan Engineering A ‘toolkit’ A collaborative What is IS:“A heuristic for learning from experience andguiding purposeful action.” At all levels of scale.
“An algorithm for achieving an aim at any scale”IHI-QI
Conceptual FrameworksComplex adaptivesystemsSystemMultidisciplinary teamsDecision theoryLeadershipPsychologyDiffusion of innovationSocial network theoryTheories ofmotivationReliability theoryMeasurementProgram EvaluationRegressionOperational definitionsModel for improvementLearningGraphical displays ofdataStatistical process controlVariationDesign of experimentsTools and MethodsValue stream mapSystem diagramDriver diagramSDIDirected creativitySystemPsychologyRCA‘Leading Change’SituationalAwarenessGemba walkSocial networkdiagramsKaizen eventControl chartsDevelop-testimplement sequenceBTS collaborativesRun chartsLearningPDSA FormsA3 planningVariationPareto chartsHistograms
Projects"All Improvement Takes Place Project by Project. There isno such thing as improvement generally. All improvementtakes place project by project and in no other way.As used here, “improvement project” means “a chronicproblem scheduled for solution.” Since improvement projecthas multiple meanings, the company glossary and trainingmanuals shoulddefine it.“–Joseph Juran - HandbookPlanning – Improvement - Control
BTS Collaborative: A Learning ModelKEYSelect topic andtarget system,populationLS Learning SessionAP Action PeriodPlanning & PreparationIdentify subjectmatter &improvementexpertsto support teamsSpread ActivityBaselinedataEngage localpartnersAP1AP2AP3AP4Expert MeetingProgrammedesign includingspread luate,Publish,Organizematerial forfuture projectssupport– site visits, phone calls, webniars,engagement of supervisory managers, facultyfeedback, data interpretation, IT support, etc.12 – 18 months“Without theory, there are no questions;without questions, there is no learning.”- W. Edwards Deming“Avoid going through the motions.”- Xi Jinping
Content TheoryOutcomesPrimary DriversSecondary DriversP1 The system of carereliably identifies patientswith advanced illnessPatients of the NSLIJsystem with advancedillness reliably receivecare that Is trustworthy Aligns with their needs &preferences Avoids unneeded orundesired tests andtreatments Engages with patientsand families as respectedpartners in care Encourages patient andfamily responsibility(1)Reliable process for early identification ofpatients with advanced illness via standardcriteriaProviders educated and selectedfor ConversationsCommunity awareness encourages earlyself-identification, use of advanced directivesP2 Informed patientpreferences and hopes areunderstood by families andcliniciansP3 Services align withpatients’ needs andpreferences: accessible,appropriate, respectful,coordinated across timeand placeMeasure Concepts: Patient/family satisfaction ICU days in last X monthsof life Acute admissions in last Xmonths of life: # & LOS Cost of care in last Xmonths (to payer, system,and family)ChangesTrigger: Norton, The ‘Surprise’question, multiplehospitalizations), AIM criteriaPartner with community agenciesfor awareness programs &recruitmentInformed, recurring Conversations (2) occurat critical times (starting early) and includekey elementsElements & structure ofConversations: e.g. ‘PresenceListening- Planning- Guidance cyclePreferences are reliably documented andcommunicated multiple waysAdvanced directives, personalhealth records, electronic sharingwhere feasibleCare is provided by identified (3)interdisciplinary team, with ‘navigator’ or caremanager for pt/fam, and PCP ‘in driversseat’Intentional team set up with teamroles clarified and physiciancontrol respected per pt. wishHome /family caregivers are assessed andsupportedProcess to assemble individualcare team and communicate topt/famSupports include:Team provides curative and palliative careCare is continuous across settings, mediatedthrough shared information ( both manual andInformation Technology platform)Version 8/13/2013 Notes (n) in slide notesP4 Financial and paymentarrangements support theaimCall center; clinician/ sw cellphoneServices, advice and facilities available topatients for appropriate care 24/7Business models are explicit and includesupporting care and services outside thehospitalChronic Care ModelHealth SystemCommunityResources and ientHealth Care red,ProactivePractice TeamFunctional and Clinical Outcomes
ECC Phase III – Execution TheoryAIM: Reduce incidence of caries, pain & referrals by participating practices through application of disease management model. Develop content for campaign to follow.External Context Phase 1 and 2 ECCprojects demonstratefeasibility; continuingfaculty Team experience withprior data proceduresand measures (ECC 2) Aggregator prototype(EDD) Anticipated changes inreimbursement policiesprovide motivation forteam participation National interest bydental in medicaldisease managementmodels driveparticipation Evolving dentalprotocols re prevention,disease management(CHB protocols) Moral imperative resafety net population Private practicepayment model resistsDM approaches Evolving roles of dentalproviders: team basedcareInputsInterventionsCollaborative teams : Senior leadership &alignment with org goals QI Team Lead Clinical champion Measurement processfor data entry, review, anduse Experienced teams fromECC2/EDD Will to change! Dedicated time for QIteam EDR; Aggregatorinstallation, coding No ‘crises’ in playStandard BTS components Prework, baselinemeasurement, orientationcalls, application process Learning sessions (inperson/virtual) AP calls Monthly reports, PDSA logs,reviews, data feedback Virtual discussions viaBasecampBTS enhancements Coaches monthly contact Measure help desk Site visits Bi weekly summaryDQI Team Experienced faculty fromprior initiatives Experienced projectteam; broad skills NICHQ projectmanagement DQI funding to supportfaculty & teams Coaches from ECC2Training for Teams –sequenced based on driverdifficulty MFI – standard Motivational interviewing Process analysis & reliability Clinical protocol & scienceMaterials Driver diagram with highdegree of confidence Project charter, changepackage, other technicalsupport documents Measurement plan DQI resources:- Online Learning Center- Collaborativeinfrastructure (list, Webex,Basecamp, etc)- Aggregator, programmerOperational strategies Vanguard team Directed storyboard contentat LS Videos to teach MI Team-authored video withfeedback Measure cheat sheet,coaching on data Coaches modelimprovement, provide 1st pointof contactPredictions /Mechanisms(K2) ImmediateOutcomes Prework & applicationensures team readiness &self-selection Test feasibility of virtualLSs LS transfer QI skill,motivate teams; AP callssustain involvementbetween LSs Team feedback provideguidance and ideas,motivates teams, modelsuse of data forimprovement Enhancements provideindividual team support,esp. for ‘stuck’ teams Driver sequence helpsteams develop effectiveskills, motivation Site visits help DQI teamunderstand team &collaborative issues,including ‘received’ content Coaches provide realworld experience, closerelationship (predications foroperational strategies) Frequent faculty contactsencourages consistentmessaging, keeps facultyinformed.Team Activity Storyboards, AP callpresentations Attendance &participation on calls, LSs Process & outcome datareporting PDSA activity reportedvia PDSA logs & monthlyreports Coach engagement Compliance withassigned work products(K3) Behavior Changes Culture of transparency Generalized application of MFI Reliable enactment of DMprotocol Routine use of data forpopulation management, QItracking, PDSA Team based care models Adherence to DMprotocolTesting and ProcessImprovement MFI understood andused appropriately Aggregator and neededcodes established & usedreliably Teams test & implement& spread appropriately(K4) Long Term Impact Increase in % with reduced risk Decrease in new cavitation by50% Decrease in pain by 30% Decrease referrals by 50% Development of QI capacity withDQI/SNS Provide materials and methodsto inform future initiatives.Project team developmentand oversight, huddles,faculty calls, coaching mentorcalls, team lead callsAssumptions Current delivery, policy & reimbursement models will be restructured.2/10/2015 56Figure A.1 Complete List of Change .35.36.Eliminate things that are not usedEliminate multiple entryReduce or eliminate overkillReduce controls on the systemRecycle or reuseUse substitutionReduce classificationsRemove intermediariesMatch the amount to the needUse SamplingChange targets or set pointsSynchronizeSchedule into multiple processesMinimize handoffsMove steps in the process close togetherFind and remove bottlenecksUs automationSmooth workflowDo tasks in parallelConsider people as in the same systemUse multiple processing unitsAdjust to peak demandMatch inventory to predicted demandUse pull systemsReduce choice of featuresReduce multiple brands of the same itemGive people access to informationUse proper measurementsTake Care of basicsReduce de-motivating aspects of pay systemConduct trainingImplement cross-trainingInvest more resources in improvementFocus on core process and purposeShare risksEmphasize natural and logical 6.67.68.69.70.71.72.Develop alliances/cooperative relationshipsListen to customersCoach customer to use product/serviceFocus on the outcome to a customerUse a coordinatorReach agreement on expectationsChangeOutsource for “Free”conceptsOptimize level of inspectionWork with supplierscompatibleReduce setup or startup timewith LeanSet up timing to use discountsOptimize maintenanceproductionExtend specialist’s timeReduce wait timeStandardization (Create a Formal Process)Stop tamperingDevelop operation definitionsImprove predictionsDevelop contingency plansSort product into gradesSource: The Improvement Guide p. 359DesensitizeExploit variationUse remindersUse differentiationUse constraintsUse affordancesMass customizeOffer product/service anytimeOffer product/service anyplaceEmphasize intangiblesInfluence or take advantage of fashion trendsReduce the number of componentsDisguise defects or problemsDifferentiate product using quality dimensionsChange the order of process stepsManage uncertainty, not tasks
North Shore LongIsland Jewish –Reducing SepsisMortalityPrimaryDriversSecondary DriversTeam roles and personnel are clearly defined,understood, and trusted by all participantsStaff recognize and prioritize patient needs, andappreciate importance of timely sepsis responseWell structured,committed, highfunctioning clinical teamsTeams transparently and immediately share processdefects, ideas for change, and outcome metricsStandard methods for onboarding new personnelA fundamental assumption ofclinical QI:Reliable execution of keyclinical driver processesimproves outcomes measuredat the population levelTimely, sensitive & specific recognition of sepsis andsevere sepsisOutcomesReduce mortality amongpatients with severesepsis/shock by 50%system wide in 5 yearsReliable identification ofsepsis and execution ofsepsis protocolsExplicit standard process is ‘ready to go’ when sepsis isdiagnosedRequired clinical personnel are available and ready torespond, including required escalation of careTimely MD engagement and ordersTimely & effective communication & handoffs: ED to Floor& ICU, Floor to ICU, ICU to floorSr leadership aligns incentives and strategy to focus onsepsis care & mortality reductionVigorous and effectiveleadershipSr and mid-level leaders regularly review results, allocateresources, activate improvementProvide feedback on performance; continue to emphasizeimportance of sepsis careRev. 5/3/2013Organizationalinfrastructure supportseffective sepsis careEfficient, timely data collection and reporting of key sepsisprocess metrics (KQMI)System wide change management support for front lineteams (CLI)Support processes respond in a timely fashion: Lab,Pharmacy, supply chain & support servicesReliability Of Evidence-Based Care McGlynn, et al: ‘The quality of health caredelivered to adults in the United States’. NEJM2003; 348:2635-2645 439 indicators of clinical quality of care 30 acute and chronic conditions, plus prevention Medical records for 6712 patients Participants received 54.9% of scientifically indicatedcare (Acute: 54%; Chronic: 56%; Preventive: 55%) The “defect rate” in the quality of Americanhealth care is approximately 45%
Getting Consistent, at Scale in SystemsWhat Can Go Wrong in a Process?Problems inhand-offbetween stepsProblems inexecution withinstepsSource: Peter Margolis, CCHMC; Moira Inkelas, UCLAEvery Step CountsHow many people get what they need from aprocess that has multiple steps – if there is 90%reliability in each step?90%90%90%90%Source: Peter Margolis, CCHMC; Moira Inkelas, UCLA66%
Staph aureus (SA)Screening and Decolonization Process ExampleScheduling1-4 weeks pre-procedure2-3 weeks pre-procedureInsert labrequest for SAcultureScheduleprocedureYesInform patientof SAscreeningTKA orTHA?Day of surgery99%90%NoPt presents fornasal swabLab90%100%Processspecimen99%Results tosurgeon &hospitalNotify hospital(90%)NoPositivefor SA?Yes(10%)85%Contact patient100%Prescribe 5day mupirocin99%Hospital/Surgeon75%Confirm RxcompleteKEY RELIABILITY MEASURE50%% of colonized patients with completedRxSource: IHI Project JointsDocument inrecordSurgeryBuilding BeliefPDSPASDAPDChangePAChange ideas,suggestions, PPAADPSSAATests increase inscope and scale.Learning from dataSSystem changesthat will result inimprovement
Process Change: Scale Up & SpreadConfidence that change is effectiveEmbed in dailyoperationsTest under avariety ofconditionsPrerequisitesfor changeSpreadthroughout thesystemImplement achangePilot /prototypea changeDevelop achangeIHI-QI Roadmap Plan the Initiative Content Theory and Aim Execution Theory and Plan Develop, test, and pilot changesImplement, sustain and controlSpread throughout the SystemEvaluate results and ‘pass forward’
LeanLean Enterprise InstituteWhat is ‘Value?’ - the Lean Ideal The output is defect free. The product or service is delivered in response tocustomer need (pull, on demand). The response is immediate. Products or services are provided 1x1 in the unit sizeof use [i.e. tailored to the identified needs of theconsumer –the authors]. Work is done without waste. Work is done safely. Work is done securely.Spear, S. and H. K. Bowen (1999). "Decoding the DNA of the ToyotaProduction System." Harvard Business Review 77(5): 96-106.
Two SystemsDeming: “By what means” the ideal? Production System Management SystemThe Production SystemTwo fundamental operating principles toachieve the ideal Jidoka: Highlight and visualize problems--stopwhen defects are detected, continuousinspection at all levels. Just In Time: each process produces only whatis needed by the next process in a y/vision philosophy/toyota production system/
Concepts To Support Lean Production Value versus waste Kaizen Value stream: Production stream: customer desire production consumption Information flows to control production A few Lean change conceptsstandard work flow load leveling poke-yoke kanban andon visual controlValue Stream Map of Current State: PhlebotomySource: AHRQ Publication # 05-0108-EF
Waste ‘Negative Value’Source: Virginia Mason Health SystemLean Production RoadmapWomack and Jones (1996), Lean Thinking, Simon & Schuster: New York
Management SystemIdeal management system to support valuebased production: Leader standard work Visual controls Daily accountability and planning Respect for people who do the work Unity of purposeMann, D. (2010). Creating a Lean Culture: Tools to sustain leanconversions. Boca Raton, FL, CRC Press.Source: Virginia Mason Health System
Source: Virginia Mason Health SystemStandard Work for ManagersManagers have standard work processes, primary role as coaches forfront line staff. Improvement is integrated with standard work.Source: John Toussaint, Thedacare
Daily ManagementSource: Virginia Mason Health SystemLean System Deployment – Road MapLong Term CycleAdopt SystemsParadigm Build vision Convey urgency Make theCommitment Obtain Sr. MgmtBuy-inDesign Processes Map ProcessesInternalize VisionSet Goals & MetricsIdentify StakeholdersDetailedVisionBuild Lean Cultiure and Behavior Organize for Implementation Identify & Empower ChangeAgents Align Incentives Adapt Structure & Systems Short Term CycleDecision to PursueLean ApproachOrganizationalStrategyManage Quality Monitor Progress Refine the Plan Capture, Adopt New KnowledgeCreate /Refine Plan Identify & Prioritize Activities Commit Resources Provide Education & TrainingImprove Quality Develop Detailed Plans Implement QI ActivitiesSource: Rohit Ramaswamy, Adapted from MIT Lean Aerospace Institute
For IHI-QI, What is Lean?“Lean is, in a sense, a complex and deep‘application’ of Profound Knowledge, a particulardeployment of improvement in the realm ofproduction systems The TPS package ofinterdependent change concepts represents a‘template’ for improving [production] systems,with a set of predefined aims, change concepts,implementation roadmap, and tools.”Scoville & Little 2014 - Comparing Lean and QI p. 18Key Similarities Purpose of the system guidesimprovement: Aim / Value Change Concepts Continuous Quality Improvement at thefront line Simplified heuristic for problem solving:MFI, A3 Shared tools & methods Measured feedback Emphasis on analytical, blame-free culture
Key Differences of Emphasis Blank slate? IHI-QI: Theory drives aims; eclecticism Lean: Aims based on lean ‘ideal’ Organizing for improvement IHI-QI: Improvement based in projects Lean: Improvement focuses on daily production andmanagement standard work Approach to reducing variation(‘what do we think of first?”) IHI-QI: SPC, distinguish common from special causes Lean: Standardized work with kaizen Role of leaders IHI-QI: Sponsors, resources, accountability Lean: Coaching, standard work, accountabilityComplementary BenefitsIHI-QI Go to gemba “Bring theimprovement initiativeto the workplace” Management systemimprovement isessential forsustainable resultsLean Key concepts (e.g.“value”, “flow”) mustadapt to healthcare. Diverse conceptualframeworks offervaluable changeconcepts for Leanhealthcare Project formats as amethod for Leandeployment
Waste ‘Negative Value’Dimensions of Care ValueSafeEffectiveEfficientTimelyPt CenteredEquitable?Wasteful Health CareUnsafeIneffective Care that causes harm Infections Falls and injuries Care that does notconform to protocol Unnecessary care Insufficient careUntimelyInefficient Waiting for information Scheduling problems Idle time for people,equipment6HealthcareWastesInequitable Care based on abilityto pay Care is based onethnicity, language,culture Unnecessary tests,procedure Unnecessary transportor motion Inspection Reports that are not used ReadmissionsNot-Pt-Centered Disrespectful Patient not informed Families not included Unwanted care
The Model for Improvement“Deploy a Lean production system inour multi-site health care system.”Sustained adoption of Leanproduction and managementsystemsImprovement in process, outcomemetricsUse a BTS collaborative formatfocused on process flow,management systemQuestions R. Scoville 89
Virginia Mason, Seattle Adopts Lean methods 'Virginia Mason Production System 2000 Deming Consults in U.S. API Principals are students TV show 1980 Don Berwick founds IHI Curing Healthcare 1989 API: Tom Nolan, Lloyd Provost are QI mentors 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 Some Healthcare QI Milestones