Transcription
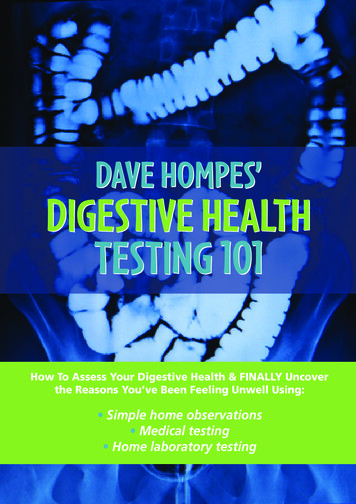
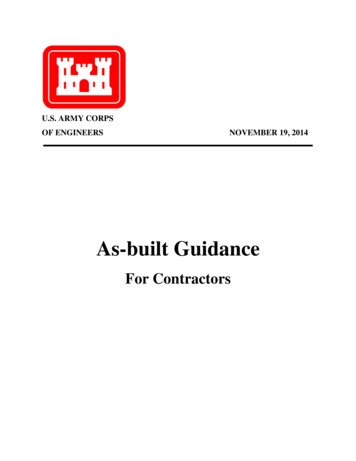
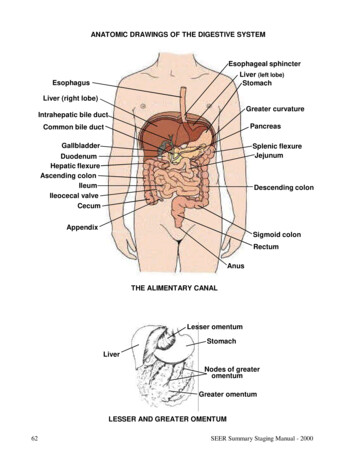
ANATOMIC DRAWINGS OF THE DIGESTIVE SYSTEMEsophageal sphincterLiver (left lobe)StomachEsophagusLiver (right lobe)Greater curvatureIntrahepatic bile ductPancreasCommon bile ductGallbladderSplenic flexureJejunumDuodenumHepatic flexureAscending colonIleumIleocecal valveCecumDescending colonAppendixSigmoid colonRectumAnusTHE ALIMENTARY CANALLesser omentumStomachLiverNodes of greateromentumGreater omentumLESSER AND GREATER OMENTUM62SEER Summary Staging Manual - 2000
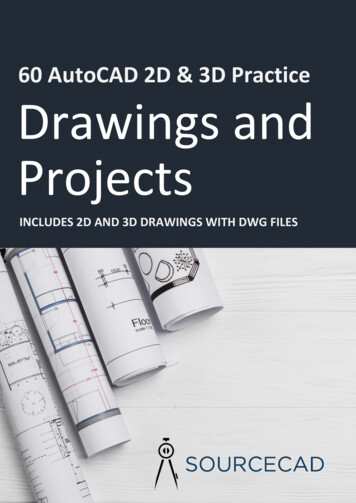
ANATOMIC DRAWINGS OF THE DIGESTIVE SYSTEMTransverse colonHepatic flexureSplenic flexureAscending colon(“right colon”)Descending colon(“left colon”)RectumSmall intestines:(duodenum, jejunum,and ileum)AnusTHE INTESTINESSEER Summary Staging Manual - 200063
DIGESTIVE SYSTEM SITESTABLE OF ANATOMIC STRUCTURESPRIMARY SITESUBMUCOSAMUCOSAEpitheliumEsophagus(C15. )YesSUBOUTSIDE THEMUSCU- SEROSALSEROSA 3LARIS TISSUES1 SEROSA 2Lamina MuscularisPropriaBYesYesYesYesSee note 4.NoSee note 4.YesYesYesYesNoYesGreater andlesser omentumYesYesYesYesNoYesMesentery ofsmall intestineAStomach(C16. )YesSESm. Intestine(C17. )YesColon (C18. )YesEYesYesYesYes.0 CecumYesNYesYesYesYesYes.1 AppendixYesYesYesYesYesYes.2 AscendingYesT:MYesYesYesYesNo.3 Hepatic fle x.YesEYesYesYesYesYes.4 TransverseYesMYesYesYesYesYes.5 Splenic flex.YesBYesYesYesYesYes.6 DescendingYesRYesYesYesYesNo.7 SigmoidYesAYesYesYesYesYes.8 OverlappingYesNYesYesYesYes.9 Colon, NOSYesEYesYesYesYesMYes::Yes::Yes::See note 5.:Mesenteric orYespericolic fat:Yes::Yes::See note Mesenteric orpericolic/perirectal fatRectumYesYesYesYesYesNoNoSee note 6.(C20.9)12345664Subserosal tissues include fat and flesh between the muscularis and the serosa.Serosa is also called mesothelium and visceral peritoneum. For the stomach and small intestine, serosa is alsoreferred to as tunica serosa. The term “serosa” is sometimes generically used to include both the serosa and thesubserosa, and therefore, the clinician should be consulted to determine if the use of “serosa” includes thesubserosa also.Mesenteric fat is also called pericolic fat.The tissue outside the muscularis of the esophagus is composed of fibrous connective tissue and referred to asadventitia.Anterior and/or medial aspects, but not lateral.Referred to as perirectal tissue.SEER Summary Staging Manual - 2000
DISTINGUISHING “IN SITU” AND “LOCALIZED” TUMORS FOR THE DIGESTIVE SYSTEMCareful attention must be given to the use of the term “confined to mucosa” for the esophagus, stomach,small intestine, colon and rectum.Historically, carcinomas described as “confined to mucosa” have been coded as localized. In order toprovide greater specificity and to rule out the possibility of classifying noninvasive tumors in this category,abstractors should determine:1) if the tumor is confined to the epithelium, in which case it is in situ, OR2) if the tumor has penetrated the basement membrane to invade the lamina propria, in whichcase it is localized and is coded to invasion of the lamina propria.The mucosa of the digestive tract consists of:The EPITHELIAL LAYER borders on the lumen. It contains no blood vessels or lymphatics.The BASEMENT MEMBRANE, a sheet of extracellular material, functions as a filtrationbarrier and a boundary involved in generating and maintaining tissue structure.The LAMINA PROPRIA, composed of areolar connective tissue, contains blood vessels,nerves, and, in some regions, glands. Once tumor has broken through the basement membrane into the lamina propria, it can spread by way of the lymphatics and blood vessels toother parts of the body.The MUSCULARIS MUCOSAE is a thin layer of smooth muscle fibers. It is found in thewall of the digestive tract from the esophagus to the anal canal.The SUBMUCOSA is a thick layer of either dense or areolar connective tissue. It containsblood vessels, lymphatic vessels, nerves, and, in some regions, glands.The MUSCULARIS PROPRIA is a double layer of muscle tissue in most of the digestivetract; it constitutes the wall of the organ.The SEROSA, the outermost layer covering most of the digestive tract, is a single layer ofsquamous epithelial cells, part of the visceral peritoneum. Just inside the serosa (mesothelium), and sometimes considered part of the serosa, is a layer of connective tissue called thesubserosa. The serosa and subserosa are present only in the peritonealized portions of thedigestive tract. For the esophagus and in the rectum below the peritoneal reflection, there isno serosa. For the esophagus, the connective tissue of surrounding structures merges with theconnective tissue of the esophagus and is called ADVENTITIA.SEER Summary Staging Manual - 200065
66SEER Summary Staging Manual - 2000
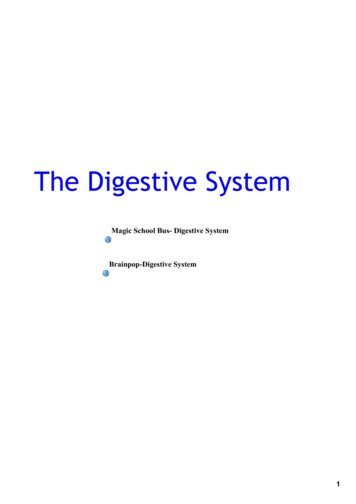
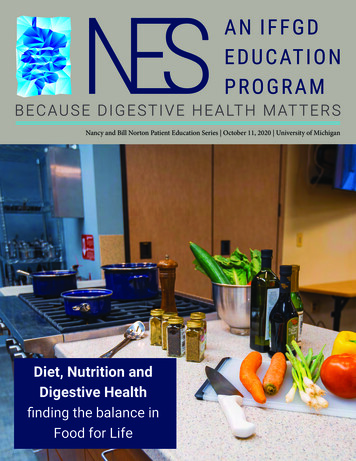
ANATOMIC DRAWINGS OF THE ESOPHAGUSMucosaSubmucosaCircular MuscleLongitudinal MuscleMuscularisAdventitiaCROSS SECTION OF ESOPHAGUSIncisorsCervical esophagusUpper 1/3(proximal)Middle 1/3Upper thoracic esophagusMid thoracic esophagusDiaphragmLower1/3(distal)Lower thoracic esophagusAbdominal esophagusCardioesophagealjunctionTHE ESOPHAGUSSEER Summary Staging Manual - 200067
ESOPHAGUSC15.0-C15.5, C15.8-C15.9C15.0 Cervical esophagusC15.1 Thoracic esophagusC15.2 Abdominal esophagusC15.3 Upper third of esophagusC15.4 Middle third of esophagusC15.5 Lower third of esophagusC15.8 Overlapping lesion of esophagusC15.9 Esophagus, NOSAnatomic Limits of Esophagus:CERVICAL ESOPHAGUS (C15.0): From the lower border of the cricoid cartilage to the thoracic inlet(suprasternal notch), about 18 cm from the incisors.INTRATHORACIC (including ABDOMINAL) ESOPHAGUS (C15.1-C15.5):Upper thoracic portion (C15.3): From the thoracic inlet to the level of the tracheal bifurcation (18-24 cm)Mid-thoracic portion (C15.4): From the tracheal bifurcation midway to the gastroesophageal (GE) junction (24-32 cm).Lower thoracic portion (C15.5): From midway between the tracheal bifurcation and the gastroesophagealjunction to the GE junction, including the abdominal esophagus (C15.2) between 32-40 cm.SUMMARY STAGE0 In situ: Noninvasive; intraepithelial1 Localized onlyInvasive tumor confined to:Intramucosa, NOSLamina propriaMucosa, NOSMuscularis mucosaeMuscularis propria invadedSubmucosaLocalized, NOS68SEER Summary Staging Manual - 2000
ESOPHAGUSC15.0-C15.5, C15.8-C15.92 Regional by direct extension onlyAdventitia and/or soft tissue invadedEsophagus is described as “FIXED”Extension to:Cervical esophagus (including first 18 cm of upper esophagus):Blood vessel(s) (major):Carotid arteryJugular veinSubclavian arteryCarinaCervical vertebra(e)HypopharynxLarynxTracheaThyroid glandIntrathoracic:Lung via bronchusMediastinal structure(s)PleuraRib(s)Thoracic vertebra(e)Intrathoracic, upper or mid-portion, esophagus:Blood vessel(s) (major):AortaAzygos veinPulmonary artery/veinVena cavaCarinaDiaphragmMain stem bronchusTracheaIntrathoracic, lower portion (abdominal), esophagus:Blood vessel(s) (major):AortaGastric artery/veinVena cavaDiaphragmStomach, cardia (via serosa)Continued on next pageSEER Summary Staging Manual - 200069
ESOPHAGUSC15.0-C15.5, C15.8-C15.93 Regional lymph node(s) involved onlyREGIONAL Lymph Nodes (including contralateral or bilateral)Cervical only:Cervical, NOS:Anterior deep cervical (laterotracheal) (recurrent laryngeal)Internal jugular, NOS:Deep cervical, NOS:Upper, NOS:Jugulodigastric (subdigastric)Peri-/paraesophagealScalene (inferior deep cervical)###***Supraclavicular (transverse cervical)###***Intrathoracic, upper thoracic or middle, only:Internal jugular, NOS:Deep cervical, NOS:Lower, NOS:Jugulo-omohyoid (supraomohyoid)MiddleUpper, NOS:Jugulodigastric (subdigastric)Intrabronchial:Carinal (tracheobronchial) (tracheal bifurcation)Hilar (bronchopulmonary) (proximal lobar) (pulmonary root)PeritrachealLeft gastric (superior gastric):###Cardiac (cardial)Lesser curvaturePerigastric, NOSPeri-/paraesophagealPosterior mediastinal (tracheoesophageal)###Superior mediastinal###***Intrathoracic, lower (abdominal), only:Left gastric (superior gastric):Cardiac (cardial)Lesser curvaturePerigastric, NOSPeri-/paraesophagealPosterior mediastinal (tracheoesophageal)Regional lymph node(s), NOS70SEER Summary Staging Manual - 2000
ESOPHAGUSC15.0-C15.5, C15.8-C15.94 Regional by BOTH direct extension AND regional lymph node(s) involvedCodes (2) (3)5 Regional, NOS7 Distant site(s)/lymph node(s) involvedAdjacent structures:Cervical/upper esophagus:LungMain stem bronchusPleuraThoracic/middle esophagus:Pericardium**Abdominal/lower esophagus:Diaphragm fixedDistant lymph node(s):Celiac for intrathoracic esophagusCervical, NOS for intrathoracic esophagusPara-aortic for lower/abdominal esophagus onlyScalene (inferior deep cervical) for intrathoracic esophagus onlySuperior mediastinal for cervical esophagus onlySupraclavicular (transverse cervical node) for intrathoracic onlyOther distant lymph node(s)Further contiguous extensionMetastasis9 Unknown if extension or metastasisNote: Ignore intraluminal extension to adjacent segment(s) of esophagus or to cardia of stomach and code depth of invasion orextra-esophageal spread as indicated.### Considered distant in Historic Stage** Considered regional in 1977 Summary Staging Guide*** Considered distant in 1977 Summary Staging GuideSEER Summary Staging Manual - 200071
72SEER Summary Staging Manual - 2000
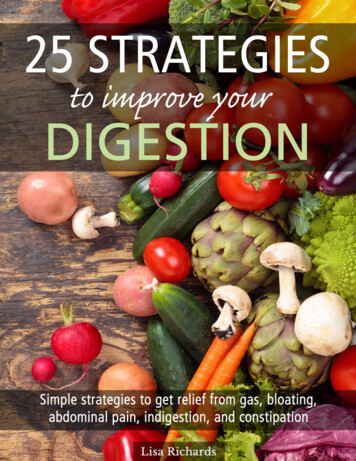
ANATOMIC DRAWINGS OF THE STOMACHCardiac notchFundusBody of stomachDistal esophagusCardiac orificeLesser curvatureGreater curvatureRugae(rugal folds)DuodenumPyloric antrumAngular notchTHE STOMACH (WITH CUT-OUT)Left clavicleEsophagusCardiac Body of stomachGreater curvaturePyloricantrumTHE ESOPHAGUS AND STOMACHSEER Summary Staging Manual - 200073
STOMACHC16.0-C16.6, C16.8-C16.9C16.0 Cardia, NOSC16.1 Fundus of stomachC16.2 Body of stomachC16.3 Gastric antrumC16.4 PylorusC16.5 Lesser curvature of stomach, NOSC16.6 Greater curvature of stomach, NOSC16.8 Overlapping lesion of stomachC16.9 Stomach, NOSSUMMARY STAGE0 In situ: Noninvasive; intraepithelial(Adeno)carcinoma in a polyp, noninvasive1 Localized onlyInvasive tumor confined to:Intramucosa, NOSLamina propriaMucosa, NOSMuscularis mucosaeMuscularis propriaPerimuscular tissue invadedPolyp, NOS:Head of polypStalk of polypSubmucosa (superficial invasion)Subserosal tissue/(Sub)serosal fatExtension through wall, NOSImplants inside stomachIntraluminal spread (only) to esophagus or duodenum##**Invasion through muscularis propria or muscularis, NOSLinitis plastica (diffuse involvement of the entire stomach wall)**Localized, NOS2 Regional by direct extension onlyExtension to:Adjacent tissue, NOSConnective tissue:Gastric nic74SEER Summary Staging Manual - 2000
Code 2 continued on next pageSTOMACHC16.0-C16.6, C16.8-C16.92 Regional by direct extension only (continued)Omentum, NOS:GreaterLesserPerigastric fatDiaphragmDuodenum via serosa or NOSEsophagus via serosaIleumJejunumLiverPancreasSmall intestine, NOSSpleenTransverse colon including flexuresInvasion of/through:Mesothelium#Serosa#Tunica serosa#Visceral peritoneum#3 Regional lymph node(s) involved onlyREGIONAL Lymph NodesCeliac***###Hepatic***###Left gastric (superior gastric), NOS:CardialCardioesophagealGastric, leftGastropancreatic, leftLesser curvatureLesser omentumParacardialPancreaticosplenic (pancreaticolienal)Perigastric, NOSPeripancreaticSEER Summary Staging Manual - 200075
Code 3 continued on next pageSTOMACHC16.0-C16.6, C16.8-C16.93 Regional lymph node(s) involved only (continued)Right gastric (inferior gastric), NOS:GastrocolicGastroduodenalGastroepiploic (gastro-omental), right or NOSGastrohepaticGreater curvatureGreater omentalInfrapyloricPancreaticoduodenalPyloric, NOS:Infrapyloric (subpyloric)SuprapyloricSplenic (lienal), NOS:Gastroepiploic (gastro-omental), leftSplenic hilarNodule(s) in perigastric fatRegional lymph node(s), NOS4 Regional by BOTH direct extension AND regional lymph node(s) involvedCodes (2) (3)5 Regional, NOS7 Distant site(s)/lymph node(s) involvedDistant lymph node(s):Inferior mesentericPara-aorticPorta hepatis (portal) (hilar) [in hilus of liver]RetroperitonealSuperior mesentericOther distant lymph node(s)Extension to:Abdominal wallAdrenal (suprarenal) glandKidneyRetroperitoneumFurther contiguous extensionMetastasis76SEER Summary Staging Manual - 2000
STOMACHC16.0-C16.6, C16.8-C16.99 Unknown if extension or metastasis#Considered localized in Historic StageConsidered regional in Historic Stage###Considered distant in Historic Stage** Considered regional in 1977 Summary Staging Guide*** Considered distant in 1977 Summary Staging Guide##SEER Summary Staging Manual - 200077
ANATOMIC DRAWINGS OF THE SMALL INTESTINESEsophagusStomachSuperiormesenteric arteryAortaGastriclymph nodesDuodenumSuperior mesentericlymph nodesMesentericlymph nodesJejunumIleumMesenterySTOMACH AND SMALL INTESTINE WITH LYMPH NODESArrows show the direction of lymph node drainage78SEER Summary Staging Manual - 2000
ANATOMIC DRAWINGS OF THE SMALL INTESTINESCardioesophagealjunctionStomachPyloric antrumDuodenumIleumSEER Summary Staging Manual - 2000Jejunum79
SMALL INTESTINEC17.0-C17.3, C17.8-C17.9C17.0 DuodenumC17.1 JejunumC17.2 Ileum (excludes ileocecal valve, C18.0)C17.3 Meckel diverticulum (site of neoplasm)C17.8 Overlapping lesion of small intestineC17.9 Small intestine, NOSSUMMARY STAGE0 In situ:Noninvasive; intraepithelial(Adeno)carcinoma in a polyp, noninvasive1 Localized onlyInvasive tumor confined to:IntramucosaLamina propriaMucosa, NOSMuscularis mucosaeMuscularis, NOSMuscularis propriaPolyp, NOS:Head of polypStalk of polypSubmucosa (superficial invasion)Subserosal tissue/(sub)serosal fatTransmural, NOSWall, NOSExtension through wall, NOSIntraluminal to other segments of small intestine or cecumInvasion through muscularis propria or muscularis, NOSLocalized, NOS80SEER Summary Staging Manual - 2000
SMALL INTESTINEC17.0-C17.3, C17.8-C17.92 Regional by direct extension onlyExtension to:All small intestine sites:Abdominal wallAdjacent tissue(s), NOSConnective tissue:Mesenteric fatMesenteryNonperitonealized perimuscular tissueRetroperitoneumFat, NOSDuodenum:Ampulla of VaterBlood vessel(s) (major):AortaGastroduodenal arteryPortal veinRenal veinSuperior mesenteric artery or veinVena cavaDiaphragmExtrahepatic bile duct(s)GallbladderHepatic flexureKidney, NOS:Kidney, rightLiver, NOS:Liver, quadrate lobeLiver, right lobeOmentum, NOS:Greater omentumPancreasPancreatic duct###StomachTransverse colonUreter, rightJejunum and Ileum:Colon including appendixOther segments of small intestine via serosaCode 2 continued on next pageSEER Summary Staging Manual - 200081
SMALL INTESTINEC17.0-C17.3, C17.8-C17.92 Regional by direct extension only (continued)Invasion of/through:All sites:Mesothelium#*Serosa#*Tunica serosa#*Visceral peritoneum#*3 Regional lymph node(s) involved onlyREGIONAL Lymph NodesPericholedochal (common bile ic###Infrapyloric or mesenteric###***Jejunum and Ileum:Ileocolic for terminal ileum onlyMesenteric, NOSPosterior cecal (retrocecal) for terminal ileum onlySuperior mesenteric###***Regional lymph node(s), NOS4 Regional by BOTH direct extension AND regional lymph node(s) involvedCodes (2) (3)5 Regional, NOS82SEER Summary Staging Manual - 2000
SMALL INTESTINEC17.0-C17.3, C17.8-C17.97 Distant site(s)/node(s) involvedDistant lymph node(s)Jejunum and Ileum:Bladder##Fallopian tube(s)##Ovary(ies)##Uterus##Further contiguous extensionMetastasis9 Unknown if extension or metastasis######****Considered localized in Historic StageConsidered regional in Historic StageConsidered distant in Historic StageConsidered localized in 1977 Summary Staging GuideConsidered distant in 1977 Summary Staging GuideSEER Summary Staging Manual - 200083
ANATOMIC DRAWINGS OF THE COLONEsophageal sphincterLiver (left lobe)StomachEsophagusLiver(right lobe)AGreater curvatureIntrahepatic bile ductCommon bile ductPancreasGallbladderSplenic flexureJejunumDuodenumHepatic flexureAscending colonIleumIleocecal valveCecumDescending colonAppendixSigmoid colonRectumAnusTHE ALIMENTARY CANAL84SEER Summary Staging Manual - 2000
ANATOMIC DRAWINGS OF THE COLONTransverse �right colon”)Ileocecal valveDescendingcolonDistal ileum(“left colon”)CecumAppendixSigmoid colonRectumAnusCOLON, RECTUM, AND ANUSLumenMucosaSubmucosaMuscularis propriaSubserosaSerosaPeritoneumLAYERS OF THE COLON WALL OF COLONSEER Summary Staging Manual - 200085
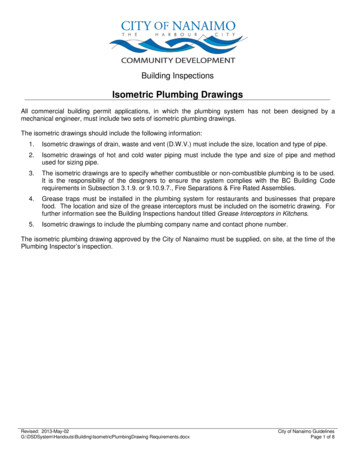
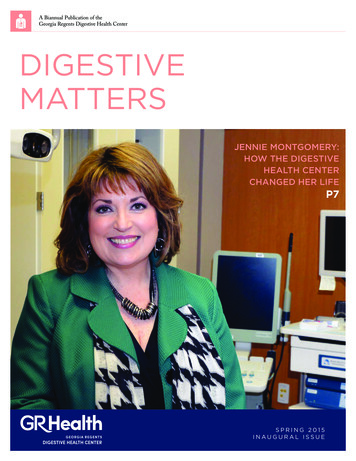
ANATOMIC DRAWINGS OF THE rismucosaCSubmucosaMuscularispropriaSerosaAdapted from: Atlas of Diagnostic Oncology, 2nd Edition, 1996The dark areas (with labels A, B, and C) represent zones of carcinoma. Area A in both the pedunculated polyp and the sessile (or flat) polyp shows no invasion and is therefore in situ. Areas Band C in both polyps are invasive. Notice that polyps are “bulges” in the colon wall with thecorresponding layers of the colon wall (see layers of the colon wall on page 85) within them.CARCINOMA IN A POLYP86SEER Summary Staging Manual - 2000
ANATOMIC DRAWINGS OF THE COLONTransverse colonHepatic flexureSplenic flexureIC IleocolicLymph NodesLeft coliclymph nodesPara- (peri-) coliclymph nodesICAscending(right) colonPrececallymph nodesRetrocecallymph nodesDescending(left) colonInferiormesentericlymph nodesIleocecalvalveCecumAppendixSuperior rectallymph nodesCOLON AND LYMPH NODESSEER Summary Staging Manual - 200087
COLONC18.0-C18.9C18.0 CecumC18.1 AppendixC18.2 Ascending (right) colonC18.3 Hepatic flexure of colonC18.4 Transverse colonC18.5 Splenic flexure of colonC18.6 Descending (left) colonC18.7 Sigmoid colonC18.8 Overlapping lesion of colonC18.9 Colon, NOSSUMMARY STAGE0 In situ: Noninvasive; intraepithelial(Adeno)carcinoma in a polyp or adenoma, noninvasive1 Localized onlyInvasive tumor confined to:Intramucosa, NOSLamina propriaMucosa, NOSMuscularis mucosaeMuscularis propriaPerimuscular tissue invadedPolyp, NOS:Head of polypStalk of polypSubmucosa (superficial invasion)Subserosal tissue/(sub)serosal fatTransmural, NOSWall, NOSConfined to colon, NOSExtension through wall, NOSInvasion through muscularis propria or muscularis, NOSLocalized, NOSNote: Ignore intraluminal extension to adjacent segment(s) of colon/rectum or to the ileum from the cecum.88SEER Summary Staging Manual - 2000
COLONC18.0-C18.92 Regional by direct extension onlyExtension to:All colon sites:Invasion of/through serosa (mesothelium) (visceral peritoneum)#Extension into/through:Abdominal wall###Adjacent tissue(s), NOSConnective tissueFat, NOSGreater omentumMesenteric fatMesenteryMesocolonPericolic fatRetroperitoneum (excluding fat)###Small intestineAscending colon:Kidney, right###Liver, right lobeRetroperitoneal fat###Ureter, right###Transverse colon and flexures:Bile ducts###Gallbladder###Gastrocolic ing colon:Kidney, left###Pelvic wall###Retroperitoneal fat###SpleenUreter, leftSigmoid colon:Pelvic wall###SEER Summary Staging Manual - 200089
COLONC18.0-C18.93 Regional lymph node(s) involved onlyREGIONAL Lymph NodesAll colon subsites:Colic, NOSEpicolic (adjacent to bowel wall)Mesenteric, NOSParacolic/pericolicNodule(s) in pericolic fatCecum and Appendix:Cecal, NOSAnterior (prececal)Posterior (retrocecal)IleocolicRight colicAscending colon:IleocolicMiddle colicRight colicTransverse colon and flexures:Inferior mesenteric for splenic flexure onlyLeft colic for splenic flexure onlyMiddle colic Right colic for hepatic flexure onlyDescending colon:Inferior mesentericLeft colicSigmoid###Sigmoid:Inferior mesentericSigmoidal (sigmoid mesenteric)Superior hemorrhoidal###Superior rectal###Regional lymph node(s), NOS4 Regional by BOTH direct extension AND regional lymph node(s) involvedCodes (2) (3)90SEER Summary Staging Manual - 2000
COLONC18.0-C18.95 Regional, NOS7 Distant site(s)/node(s) involvedAll colon sites unless included in code 2Distant lymph node(s):Para-aorticRetroperitonealSuperior mesenteric§Other distant lymph node(s)Extension to:Adrenal (suprarenal) glandBladderDiaphragmFallopian tube Fistula to skinGallbladderOther segment(s) of colon via serosaOvary Uterus Cecum and appendix:Distant lymph node(s):Inferior mesentericOther distant lymph node(s)Extension to:Kidney, rightLiver##Ureter, rightAscending colon:Distant lymph node(s):Inferior mesentericOther distant lymph node(s)Transverse colon and flexures:Distant lymph node(s):Inferior mesenteric for hepatic flexure and transverse colon onlyOther distant lymph node(s)Extension to:UreterSigmoid colon:Extension to:Cul de sac (rectouterine pouch)UreterFurther contiguous extensionMetastasisSEER Summary Staging Manual - 200091
COLONC18.0-C18.99 Unknown if extension or metastasisConsidered regional for cecum, ascending, desending and sigmoid for Historic stage§ Considered regional for cecum, appendix, ascending, hepatic flexure and transverse colon in 1977Summary Staging Guide Considered distant for splenic flexure in Historic stageNote 1: Ignore intraluminal extension to adjacent segment(s) of colon/rectum and code depth of invasion or extracolonic spread asindicated.Note 2: Terminology such as “Transmural, NOS” and “Extension through the wall, NOS” typically means that the tumor hasinvaded the muscularis propria but has not necessarily invaded the entire thickness of the colon wall.#Considered localized in Historic Stage## Considered regional in Historic Stage### Considered distant in Historic Stage92SEER Summary Staging Manual - 2000
ANATOMIC DRAWING OF THE COLON AND RECTUMDescendingcolonLeft colic nodesSigmoid mesenteric nodesPerirectal nodesRectumSigmoid colonLOWER COLON AND RECTUMAND PRINCIPAL LYMPH NODESSEER Summary Staging Manual - 200093
RECTOSIGMOID JUNCTION, RECTUMC19.9, C20.9C19.9 Rectosigmoid junctionC20.9 Rectum, NOSSUMMARY STAGE0 In situ: Noninvasive; intraepithelial(Adeno)carcinoma in a polyp, noninvasive1 Localized onlyInvasive tumor confined to:Intramucosa, NOSLamina propriaMucosa, NOSMuscularis mucosaeMuscularis propriaPerimuscular tissue invadedPolyp, NOS:Head of polypStalk of polypSubmucosa (superficial invasion)Subserosal tissue/(sub)serosa fat invadedTransmural, NOSExtension through wall, NOSInvasion through muscularis propria or muscularis, NOSLocalized, NOS2 Regional by direct extension onlyInvasion of/through serosa (mesothelium) (visceral peritoneum)#Extension to/through:Adjacent tissue(s), NOSConnective tissueFat, NOSPerirectal fatRectosigmoid:Cul de sac (rectouterine pouch)Mesenteric fatMesenteryMesocolonPelvic wallPericolic fatSmall intestineCode 2 continued on next page94SEER Summary Staging Manual - 2000
RECTOSIGMOID JUNCTION, RECTUMC19.9, C20.92 Regional by direct extension only (continued)Rectum:AnusBladder for males onlyCul de sac (rectouterine pouch)Ductus deferensPelvic wallProstateRectovaginal septumRectovesical fascia for males onlySeminal vesicle(s)Skeletal muscle of pelvic floorVagina3 Regional lymph node(s) involved onlyREGIONAL Lymph NodesRectosigmoid:Colic, NOS:###Left colic###Hemorrhoidal, superior or middleInferior mesentericMesenteric, NOSParacolic/pericolicPerirectalRectalSigmoidal (sigmoid mesenteric)Superior rectalNodule(s) in pericolic fatRectum:Hemorrhoidal, superior, middle or inferiorInferior mesentericInternal iliac (hypogastric), NOS:###ObturatorMesenteric, NOSPerirectalRectalSacral, NOS:###Lateral (laterosacral)Middle sacral (promontorial) (Gerota’s node)PresacralSigmoidal (sigmoid mesenteric)Nodule(s) in perirectal fatRegional lymph node(s), NOSSEER Summary Staging Manual - 200095
RECTOSIGMOID JUNCTION, RECTUMC19.9, C20.94 Regional by BOTH direct extension AND regional lymph node(s) involvedCodes (2) (3)5 Regional, NOS7 Distant site(s)/node(s) involvedDistant lymph node(s):Internal iliac (hypogastric), NOS: for rectosigmoid:**Obturator for rectosigmoidLeft colic for rectum##Other distant lymph node(s)Extension to:Rectosigmoid:Bladder##Colon via serosa##Fallopian tube(s)##Ovary(ies)##Prostate ##Ureter(s)Uterus##Rectum:Bladder for females only##Bone(s) of pelvis##Urethra##Uterus###Further contiguous extensionMetastasis9 Unknown if extension or metastasisNote 1: Ignore intraluminal extension to adjacent segment(s) of colon/rectum and code depth of invasion or extracolonic spread asindicated.Note 2: Terminology such as “Transmural, NOS”, and “Extension through the wall, NOS” typically means that the tumor hasinvaded the muscularis propria but has not necessarily invaded the entire thickness of the colon wall. (See drawing.)######**96Considered localized in Historic StageConsidered regional in Historic StageConsidered distant in Historic StageConsidered regional in 1977 Summary Staging GuideSEER Summary Staging Manual - 2000
ANATOMIC DRAWING OF THE ANUS AND ANAL CANALRectumAnal canalSphinctermusclesSphincter musclesAnal mucosaAnusANUS AND ANAL CANALSEER Summary Staging Manual - 200097
ANUS AND ANAL CANALC21.0-C21.2, C21.8C21.0 Anus, NOSC21.1 Anal canalC21.2 Cloacogenic zoneC21.8 Overlapping lesion of rectum, anus and anal canalSUMMARY STAGE0 In situ: Noninvasive; intraepithelial1 Localized onlyIncidental finding of malignancy in hemorrhoidInvasive tumor confined to:IntramucosaLamina propriaMucosa, NOSMuscularis mucosaeMuscularis propria (internal sphincter)Submucosa (superficial invasion)Localized, NOS2 Regional by direct extension onlyExtension to:Ischiorectal fat/tissuePerianal skinPerineumRectal mucosa or submucosaSkeletal muscles:Anal sphincter (external)Levator aniSubcutaneous perianal tissueVulva3 Regional lymph node(s) involved onlyREGIONAL Lymph NodesAnorectalInferior hemorrhoidalInternal iliac (hypogastric), NOS: for anus###*** and anal canal:###Obturator for anus###*** and anal canal###Lateral sacral (laterosacral)###PerirectalSuperficial inguinal (femoral) for anus and anal canal***Regional lymph node(s), NOS98SEER Summary Staging Manual - 2000
ANUS AND ANAL CANALC21.0-C21.2, C21.84 Regional by BOTH direct extension AND regional lymph node(s) involvedCodes (2) (3)5 Regional, NOS7 Distant site(s)/node(s) involvedDistant lymph node(s)Extension to:Bladder##Broad ligament(s)##Cervix uteri##Corpus uteri##Pelvic peritoneumProstate ##Urethra##Vagina##Further contiguous extensionMetastasis9 Unknown if extension or metastasis## Considered regional in Historic Stage### Considered distant in Historic Stage*** Considered distant in 1977 Summary Staging GuideSEER Summary Staging Manual - 200099
ANATOMIC DRAWINGS OF THE BILIARY TRACTCoronary ligamentFalciform ligamentCystic ductRight hepaticductLefthepaticductNeck ofgallbladderRight lobe of liverCoronaryligamentLeft lobe of liverBody ofgallbladderRound ligament(ligament teres)Common hepatic ductCommon bile ductPancreatic ductAmpulla of Vater(hepatopancreatic ampulla)FundusMajor duodenalof gallbladder papilla (Vater)ANTERIOR VIEW OF THE LIVERGallbladderQuadrate lobe of liverRound ligamentFalciform ligamentRight lobeof liverDEABCLeft lobeof liverA Common bile ductB Hepatic arteryC Portal veinD Cystic ductE Hepatic ductCaudate lobe of liverInferior vena cavaUNDERSURFACE OF THE LIVER100SEER Summary Staging Manual - 2000
ANATOMIC DRAWINGS OF THE BILIARY TRACTStomach pylorusBody of pancreasTail of pancreasDuodenumHTransverse mesocolonattaches hereDistal duodenumH Head of pancreasSuperior mesenteric arterySuperior mesenteric veinMiddle colic arteryTHE PANCREASPeriaorticlymph nodesCeliac trunkCommonhepatic arteryPancreaticospleniclymph nodesLeft gastricarteryPeripancreaticlymph nodesSpleenTailof pancreasSplenic yBody of pancreasTesticular (ovarian) arteryAbdominalaortaTesticular(ovarian)arteryBODY AND TAIL OF PANCREAS(arrows show direction of lymphatic drainage)SEER Summary Staging Manual - 2000101
LIVER AND INTRAHEPATIC BILE DUCTSC22.0-C22.1C22.0 LiverC22.1 Intrahepatic bile ductSUMMARY STAGE0 In situ: Noninvasive; intraepithelial1 LocalizedConfined to one lobe with or without vascular invasionMultiple (satellite) nodules/tumors confined to one lobeConfined to liver, NOSLocalized, NOS2 Regional by direct extension onlyMore than one lobe involved by contiguous growth (single lesion)Extension to:DiaphragmExtrahepatic bile duct(s)Extrahepatic blood vessel(s):Hepatic arteryPortal veinVena cavaGallbladderLesser omentum###Ligament(s):###CoronaryFalciformRound [of eum, NOS:###Parietal###Visceral###Multiple (satellite) nodules/tumors in more than one lobe of liver or on surface ofparenchyma***Satellite nodules, NOS***102SEER Summary Staging Manual - 2000
LIVER AND INTRAHEPATIC BILE DUCTSC22.0-C22.13 Regional lymph node(s) involved onlyREGIONAL Lymph NodesHepatic, NOS:Hepatic arteryHepatic pedicleInferior vena cavaPorta hepatis (portal) (hilar) [in hilus of liver]Periportal###Regional lymph node(s), NOS4 Regional by BOTH direct extension AND regional lymph node(s) involvedCodes (2) (3)5 Regional, NOS7 Distant site(s)/lymph node(s) involvedDistant lymph nodes:Aortic, NOS:Lateral (lumbar)Para-aorticPeriaorticCardiac ##**Coronary artery##**Diaphragmatic:Pericardial (pericardiac)##**PeripancreaticPosterior mediastinal (tracheoesophageal) including juxtaphrenic nodes##**Renal artery##**Retroperitoneal, NOS**Other distant lymph node(s)Extension to:PancreasPleura##StomachFurther contiguous extensionMetastasis9 Unknown if extension or metastasis#####*****Considered regional in Historic StageConsidered distant in Historic StageConsidered regional in 1977 Summary Staging GuideConsidered distant in 1977 Summary Staging GuideSEER Summary Staging Manual - 2000103
GALLBLADDER, OTHER BILIARY, AND BILIARY, NOSC23.9, C24.8-C24.9C23.9 GallbladderC24.8 Overlapping lesion of biliary tractC24.9 Biliary tr
SEER Summary Staging Manual - 2000 69 ESOPHAGUS C15.0-C15.5, C15.8-C15.9 2 Regional by direct extension only Adventitia and/or soft tissue invaded