Transcription
VA TBI Screening and Evaluation ProgramJoel Scholten MDNational Director, Physical Medicine and RehabilitationDouglas Bidelspach MPTRehabilitation Planning Specialist
Poll Question How familiar you are with diagnosis and treatment of TBI?o Not at allo A littleo Moderatelyo Very familiarVETERANS HEALTH ADMINISTRATION
Organization of Today’s Presentation TBI Screening and Evaluation Background Implementation and Enhancements to Programming Research Findings Treatment following a TBI Diagnosis Individualized Rehabilitation and Community Reintegration Care Plan (IRCR)Mayo-Portland Participation Index (M2PI)Opportunities for future InvestigationVETERANS HEALTH ADMINISTRATION
TBI- to Screen or Not to Screen Initial focus at onset of OEF/OIF on returning Servicemembers withmoderate and severe TBI, obvious injuries requiring inpatientrehabilitation. Increasing number of Servicemembers and Veterans noting multiplesymptoms following deployment.o Evaluation and treatment was inconsistent.o Pressure on DoD and VA to develop a system to address this cohort. Collaboration through DVBIC to develop a screening tool.o Deployed by VA April 2007 Debate on cause of symptoms: TBI vs. PTSD vs. both vs. ?VETERANS HEALTH ADMINISTRATION 4
VHA Directive 2010-012 - Screening and Evaluation ofPossible TBI in OEF/OIF(OND) VeteransOutlines screening and evaluation requirements Screening and evaluation address OEF/OIF/OND deployment relatedinjuries Positive screens must be offered referral for Comprehensive TBIEvaluation (CTBIE) CTBIE template should only be completed following a positive screen forOEF/OIF/OND deployment related injuries CTBIE is to be completed at Polytrauma Network Sites or PolytraumaSupport Clinic Team sites by a TBI Specialisto Other sites (Polytrauma Point of Contacts) or use of other providers must berequested through an alternate plan submitted through VISN CMO forVETERANS HEALTHADMINISTRATIONapprovalby National Director PM&R
TBI Clinical Reminder Section 1:o Trauma Events Section 2:o Immediate Disturbance ofConsciousness Symptoms afterEvents Section 3:o New or Worsening Symptomsafter the event Section 4:o Current SymptomsVETERANS HEALTH ADMINISTRATION Initial positive screens tracked for CTBIE:o After YES to Section 1-4 (Section 4 Current Symptoms) the patient has theoption to accept further evaluationo Data Elements: Presence of the national healthfactor TBI-SECTION IV – YES andTBI-REFERRAL SENT health factorOR Presence of the national healthfactor TBI-SECTION IV – YES healthfactor and the absence of TBIREFERRAL DECLINED health factor
Comprehensive TBI Evaluation (CTBIE) Face-to-face or telehealthevaluation completed by TBIspecialist (protocol link below)– http://www.rstce.pitt.edu/VATBI/VATBI.html History of patient’s presentillness/symptoms Focused review of body systems Targeted physical exam Administration of the“Neurobehavioral SymptomInventory (NSI)”VETERANS HEALTH ADMINISTRATION Confirming diagnosis ofdeployment related TBI Develop interdisciplinarytreatment plan Follow up
Poll Question In December 2015, VA completed the 1,000,000th screen for possibledeployment related TBI?o Trueo FalseVETERANS HEALTH ADMINISTRATION
VA Screening for Mild Traumatic Brain Injuryfor OEF/OIF/OND Veterans VHA has screened over 1 Million Veterans for possible mild TBIo 20% of Veterans screen positive and are referred for acomprehensive evaluation From April 2007 to September 30, 2015:o 137,810 completed comprehensive evaluationo 82,468 received confirmed diagnosis of mild TBIo 8.4% of the total Veteran population screened receive a TBIdiagnosisVETERANS HEALTH ADMINISTRATION 9
VA Polytrauma/TBI System of Care 110 Specialized Rehabilitation Siteso 5 Polytrauma Rehabilitation Centers (PRC)o All inpatient, residential, outpatient and telehealth careo 23 Polytrauma Network Sites (PNS)o Outpatient TBI and telehealth care, inpatient rehabilitationo 87 Polytrauma Support Clinic Teams (PSCT)o Outpatient TBI care TBI Screening and Evaluation Program Polytrauma Case Management Polytrauma Transitional Rehabilitation Program Assistive Technology Labs Emerging Consciousness ProgramVETERANS HEALTH ADMINISTRATION Assisted Living TBI Pilotwww.polytrauma.va.gov 10
Integration of Comprehensive Rehabilitation CareAudiologyProgramCare Managementand MilitaryLiaisonsHearingLossPatient ogramsVETERANS HEALTH MentalHealthBrain InjuryProgramPainManagementPTSDProgram 12
Implementation/EnhancementsClinical Program Development PSC Developmento PRC Enhancemento PNS and PSCT Designationo Education, Training, and Oversight roles to establish a System of Care Partnership with Primary Careo Handoff from screening to evaluationo Primary Care models for Post-deployment careo Collaboration with Mental Health and DentalVETERANS HEALTH ADMINISTRATION
TBI Screening and Evaluation:Implementation/Enhancements IT Dateso April 2007 – TBI screeno October 2007 – VSSC TBI evaluation templateo June 2012 – IT supported TBI evaluation template (CTBIE)o Responses linked to consensus TBI definitiono October 2013 – Transition to CTBIE Reportso February 2014 – Concussion Coach (self care app)o August 2015 – Expanded use of TBI Instrumentso December 2015 - TBI Clinical Decision Support (CDS) PilotVETERANS HEALTH ADMINISTRATION
Comprehensive TBI Evaluation (CTBIE):Compliance with Consensus Definition for mTBIJuly 1, 2012VETERANS HEALTH ADMINISTRATION 15
TBI Instruments – Expanded form availabilityVETERANS HEALTH ADMINISTRATION 16
CTBIE DataMonitoring Access to CTBIE and Clinical Services TBI Screening Reporto Goal metric of 95% of all eligible OEF/OIF/OND Veterans have TBI screencompleted if accessing VHA for care Quarterly CTBIE Reportso Timeliness to measure Access to a TBI Specialist- target less than 30 dayso Percentage of TBI screens completing CTBIE- target 75% Sites failing the measure submit a corrective action plan through 10N. Persistentconcerns result in a virtual site visit with CMO and PM&R Program Office. Previously a Performance Measure, now a Quality IndicatorVETERANS HEALTH ADMINISTRATION
CTBIE Template Reports tbi.aspxOutstanding CTBIEs and overall results accessible through main results page.VETERANS HEALTH ADMINISTRATION
IRCR/M2PI ReportsVETERANS HEALTH ADMINISTRATION ummary&rs%3aCommand 19 Render&rc%3aToolbar True
TBI Clinical Decision Support - Where are we ent& MeasurementDevelopDecisionSupportVETERANS HEALTH ADMINISTRATIONBackendIntegrationProcessImprovement 20
TBI Screening and Evaluation: Context TBI screen implemented in 2007o Timeline for implementation precluded research on the TBI screen beforeimplementation or an implementation trialo Unlike the mental health screens, lack of evidence on psychometrics priorto implementationo GAO noted this gap in 2008 (GAO-08-276) Research to support and improve VH!’s TBI screening/evaluation programbecame PT/BRI QUERI’s highest priorityo Research on psychometric properties of TBI screeno Evaluation of implementationVETERANS HEALTH ADMINISTRATION
Research Activities Utilizing CTBIE Data Sensitivity/specificity of screeno Sensitivity 85-94%o Specificity 13-59% Gender differenceso Women less likely than Men to screen positive for possible TBI.o Women report higher degree of symptom interference on CTBIE compared tomen. Cost/Utilizationo QUERI Utilization Reports TBI Screening Fact Sheeto reening-eval.pdfVETERANS HEALTH ADMINISTRATION
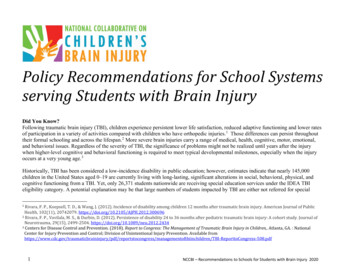
Table 2. Postconcussive Symptoms by Severity in the N 55,070 Veterans Evaluated for TBI*Symptom SeverityModerate toMildNoneVery SevereN%N%N%Irritability, easily annoyed45,389826,282112,2996Sleep 1778,071154,5588Anxious or 85,39410Poor concentration38,851719,472176,74712Poor frustration tolerance, 88,93716Hearing difficulty33,5226111,5372110,01118Depressed or sad33,2236010,7502011,09720Slowed thinking, difficulty organizing,32,2895911,3812111,40021Sensitivity to noise30,0345510,9832014,05326Sensitivity to light27,8675112,2982214,90527Difficulty making decisions27,8775111,6152115,57829Numbness of tingling in parts of body25,9214711,9222217,22731Symptoms in last 30 daysoverwhelmeddifficulty finishing things Scholten J, Sayer N, Vanderploeg R, Bidelspach D, Cifu D. “Analysis of US Veterans Health Administration Comprehensive Evaluations for TBI inOEF/OIF Veterans” Brain Injury September 2012; 26(10): 1177–1184.
TBI Utilization dex.as Led by Brent Taylor, PhD, in close collaboration with PM&Ro PM&R part of research team Leverage VHA administrative data to address the following questions:o What is the prevalence of clinician-diagnosed TBI in Afghanistan andIraq war Veterans who used VHA?o Among those with clinician-diagnosed TBI, what is the rate of cooccurring mental health and pain-related conditions?o What is the cost of providing VHA care to Veterans with TBI?VETERANS HEALTH ADMINISTRATION
First Publication from Utilization ReportsMedical Care. 2012; 50: 342-346VETERANS HEALTH ADMINISTRATION
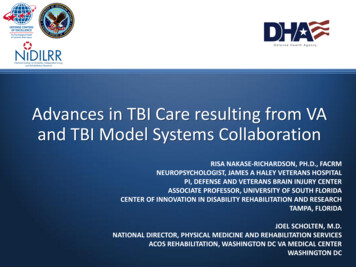
Prevalence of Diagnoses by TBI (FY 2009)TBI(n 22,053)6.7%No TBI(n 305,335)93.3 %Total(n 21%Anxiety22%10%11%Substance 9%12%Back Pain45%23%25%Neck Pain15%5%6%PEainPTVSDETE anRANdS HALT H ADMINISTRATION 54%11%14%DiagnosesMental Health dx
Average VHA Medical Costs for Afghanistan andIraq War Veterans by Diagnosis Group (FY2009)VETERANS HEALTH ADMINISTRATION
Three Years of Utilization Reports Pooled TogetherVETERANS HEALTH ADMINISTRATION
Proportion of Iraq and Afghanistan War Veteranswith Diagnoses of TBI, Pain of the Head, Neck orBack, and/or PTSD Over TimeVHA UserFY2009VHA UserFY2010VHA UserFY2011VHA UserFY2009 toFY2011N 327,388N 398,453N 471,383N ANS HEALTH ADMINISTRATION
Polling Question The best way to differentiate etiology of symptoms in an individual with ahistory of mTBI and PTSD is:o Brain MRIo Brain SPECT scano DTIo Neuropsychological Testingo Clinical InterviewVETERANS HEALTH ADMINISTRATION
Treatment following TBI Diagnosis What is “standard of care” treatment for mild TBI? Clinical Practice Guidelines (CPG)o Developed from best available evidence and consensus opinion fortreatment of symptoms following mild TBIo Published in 2009, updated CPGs will be published in 2016o tbi/VETERANS HEALTH ADMINISTRATION
The Individualized Rehabilitation and CommunityReintegration (IRCR) Care Plan Mandated by Congress in 2010 (38 U.S.C. 1710C, 2010).o Required for all Veterans and Service Members receiving inpatient or outpatientrehabilitation for TBI at a VA facility.o Encourages collaboration amongst Veterans , their families, and providers fromdiverse disciplineso Plan must be communicated to the Veteran in writing, containing:o Comprehensive Evaluationo Goals focused on physical, cognitive, and vocational functioning to ultimately facilitatecommunity reintegrationo Details means to access careo Type, frequency, duration, and location of all rehabilitative treatmentso Name of case managero Dates when plan will be reviewed VHA Handbook 1172.01 Polytrauma System of CareVETERANS HEALTH ADMINISTRATION
IRCR Algorithm Developed by the Physical Medicine & Rehabilitation Program Office to assistclinicians in identifying Veterans in need of an IRCRAlso required for every patient discharged from Polytrauma Rehabilitation Centers(PRC) or Polytrauma Transitional Rehabilitation Program (PTRP).VETERANS HEALTH ADMINISTRATION
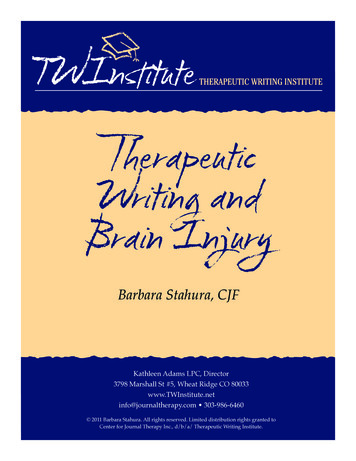
Compliance with the IRCR Algorithm at a singlePolytrauma Network Site Retrospective Chart Review of 546 Veterans with a TBI diagnosis in 2013seen at the DC VAMC PNS.–Work supported by Polytrauma/Blast Related Injury QUERI QLP 56-012400Number of Veteran Cases350300Compliant & DoNot Require IRCR56%250Compliant &Require IRCR20015028%Non-Compliant& Require IRCR100500-50VETERANS HEALTH ADMINISTRATION14%Non-Compliant& Do NotRequire IRCR2%
Ensuring Quality Mayo-Portland Participation Index (M2PI) and InterdisciplinaryRehabilitation Care Plan (IRCR)o Monitor IDT planning and outcomes for outpatients in Polytraumaclinicso 9,500 unique Veterans with M2PI or IRCR in FY15o 9,543 total IRCR planso 5,665 total M2PI entriesVETERANS HEALTH ADMINISTRATION
Opportunities for Future InvestigationoooooFurther study to define “standard of care” treatmentQuantify rehab “dose”Monitor Clinical Practice Guideline (CPG) adherence and link to outcomesCare models to maximize Veteran engagementFuture of TBI Screeno Transition to a Symptom screen vs. De-implementation studyo Maximize efficiency of Interdisciplinary teamso Manage TBI in a chronic Disease Modelo Care Coordinationo Patient Aligned Care Team, Mental Health, Care ManagementVETERANS HEALTH ADMINISTRATION
Selected References and ResourcesCifu DX, Taylor B, Carne WF, Bidelspach D, Sayer NA, Scholten J, Hagel C. Traumatic brain injury, posttraumaticstress disorder and pain diagnoses in OEF/OIF/OND Veterans. J Rehabil Res Dev. 2013;50:1169–76.Ford JH, Wise M, Krahn D, Oliver KA, Hall C, Sayer NA. Family Care Map: Sustaining Patient and FamilyCentered Care in Polytrauma Rehabilitation Centers. J Rehabil Res Dev. 2014; 51(8): 1311-1324.Friedemann-Sanchez G, Sayer NA, Pickett T. Provider perspectives on rehabilitation of patients withpolytrauma. Arch Phys Med Rehab 2008; 89(1): 171-178.Hall C, Sigford B, Sayer NA. Practice changes associated with the Department of Veterans Affairs Family CareCollaborative. J Gen Intern Med Supplement 1 2010; 25: 18-26.Scholten J, Sayer NA, Bidelspach D, Vanderploeg R, Cifu DX. Analysis of U.S Veterans Health AdministrationComprehensive Evaluations for Traumatic Brain Injury in Operation Enduring Freedom and Operation IraqiFreedom Veterans. Brain Injury. 2012; 26 (10): 1177-1184VETERANS HEALTH ADMINISTRATION
Selected References and Resources (continued)Taylor BC, Hagel EM, Carlson KF, Cifu DX, Cutting A, Bidelspach DE, Sayer NA. Prevalence and Costs of CoOccurring Traumatic Brain Injury with and without Psychiatric Disturbance and Pain among Iraq and AfghanistanVeteran VA Users. Medical Care. 2012; 50: 342-346Taylor B, Sayer NA. Guest Editorial: Annual Reports on VHA Healthcare Utilization among Iraq and AfghanistanWar Veterans with TBI and Co-morbidities to Inform Policy, Research and Practice. J Rehabil Res Dev. 2014; 51(7):VII-VIII.Websites:Clinical Practice Guideline for management of concussion/mild TBI available /mtbi/concussion mtbi full 1 0.pdfFamily Care Map available at http://www.polytrauma.va.gov/FCM/PT/BRI QUERI Utilization Reports for OEF/OIF Veterans diagnosed with TBI available pPT/BRI QUERI TBI Screening and Evaluation Fact Sheet available screening-eval.pdfVETERANS HEALTH ADMINISTRATION
Contact Information Joel Scholten, MDJoel.Scholten@va.gov Douglas Bidelspach, MPTDouglas.Bidelspach@va.govVETERANS HEALTH ADMINISTRATION 39
Guidance for completion of the CTBIE by Community Providers1.What providers can complete the Comprehensive TBI Evaluations (CTBIE)?Given the expertise required to establish a diagnosis of TBI and implement appropriate treatmentthe community provider should be a physiatrist, neurologist, or neuropsychiatrist withexperience in interdisciplinary TBI care.2.What information should be communicated to the community provider?It is important to communicate the intent of the process with the community provider, focusingon the Comprehensive TBI Evaluation (CTBIE) specific to OEF/OIF/OND deployment relatedinjuries, and the significance of the questions on loss of consciousness, alteration ofconsciousness, and post traumatic amnesia at the time of injury for the historical diagnosis ofdeployment related TBI.3.What is the primary method that the evaluator should use for deriving a TBIdiagnosis?The diagnosis of TBI involves documenting a historical event during deployment and itsimmediate sequelae. The TBI diagnosis is based entirely on history – either a credible historyfrom the patient or medical record documentation that:i. There was an event that had the potential to cause a significant force to the headii. This force to the head was immediately followed by:a. Any period of loss of or a decreased level of consciousnessb. Any loss of memory for events immediately before or after the injury (posttraumatic amnesia)c. Alteration in mental state at the time of the injury (mental confusion,disorientation, slowed thinking, etc.)d. Neurological deficits (e.g., neurological signs such as weakness, loss of balance,sensory loss, aphasia, etc.) that may or may not be transiente. Intracranial lesion on neuroimagingNot all individuals exposed to an external force will sustain a TBI, but any person who has ahistory of such an event with immediate manifestation of any of the above signs or symptomscan be said to have had a TBI.If the patient cannot reliably or believably provide this information, ask about what they weretold by others who were at the scene. Were they lying on the ground and non-responsive (TBI)?Were they saying things that did not make sense (TBI)? Immediately afterward, while still at thescene, were they able to walk, talk, and function normally (unlikely to have had a TBI)?
4.How should the Comprehensive TBI Evaluation (CTBIE) completed by acommunity provider be documented?The evaluations should be documented using the word version of the CTBIE, which is returnedand scanned into CPRS. The local VA team can then access the CTBIE template in TBIInstruments, and check the first box indicating the evaluation was completed by a ‘fee’ provider,specify if the diagnosis was confirmed or ruled out, and outline the treatment plan in thetemplate. If the MD does not enter the CTBIE note into TBI Instruments, the team membercompleting the entry (transposing the results of the three available sections from the CTBIE intothe online template), should identify the MD of the team as a cosigner on the note, and ensure theindividualized treatment plan is developed and carried out, as indicated.5.When is neuropsychological testing indicated?Neuropsychological testing cannot establish a diagnosis of TBI and is not indicated in all cases.It is only indicated when it will help document potential residual effects, assist in treatmentplanning, or help evaluate treatment response. However, because of rapid improvement expectedfollowing mild TBI, neuropsychological testing is not recommended during the first 30 days postinjury, except in cases of acute concussion management when it may be used to monitor therecovery process and assist with determining return to work/school. Providers should considerreferring patients for neuropsychological testing who have persistent cognitive complaints aftertreatment and if alternative explanation for these cognitive complaints, such as PTSD, depressionand insomnia, have been ruled out. In these cases, neuropsychological testing may be indicatedand useful in determining if there are objective findings to support the subjective symptomcomplaints; and if so, the nature, severity, and likely etiology of those objective cognitiveproblems.6.Are there training resources the community provider should access?Consistent with VA provider training, a community provider completing the Comprehensive TBIEvaluation should access the VHI training or the VA/DoD Clinical Practice Guideline forConcussion/mild Traumatic Brain Injury, which can be accessed through the links below.VA/DoD Clinical Practice Guideline: Management of Concussion/Mild Traumatic nes/Rehab/mtbi/Veterans Health Initiative – Traumatic Brain iative/traumatic brain injury.asp
o 87 Polytrauma Support Clinic Teams (PSCT) o Outpatient TBI care TBI Screening and Evaluation Program Polytrauma Case Management Polytrauma Transitional Rehabilitation Program Assistive Technology Labs Emerging Consciousness Program Assisted Living TBI Pilot . VETERANS HEALTH ADMINISTRATION . www.polytrauma.va.gov