Transcription
Ministry of Health - Sri LankaNationalGuidelinesGuidelines on Management of Dengue Fever &Dengue Haemorrhagic FeverIn AdultsIn Collaboration with theCeylon College of PhysiciansRevised and expanded editionNovember 2012
The guidelines, published in November 2012, supersede the previousguidelines on Management of Dengue Fever / Dengue Haemorrhagic Feverpublished by the Epidemiology Unit, Ministry of Health in 2010.These guidelines were developed based on the best available evidence at thetime of writing. It is expected to be used in the clinical management ofdengue infection in Sri Lanka. The guidelines will be reviewed periodicallywhen new evidence becomes available.Please forward your comments and suggestions to the following address bypost or e-mail.The EpidemiologistEpidemiology Unit231, De Saram PlaceColombo -10E-mail: chepid@sltnet.lkElectronic version is available on www.epid.gov.lkISBN: 978-955-0505-35-7
Guidelines Development CommitteeDr Nirmalee GunawardaneDr Ananda WijewickramaDr Upul DissanayakeDr Kamani WanigasuriyaDr Panduka KarunanayakaDr Lallindra GooneratneDr Priyankara JayawardanaDr M K RagunathanDr Vasanthi PintoProf Athula KaluarachchiDr Sunethra GunasenaDr LakKumar FernandoDr Jayantha WeeramanDr Hasitha TisseraConsultant PhysicianTH KandyConsultant PhysicianIDH ColomboConsultant PhysicianDGH KalutaraSenior Lecturer in Clinical MedicineFaculty of Medical SciencesSri JayawardenepuraSenior Lecturer in Clinical MedicineFaculty of Medicine ColomboSenior Lecturer in Pathology (Haematology)Faculty of Medicine ColomboResident PhysicianCSHWConsultant PhysicianNHSLSenior Lecturer in AnaesthesiologyFaculty of Medicine Peradeniya(RepresentativeCollege of Anaesthesiologists Sri Lanka)Professor in Obstetrics and GynaecologyFaculty of Medicine Colombo(Representative Sri Lanka College ofObstetricians and Gynaecologists)Consultant Medical VirologistMedical Research InstituteConsultant PaediatricianDGH NegomboConsultant PaediatricianEpidemiology UnitConsultant EpidemiologistEditorial Assistance and Cover pageDr D. RathishResearch AssistantEpidemiology UnitEditorial Assistance (2010 Edition)Dr P. WijayagoonawardanaRegistrar in Medicine,Sri Jayewardenepura General Hospital
ContentsForewordviPreface IviiPreface IIviii1. Introduction12. The Natural Course of the illness2.1 Undifferentiated fever22.2 Dengue Fever (DF)222.3 Dengue Haemorrhagic Fever (DHF)32.4 Expanded dengue syndrome53. Diagnosis at OPD Level & by the Primary Care Physician64. Criteria for Admission75. Management of those who do not need Admission86. Inward Patients96.1 Introduction96.2 Detection of critical phase (onset of plasma leakage)96.3 Early detection of shock106.4 Monitoring patients during hospital stay116.5 Management of inward patients136.6 Options of Fluid for Resuscitation206.7 ABCS216.8 Indications for Blood Transfusion216.9 Indications for Haemodynamic Support227. Management of Hepatitis and Hepatic Encephalopathy in8. DHFDengue in Pregnancy8.1 Management of pregnant patients with DF/DHF close todelivery8.2 Management of patients with DF/DHF during immediatepostpartum232425259. Myocardial Involvement in Dengue2610 Place of Adjunctive Therapy in the Management of DHF. 10.1 Platelet transfusion272710.2 Fresh frozen plasma transfusion2710.3 Steroids and I.V. immunoglobulin2710.4 Recombinant Factor VII28
10.5 Antibiotics2810.6 Frusemide2810.7 Tranexamic acid2810.8 Calcium gluconate11 Dengue in Co-morbid Conditions.12 Transferring a patient to another Institute.13 Discharge.14 Laboratory Diagnosis.15 Outbreak Response Plan for Hospitals.AnnexuresAnnexure I - Monitoring Chart I - In Dengue suspected patients fromthe time of admission – Intake and Output chartAnnexure II - Monitoring Chart II - In Adult patients without evidenceof fluid leakage2829313233343637Annexure III - Monitoring Chart III - In Adult Patients with FluidLeakage38References39
ForewordRecent trends on morbidity and mortality of Dengue illness has caught theattention of people of various walks of life. The in-ward and the outpatientdepartments of the hospitals of Sri Lanka are receiving increasingnumbers of patients with dengue illness.This newly revised national guidelines, on management of dengue feverand dengue haemorrhagic fever in adults, developed by the EpidemiologyUnit of Ministry of Health in collaboration with the Ceylon College ofPhysicians, Sri Lanka College of Obstetricians and Gynaecologists andCollege of Anaesthesiologists Sri Lanka, is expected to further improveexisting knowledge and bridge any gaps on the above topic.I hope that this document would have a positive influence on themanagement of patients with dengue illness.Dr. Y.D.N. JayathilakaSecretaryMinistry of Healthvi
Preface IThe Ceylon College of Physicians is happy to be a partner of thiscomprehensive guidelines developed by the Epidemiology Unit of theMinistry of Health in consultation with major professional bodies in thecountry. The clinical management of dengue patients varies mainly due tothe lack of national guidelines. While some current recommendations arebacked by clear evidence, some recommendations are not supported bysolid data. Therefore the need of national guidelines with the concurrenceof major professional bodies is strongly felt.The Ceylon College of Physicians considered this project a top priority andgot involved with it from the beginning. While thanking our members whocontributed to this project, I hope that these guidelines will assistclinicians who are fighting to save the lives of patients with dengue, in thiscountry.Prof. Sarath LekamwasamPresidentCeylon College of Physiciansvii
Preface IIThe impact of Dengue illness on the health care system of Sri Lanka hasmade it one of the household names in the recent past. It has influencedvarious other fields such as economy, policy making and environmentalsciences. This highlights the need of frequent update of the knowledge onclinical management of dengue illness.The Epidemiology Unit of Ministry of Health conducted a series of meetingswith a group of specialists who contributed to the previous guidelines in2010 and who were endorsed by the Ceylon College of Physicians, SriLanka College of Obstetricians and Gynaecologists and College ofAnaesthesiologists Sri Lanka, to revise the prevailing national guidelineson the management of dengue fever and dengue haemorrhagic fever inadults. This is intended to reach all levels of the health care services whichwould lead to reduction in morbidity and prevention of mortality due todengue illness.I extend my gratitude to each and every one who contributed towards thedevelopment of this guideline.Dr. Paba PalihawadanaChief Epidemiologistviii
1. IntroductionThe clinical course of dengue infection varies from individual to individualand even in the same individual from time to time. This guideline includesnew concepts, based on scientific evidence, on the management of DengueFever (DF) and Dengue Haemorrhagic Fever (DHF). It emphasizes theimportance o f early detection of beginning and end of plasma leakage;prevention, early detection and treatment of shock and othercomplications. Management of special situations such as Dengue inpregnancy and the place for adjunctive treatment in Dengue are alsodiscussed.1
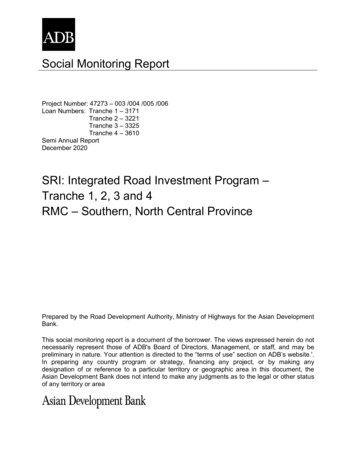
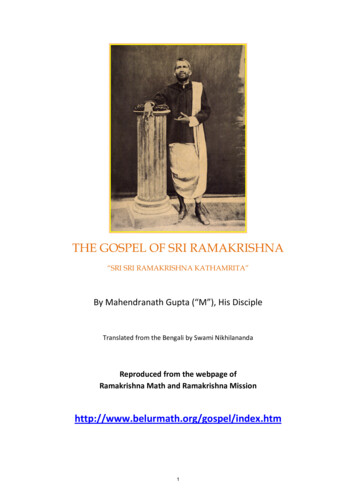
2. The Natural Course of the IllnessMany patients infected with dengue virus remain asymptomatic. Others,after an incubation period of 4-7 (range 3-14) days, develop a febrileillness which could turn out to be one of the following. Undifferentiated feverDFDHFExpanded dengue syndrome (rare)Dengue Viral InfectionSymptomaticAsymptomaticUndifferentiated fever(Viral Syndrome)WithbleedingDFWithoutbleedingDHFExpanded dengue syndrome/Isolated organopathy(Unusual manifestations)WithoutshockWith shockDengue shock syndrome (DSS)Courtesy: comprehensive guidelines for prevention and control of dengue anddengue haemorrhagic fever. Revised and expanded edition. (SEARO TechnicalPublication Series No. 60) 20112.1. Undifferentiated feverThose who have been infected with dengue virus, especially for the firsttime (i.e. primary dengue infection), may develop a simple feverindistinguishable from other viral infections.2.2. Dengue fever (DF)It is generally an acute febrile illness, with severe headache, myalgia,arthralgia and rashes. Leucopenia and thrombocytopenia may also beobserved. Although DF may be benign, it could be an incapacitatingdisease with severe headache, muscle and joint and bone pains (breakbone fever). Occasionally unusual haemorrhage such as gastrointestinalbleeding, hypermenorrhea and massive epistaxis may occur.2
Undifferentiated febrile illness and classical dengue fever can be managedas any other viral fever with symptomatic treatment. However, often it isdifficult to differentiate DF from DHF in the early phase (febrile phase) ofthe illness.2.3. Dengue haemorrhagic fever (DHF)DHF is characterized by the acute onset of high fever and is associatedwith signs and symptoms similar to DF in the early febrile phase. Plasmaleakage is the hallmark of DHF which occurs soon after the end of thefebrile phase. There is a tendency to develop hypovolemic shock (dengueshock syndrome) due to plasma leakage.Therefore suspected DF and DHF patients should be closely monitored toidentify patients with DHF.For efficient management of DHF it is important to understand its naturalhistory and its dynamic nature. Clinical course of DHF is stereotypic andconsists of three stages Febrile phaseCritical phase (leakage phase)Convalescent phase2.3.1. Febrile phaseFebrile phase is characterized by continuing high fever lasting for 2-7days. Other features seen in the febrile phase include facialflushing/diffuse blanching erythema of the skin, myalgia, arthralgia,headache, nausea and vomiting. Some patients may have sore throat,injected pharynx, conjunctival injection and diarrhoea. Mild haemorrhagicmanifestations can occur. Leucopenia (WBC 5000 mm3) and mildthrombocytopenia ( 150,000 /mm3) are common in the late febrile phase.Above features are usually indistinguishable between DF and DHF duringthe febrile phase. However, the presence of tender hepatomegaly favoursthe diagnosis of DHF.2.3.2. Critical phase (leakage phase)The critical phase is heralded by the onset of plasma leakage. Thisusually occurs towards the late febrile phase, often after the 3rd day offever, usually around the 5th or 6th day of illness with defervescence(settling of fever). However some patients may enter the critical phasewhile having high fever.3
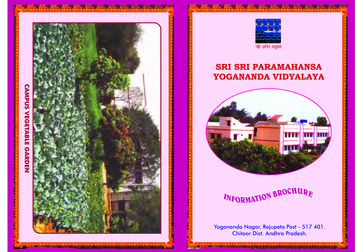
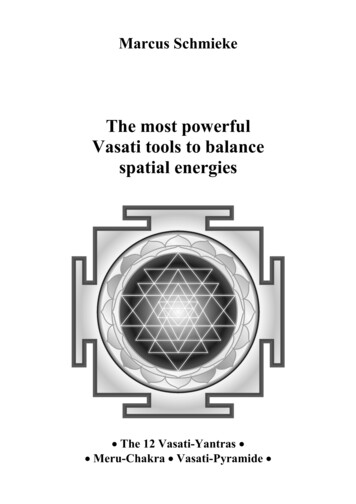
Plasma leakage is due to increased capillary permeability. Plasma leakagein DHF is selective and transient and usually lasts f o r 24-48 hours.Increased capillary permeability is the result of immune mediators and isnot a result of destruction of capillaries. Though the disease is systemic,plasma leakage occurs selectively into the peritoneal and pleural spaces.Pericardial effusion, if there is any, is rather minimal. Generalized or facialoedema, if seen, is more likely to be due to fluid overload rather than due toplasma leakage.With the leakage of plasma there will be haemo-concentration which willmanifest as an increase in HCT. A 20% rise of HCT from the baseline isindicative of significant plasma leakage. (A smaller rise in HCT which maybe seen in the early phase of the disease is usually due to dehydration). Arise in HCT less than 20% can be found in patients who received excessoral/I.V. fluids or in patients with bleeding.Other evidence of plasma leakage are a decrease in serum albumin( 3.5g/dl) and non-fasting serum cholesterol ( 100 mg/dl).The degree and the rate of plasma leakage in DHF can vary. It can beminimal in some patients while in others it can be very significant.HaematocritThe leak usually starts slowly, increases gradually, slows down and thenceases altogether at the end of leakage phase (usually within 48 hoursfrom the onset).Loss of plasma24 h24 hCritical phase (48 h)Figure: Fluid leakage in the critical phaseThose who have severe leakage may develop shock when a critical volume ofplasma is lost. If the shock is prolonged consequent organ hypo-perfusionwill result in progressive organ impairment, metabolic acidosis anddisseminated intravascular coagulation (DIC) which often lead to massivebleeding.4
Therefore early detection of critical period (onset of plasma leakage) andappropriate fluid management is of paramount importance.Haemorrhagic manifestations are not essential for the diagnosis of DHFin the presence of objective evidence of plasma leakage (refer page 09).However the term “DHF” is retained because these patients may developovert or concealed bleeding during the course of illness.2.3.3. Convalescent phase (recovery phase)This starts after the end of the critical phase and usually lasts 2-5 days.There will be reabsorption of extravasated fluid during this period.Features which would suggestconvalescent phase are: thatthe patienthas reached theImproved general wellbeing and improved appetiteAppearance of convalescent rashGeneralized itching (more intense in palms and soles)Haemodynamic stabilityBradycardia (seen in some patients)DiuresisStabilization of Haematocrit (HCT) may even be lower than baselinedue to reabsorption of extravasated fluid)Rise in white cell count followed by a rise in the platelet count.However, if excessive amounts of intravenous (IV) fluids have been used inthe critical phase there could be signs of fluid overload such asrespiratory distress due to pulmonary oedema or large pleural effusions.2.4. Expanded dengue syndrome/ Isolated organopathy (unusualmanifestations)Patients with dengue illness can sometimes develop unusualmanifestations such as involvement of liver, kidneys, brain or heart with orwithout evidence of fluid leakage and therefore do not necessarily fall intothe category of DHF. These conditions are very rare and management issymptomatic. Such unusual manifestations may be associated with coinfections and comorbidities. However, these manifestations if seen in DHFpatients are mostly a result of prolonged shock leading to organ failure.5
3. Diagnosis at OPD Level & by the Primary Care PhysicianIn the present hyper-endemic setting in Sri Lanka, dengue illness (DF andDHF) should be considered in the differential diagnosis of patientspresenting with acute onset of fever with the following: Headache, especially retro-orbital painMyalgia /ArthralgiaRash (diffuse, erythematous, macular)Haemorrhagic manifestations (petechiae, positive tourniquet test etc.)Leukopenia ( 5000 /mm3)Rising haematocrit of 5 - 10 %Platelet count 150,000 /mm36
4. Criteria for AdmissionThe first contact physician may decide to admit a patient on clinicaljudgment. However it is essential to admit patients: With a platelet count of 100,000/mm3(Platelet count above 100,000/mm3 but below 150,000/mm3 anddropping rapidly may be admitted depending on the circumstances) With the following warning signs after day 3 of fever/illness: Abdominal pain or tenderness Persistent vomiting Clinical signs of plasma leakage: pleural effusion, ascites Mucosal bleeding Lethargy, restlessness Liver enlargement 2 cm Increase in HCT concurrent with rapid decrease in platelet countOther patients who may need admission even without the above criteriaare: Pregnant mothersElderly patientsObese patientsPatients with co-morbid conditions like diabetes, chronic renalfailure, ischaemic heart disease, thalassaemia and otherhaemoglobinopathies and other major medical problemsPatients with adverse social circumstances- e.g. living alone, livingfar from health facility without reliable means of transport.7
5. Management of those who do not need AdmissionFollowing treatment measures are recommended: Ensure adequate oral fluid intake of around 2500 ml for 24 hours(if the body weight is less than 50kg give fluids as 50ml/kg for 24hours). This should consist of oral rehydration fluid, king coconutwater, other fruit juices, kanji or soup rather than plain water.Exclude red and brown drinks which could cause confusion withhaematemesis or coffee ground vomitus. Adequate physical rest Tepid sponging for fever Paracetamol not exceeding 2 tablets six hourly (reduce dose forpatients with lower body weights). Warn the patient that the fevermay not fully settle with paracetamol and advice not to takeexcess. A nti-emetics and H2 receptor blockers if necessary Avoid all NSAIDS and steroids Withhold Aspirin, Clopidogrel & Dipyridamole in patients who takethese on long term basisReview daily with Full Blood Count (FBC). First FBC should be done atleast on the third day of fever/illness and daily thereafter if the plateletcount is 150,000/ mm3. FBC should be done twice daily if the plateletcount is 150,000/ mm3. (However a FBC should be done on the firstday of fever in pregnant patients and in patients with co-morbidities).Note: A normal full blood count or a count suggestive of bacterialinfection on the first day of illness does not exclude Dengue illness.Therefore follow up FBCs are essential.Advise immediate return for review if any of the following occur:Clinical deterioration with settling of feverInability to tolerate oral fluidsSevere abdominal painCold and clammy extremitiesLethargy or irritability/restlessnessBleeding tendency including inter-menstrual bleeding ormenorrhagia Not passing urine for more than 6 hours 8
6. In-ward Patients6.1 IntroductionIn-ward patients include patients with DF and patients with DHF.Differentiation between these two is difficult during t he initial few days(first three to four days of fever).The hallmark of DHF is plasma leakage. This is not present in DF. Plasmaleakage is the main cause for shock, subsequent bleeding, organ failureand death.The only way of diagnosing a patient with DHF clinically is the detection ofplasma leakage. Therefore the mainstay of in-ward care is: Early detection of plasma leakage (onset of critical phase) Judicious fluid management to prevent shock and fluid overload6.2 Detection of critical phase (onset of plasma leakage)A white cell count of 5000/mm3 or less with predominance of lymphocytesand a platelet count less than 100,000/mm3 indicate that the patient mayenter the critical phase within the next 24 to 48 hours if behaves as DHF.Plasma leakage begins around the transition from the febrile to the afebrilephase. However, some patients may continue to have fever even during thecritical phase.A progressively rising HCT even before reaching a rise of 20%, with otherfeatures such as tender hepatomegaly may indicate that the patient isentering the critical period.Presence of pleural effusion and ascites indicates that the patient isalready in the critical phase. Pleural effusion detected clinically may not beobvious in a Chest X Ray (CXR)-PA, but may be seen only in a CXR rightlateral decubitus film. Use of a focused ultra sound scan (USS) will helpto identify clinically undetectable Pleural effusion and Ascites (Gallbladder wall oedema may be seen by USS in both DF and DHF. Though itmay also be the earliest sign of leaking in DHF; if pericholecystic oedemais not progressing in subsequent USS such patients are likely to have onlyDF). If appropriate interventions are not adopted early, the patient mayprogress to develop shock.9
6.3 Early detection of shock In a patient with features of Dengue haemorrhagic fever Compensatedshock is defined as circulatory failure manifested by narrow pulsepressure (less than or equal to 20mmHg). If there is hypotension (SBP 90mmHg or reduction of SBP by 20% ormean BP 60mmHg) the patient is in Decompensated shock. If the bloodpressure and pulse is un-detectable the patient is in Profound shock.It is important to detect the patient before going into shock status (DuringPre-shock stage). If an abnormality is detected even in one vital parametermentioned in 6.4.3 (eg: Tachycardia, Prolong capillary refill time or pulsepressure less than 25mmHg) this might indicate that the patient isprogressing towards shock. Therefore, close monitoring, properassessment and appropriate timely action is essential.Prevention or early treatment of shock is essential if complications areto be avoided. To detect shock early, observation for following symptomsand signs is important. Hence maintenance of monitoring charts, whichhelp to detect early symptoms and signs of shock, is important in themanagement of DF/DHF. Please refer to annexure I-III for the monitoringcharts.Symptoms suggestive of Pre-shock/Shock (from 3rd day of illness) Sweating Abdominal pain Persistent vomiting Restlessness / altered conscious level Postural dizziness Decreased urine output (OUP) ( 0.5 ml/kg/hour) Calculate the urine output in ml/kg/hr, using the sameweight used for fluid calculation.Signs suggestive of Pre-shock/Shock (from 3rd day of illness)Cold extremitiesProlonged capillary refill time 2 secondsUnexplained tachycardiaIncreasing diastolic pressureNarrowing of pulse pressure 20 mmHgPostural drop 20 mmHg of systolic blood pressureHypotension ( 20% from patient’s baseline or SBP 90mmHg if baseline not known or mean BP 60mmHg)Increased respiratory rate10
6.4 Monitoring patients during hospital stay6.4.1 If the patient is clinically stable on admission and DF/DHF issuspected Chart temperature 4 hourlyAssess vital signsWatch for evidence of bleeding specially malena or bleeding pervagina and quantify.Maintain an intake and output chart (annexure I). Fluid balanceshould be calculated, documented and assessed 6 hourly.Calculate the urine output in ml/kg/hr, using the same weight usedfor fluid calculation.Do a full blood count on admission and then daily6.4.2 When platelet count drops below 130,000/mm3Start monitoring using the monitoring chart annexure II. The purpose of this monitoring is to detect entry into thecritical phase.Monitor ; General condition, appetite, vomiting, bleeding and other signs andsymptoms as in page 10. Temperature four hourly Vital parameters- pulse, blood pressure (both systolic and diastolic),respiratory rate, and capillary refill time - three hourly Detailed fluid balance ( A n n e x u r e I ) with: Intake with type and route of fluid Output - urine/vomitus/diarrhoea/bleeding (quantify)Fluid balance should be calculated, documented and assessed 6hourly. FBC twice daily HCT 6 hourly6.4.3When the patient enters into the critical phase (leakage phase)Start monitoring using the monitoring chart annexure III. The purpose of maintaining this monitoring chart is foraccurate fluid management and early detection of shock.11
Entry into the Critical phase is indicated by evidence of plasma leakageand more frequent monitoring is now necessary.Monitor, Vital parameters- hourly Fluid balance chart- assess three hourlyConsider introducing an indwelling urinary catheter in All high risk patients during critical phase Patients in shock HCT - three hourly or more frequentlyIn addition to these, monitor other parameters mentioned in 6.4.2.6.4.4 If there is evidence of shock (compensated/ decompensated)Vital parameters should be checked every 15 minutes till the patient ishaemo-dynamically stable. During intense fluid resuscitation HCT shouldbe checked immediately before and 15 minutes after each fluid bolus andthen at least two to three hourly.If the shock is prolonged (not responding to initial fluid bolus) anindwelling urinary catheter should be inserted and urine outputshould be measured hourly. Due to fluid extravasation leading to arelative reduction in intravascular volume, the urine output (UOP) islikely to be less than normal. Hence, a UOP of 0.5 ml to 1 ml/kg bodyweight / hour is adequate during this period. Overenthusiastic fluidreplacement to achieve a higher UOP may lead to fluid overload.Liver profile, blood sugar, serum calcium, serum electrolytes, serumcreatinine, clotting profile and venous blood gases should be done incomplicated cases such as prolonged shock, not responding to adequatefluid resuscitation, liver failure and renal failure.6.4.5 In convalescent phaseLook for features of improvement (Refer page 05). Watch for symptoms andsigns of fluid overload such as periorbital oedema, cough, wheeze andtachypnoea, rise of both systolic and diastolic blood pressures withwidening of pulse pressure, basal crepitations and rhonchi. Urine outputis usually high during this phase. Some patients may develop bradycardiawhich is usually asymptomatic and transient. Therefore, continue tomonitor vital signs and maintain intake and output chart.12
6.5 Management of in-ward patients6.5.1 Febrile phase with platelet count more than 100,000/mm3Management of this phase is essentially similar to outpatient managementexcept for the addition of intravenous fluids. IV fluids may be indicated inpatients who are unable to take adequate oral fluids, or in patients withdiarrhoea or vomiting.Type of I.V. fluid should be Normal Saline or Hartmann’s solution. Thetotal amount of fluid (both I.V. and oral) should be limited to 2500 ml for24 hours for an average adult (2 ml/Kg/hr upto a maximum of 50 Kg ofweight).However, if there is vomiting or diarrhoea this amount should beincreased and dehydration should be corrected.It should be emphasized that over- hydration during this phase willnot prevent patients developing shock in the Critical phase. In fact itmay cause fluid overload during t h e Critical phase.6.5.2 When the platelet count drops below 100,000/mm318 G (green) cannula should be inserted and an intravenous infusion ofnormal saline or Hartmann’s solution should be started. Fluid intake perhour should be about 100ml (IV and oral) for an average adult of 50kg ormore. If the body weight is less than 50kg maintenance fluid should begiven (2ml/kg/hour).Total (both oral and I.V) amount of fluid intake should be about2500ml per day for an average adult unless the patient has vomiting /diarrhoea.6.5.3 When the patient is in the critical phase (leakage phase)The fluid requirement, both oral and intravenous, in critical phase (48hours) is calculated as M 5% (maintenance 5% deficit). Maintenance(M) is calculated as follows: For the 1st 10 kgFor the 2nd 10 kgFrom 20 kg and above up to 50 kg5% deficit is calculated as 50 ml/kg up to 50kg-100 ml/kg- 50 ml/kg- 20 ml/kg13
Example of fluid calculation for a 65 kg person (maximum body weight forfluid calculation is 50 kg) For the 1st 10 kg - 100 ml/kgFor the 2nd 10 kg - 50 ml/kgFrom 20 kg and above up to 50 kg -20 ml/kg5% deficit is calculated as 50 ml/kg up to 50 kg 1000 ml 500 ml 600 ml 2500 mlTherefore the maximum fluid requirement for an average adult forthe entire phase of critical 48 hours is 4600 ml.If the body weight is less than 50 kg, calculation should be done accordingto the ideal body weight or actual body weight whichever is less.Fluid quota is aimed at giving just adequate amount of fluid to maintainperfusion to vital organs without causing fluid overload. Once the fluidquota is exceeded chances of fluid overload is high. All patients will notneed the full fluid quota of M 5% and some may need less than this.The recommended intravenous fluid is normal saline or Hartmann’ssolution. Oral fluids should consist of electrolyte solutions such as kingcoconut water, other fruit juices, oral rehydration fluid and kanji.Drinking plain water should be minimized.How this volume should be infused during the critical period dependson the haemo-dynamic status of the patient.If the patient is haemo-dynamically stable (non-shock), but in t h eCritical (leaking) phase this volume (M 5%) could be spread over 48hours. However this volume should not be given at a uniform rate. Thevolume given should be just sufficient to maintain an effective circulationduring the period of plasma leakage as too much fluid could lead to fluidoverload.In keeping with the dynamic nature of the leakage, fluid should bestarted at a slower rate. The rate of fluid should be increased in a stepwise pattern, guided by HCT and other parameters. Since plasma leakagedoes not persist at a higher rate for more than a few hours, it is necessaryto reduce the rate of fluid intake in a step wise pattern again. Urine outputs h o u l d b e m a i n t a i n e d a t 0.5-1 ml/kg/hour (Calculate the urineoutput in ml/kg/hr, using the same weight used for fluid calculation) andpulse pressure around 30mmHg during the entire critical period.14
It should be emphasized that the HCT is a guide for fluid management.Trying to normalize the HCT will generally result in fluid overload.Given above is the general pattern of fluid leakage during the criticalphase. It is important to note that there are individual variations ofleakage. In rapid leakers peak of the leakage will be reached much earlier(before 24 hours). In slow leakers peak of the leakage will be reachedmuch later (after 24 hours).If the patient has signs of Pre-shock (refer 6.3) rate of fluid should beincreased to maintain the vital parameters stable. However a rate as highas 7ml/kg/hr is only very rarely needed and even rates as high as5ml/kg/hr if needed will only be needed for a short period (usually lessthan a couple of hours) in a very large majority of patients.6.5.4 If a patient presents with shock/goes into shock while in wardIn any patient presenting with shock Dengue Shock Syndrome should beconsidered as a differential diagnosis in the present context of hyperendemicity. Fluid therapy in an in-ward DHF patient is aimed at givingjust sufficient volume to maintain an effective circulation during theleaking period thereby preventing patient from going into shock.If the volume given is inadequate or if the leak is very rapid, the patientmay go into shock. Close monitoring and appropriate fluid therapy isaimed at preventing this from happening.In a patient with shock a blood sample should be collected formeasurement of HC
The leak usually starts slowly, increases gradually, slows down and then ceases altogether at the end of leakage phase (usually within 48 hours from the onset). Loss of plasma 24 h 24 h Critical phase (48 h) Figure: Fluid leakage in the critical phase Those who have severe leakage may develop shock when a critical volume of plasma is lost.