Transcription
Ministry of Higher Education and Scientific SearchBabylon University- College of NursingSecond stageSecond semsterPractical Microbiology for Nurses2018ByA.Professor Dr. Nada Khazal K. HindiDr.Hiba JassimDr.Mays Hadi
lab:1FungiFungi grow at comparatively slow rates , are requiring several days to weeks to form macroscopicallyvisible colonies. Usually, the growth will spread over the entire culture plate .Fungi Characteristic1. Fungi produce spores on brightly colored aerial hyphae.2. The fungi have two form; molds and yeast.3. Most fungi grow best at room temperature 25oC .4. The basic medium for the culture of many molds (multicellular, filamentous fungi ) is sabourauddextrose agar.5. The high sugar concentration and low pH (5.6) of the fungus medium make it unsuitable for thegrowth of most bacteria, thus guarding against contamination -fungi grow well at pH 5.6 moldcolonies may be examined directly in culture with a dissecting microscope.6. It is better to teach away apportion of the growth and place it on a slide with a drop of water or stain( a wet - mount) . An alternative method is a slide culture. the latter is more advantageous becauseone is able to study the growing mold and identify specific structures without disturbing the culture.The macroscopic aggregation (colony) of mold cells is called thallus,7. Thallus is composed of mass of strands called a mycelium, each strand is ahypha.8. vegetative hyphae grow on the surface of culture media, they form aerial hyphae, andreproductive hyphae (that bear asexual reproductive spores or conidia).9. The hyphae that grow below the surface of culture media are called rhizoidal hyphae.10. The hyphal strand of some molds may be separated by across wall called a septum. hyphae thatcontain septa are called septate hyphae. Molds with hyphae that lack septa are calledcoenocytic hyphae.11. molds grow best at temperature 25oC (in lab), while the yeast grow best at temperature 37oC (inhuman)12. Some fungi have two form in (the same fungus body); molds and yeast called dimorphic fungous13. The hyphal strand which carry conidia called conidiaphora, while the hyphal strand which carrysporangia called sporangiaphora. The spore inside the conidia and sporangia14. Fungi reproductive by sexual spore and asexual spore
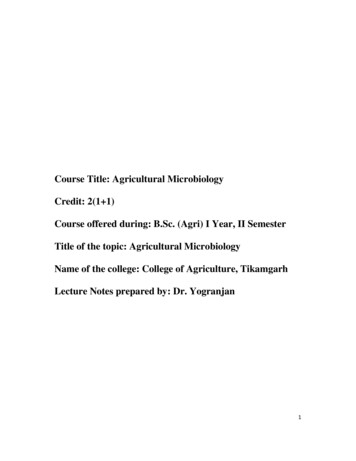
Lab:3(Parasitology)The parasites are classified as three phyla into1. phylum: protozoa2. phylum: platyhelminthus3. phylum: nematodaClasses of Protozoa:Type of locomotion of organelle has been used to divide these into four major classes:1. Rhizopods (amoebae): Entamoeba histolytica& Entamoeba coli2. Ciliaphora : Blantidium coli3. Mastigophora or flagellated: Giardia lamblia, Trichomonas vaginalis, Leishmania &Trypanosoma4. Sporozoa: Plasmodium, Toxoplasma gondii1. Class: Rhizopods (amoebae): Entamoeba histolytica& Entamoeba coliEntamoeba histolyticaTrophozoitesThe trophophozoite exhibits rapid, unidirectional, progressive movement, achieved with the help of fingerlike hyaline pseudopods. The single nucleus typically contains a small and central Karyosome. Variants ofthe karyosome include eccentric or fragmented karyosomal material. The peripheral chromatin is typicallyfine and evenly distributed around the nucleus in a perfect circle. The E. histolytica trophozoite finelygranular cytoplasms, Red blood cells in the cytoplasm are considered diagnostic because E. histolytica is theonly intestinal ameba to exhibit this characteristic. Bacteria, yeast, and other debris may also reside in thecytoplasm, but their presence, however, is not diagnostic.Even peripheral chromatinIngested RBCPseudopodiaCentral karyosomeCytoplasmFig. (1): Entamoeba histolytica trophozoite.
The spherical to round cysts of E. histolytica are typically smaller than the trophs, measuring. Thepresence of a hyaline cyst wall helps in the recognition of this morphologic form. Young cystscharacteristically contain unorganized chromatin material that transforms into squared or round – endedchromatoid bars in order cysts. The chromatoid bars may or may not be present in mature cysts. A diffuseglycogen mass is also usually visible in young cysts. As the cyst matures, the glycogen mass usuallydisappears. One to four nuclei are usually present. The mature infective cyst is quadri nucleated (containingfour nuclei). The cytoplasm remains fine and granular. Red blood cells, bacteria, yeast, and other debris arenot found in the cyst stage.Central karyosomeKaryosomeChromatoid BarCytoplasmFig. (1): Entamoeba histolytica trophozoite.Life cycleOnce the infective stage is ingested, excystation occurs in the small intestine. As a result of the nucleardivision, a single cyst produces eight motile trophozoites. These motile amebae settle in the lumen of thelarge intestine, where they replicate by binary fission and feed on living host cells. On occasion, trophzoitesmigrate to other organs in the body, such as the liver, and may cause abscess formation. Encystation occursin the intestinal lumen, and cyst formation is complete when four nuclei are present. These infective cystsare passed out into the environment in human feces and are resistant to a variety of physical conditions.Survival in a feces contaminated environment for up to a month is common.Clinical symptomsAmebiasis, an infection of the intestine or liver by an ameba, often Entamoeba histolytica. The amebae arepresent in food or water that has had contact with infected feces. Amebic dysentery, intestinal amebiasis.An inflammation of the intestine caused by Entamoeba histolytica. Symptoms are frequent, loose stoolsflecked with blood and mucus. An amebic abscess often accompanies amebic dysentery.Laboratory diagnosisStool examination is the method of choice for recovery of E. histolytica trophozoites and cysts. Throughusing wet preparations and permanent staining techniques on a suspected stool. When E. histolytica issuspected but not recovered in stool samples. Other laboratory tests including serological procedures may beutilized such methods currently available include Enzyme –Linked Immunosorbent Assay (ELISA).
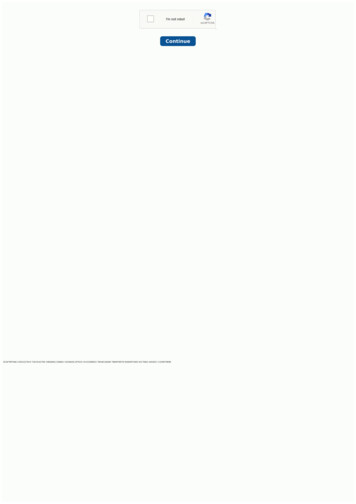
Entamoeba coliTrophozoiteThe trophozoite is equipped with blunt pseudopods and exhibits sluggish, nonprogressive motility. Thesingle nucleus is easily recognizable. In unstained preparations, the karyosome and the peripheral chromatinappear as refractile structures . The nuclear structures are enhanced when the trophozoites are stained . Thetypical nucleus consists of a large , often irregularly shaped karyosome that is eccentrically located . Thekaryosome is surrounded by unevenly distributed peripheral chromatin that varies in size and becomesapparent with addition of stain. Vacuoles, often containing bacteria , are commonly seen in the coarselygranulated cytoplasm . In contrast to E. histolytica, red blood cell inclusions do not occur.CytoplasmVacuolePseudopodbacteriaEccentric karyosomeFig. ( 3 ) : Entamoeba coli trophozoiteCystA thick cell wall surrounded the round to spherical cyst . As with the trophozoite , the cyst nuclei are readilydiscernible . One to eight nuclei with the typical nuclear features may be seen in unstained as well as stainedpreparations. Occasionally, large cysts containing 16 or more nuclei may be present . The granularcytoplasm may contain thin chromatoid bars, often with pointed to splintered ends. The glycogen mass maydisplace the nuclei present to opposite ends of the cyst.Cyst WallChromatoidCytoplasmbarsEccentric KaryosomeFig. ( 3 ) : Entamoeba coli cyst
Life cycleLife cycle of E. coli is similar to E. histolytica life cycle with the exception of difference in cyst nucleusnumbers.Clinical symptomsInfections with E. coli are usually asymptomatic.Laboratory diagnosisGeneral stool examination is the method of choice for recovery of E. coli trophozoites and cysts. Thepresence of E.coli suggests ingestion of contaminated food or drink. The technologist should thereforeexamine such preparations carefully for the presence of pathogenic parasites in addition to thenonpathogenic E. coli.Table showing the comparison between trophozoite of E. histolytica& E. colicharacteristicTroph. of E. histolyticaTroph. of E. coliNo. of nucleiOneoneKaryosomeSmall& centeralLarge irregular shape, eccentricPeripheral chromatinFine& evenly distributedCoarse& unevenly distributedCytoplasmFinely granularCoarse& often vacuolatedCytoplasmic inclusionIngested RBCBacteria, other debrisMotilityProgressive,pseudopodiafingerlikeNon Progressive, blunt pseudopodiaTable showing the comparison between cysts of E. histolytica& E. coliCharacteristiccyst of E. histolyticacyst of E. coliShapeSpherical to roundSpherical to roundNo. of nucleiOne to fourOne to eightKaryosomeSmall& centeralLarge irregular shape, eccentricPeripheral chromatinFine& evenly distributedCoarseCytoplasmFinely granulargranularCytoplasmic inclusionChromatoid bars, rounded Chromatoid bars, rounded with pointedends, diffuse glycogen massends, diffuse glycogen mass
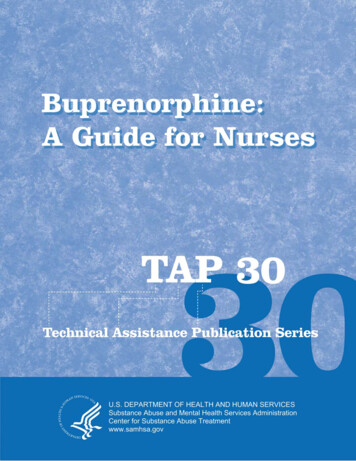
L4:Balantidium coliTrophozoitesConsidered as the largest protozoan known to humans, the typical Balantidium coli trophozoite my measurefrom 28 μm to 152 μm in length, with an average length of 35 to 50 μm. The average trophozoite width isapproximately 40 μm but may range from 22 μm to 123 μm. The ovoid to sac – shaped. B. coli trophozoitetapers at the anterior end. The organism typically exhibits rotary, boring motility. The trophozoite containstwo nuclei. The micronucleus is located adjacent to the macronucleus. The micronucleus is often notreadily visible, whereas the macronucleus may often appear as a hyaline mass, especially in unstainedpreparations. Two contractile vacuoles are located in the granular cytoplasm. In addition, the cytoplasm mayalso contain food vacuoles, as well as ingested microbes (bacteria). The trophozoite is equipped with a smallcytosome. A layer of cilia surrounds the organism, which serves as its means of nucleusMicronucleusCiliaVacuoleFig. ( 1 ) : Balantidium coli trophozoite.Table ( 1 ) : Balantidium coli trophozoite : Typical characteristicsSize rangeMotilityNumber of nucleiOther features28 to 152 μm in length 22 to 123 μm wideRotary, boringTwo : Kidney shaped macronucleus, Small spherical micronucleusOne to two visible contractile vacuoles. may contain bacteria.Small cytosome present. Layer of cilia around organismCystAveraging in size from 52 μm, the subspherical to oval. B. coli cyst may measure from 43 μm to 66 μm.Although the cyst technically contains both the macronucleus and micronucleus, the micronucleus may notbe observed in wet or permanent preparations. One or two contractile vacuoles may be visible, particularlyin young unstained cysts. A double – protective cyst wall surrounds the organism. A row of cilia may bevisible between the two cyst wall layers in unstained young cysts. Mature cysts tend to lose their cilia.Stained cysts typically reveal only the macronucleus, the other structures are not usually apparent.
CiliaCyst wallMacronucleusMicronucleusContractilevacuoleFig. ( ) : Balantidium coli cyst.Table (2 ) : Balantidium coli cyst : Typical characteristicsSize rangeNumber of nucleiOther features43 to 66 μm.Two : Kidney shaped macronucleus, usually present and small, sphericalmicronucleus, may not be observableOne to two visible contractile vacuoles in young cysts. Double cyst wallRow of cilia visible in between cyst wall layers of young cystsLife cycleHuman infection with B. coli is initiated upon ingestion of infective cysts in contaminated food or water .unlike that of E. histolytica , multiplication of the B. coli nuclei does not occur in the cyst phase . followingexcystation in the small intestine , the resulting trophozoites take up residence and feed primarily in thececal region and terminal portion of the ileum, as well as in the lumen, mucosa, and submucosa of the largeintestine. The multiplication of each trophozoite occurs by transverse binary fission, from which two youngtrophozoites emerge. The B. coli trophozoites are delicate and do not survive in the outside environment.Encystation occurs in the lumen. The resulting cysts mature and ultimately become the infective form fortransmission into a new host. These cysts may survive for weeks in the outside environment.
Clinical symptomsBalantidiasis. Symptomatic patients may experience a variety of discomforts, ranging from mild colitis anddiarrhea to full – blown clinical balantidiasis, which may often resemble amebic dysentery. In this case,abscesses and ulcers may form in the mucosa and submucosa of the large intestine followed by secondarybacterial infection. Acute infections are characterized by up to 15 liquid stools per day containing pusmucus, and blood. Patients who suffer from chronic infections may develop a tender colon, anemia,cachexia, and occasional diarrhea, alternating with constipation. Balantidium coli has been known to invadeareas other than the intestine, such as the liver , lungs, pleura, mesenteric nodes, and urogenital tract.Laboratory diagnosisLaboratory diagnosis of Balantidium coli is accomplished by examining stool specimens for the presence oftrophozoites and cysts. Stools from infected patients experiencing diarrhea are more likely to contain B. colitrophozoites. Although it does not occur frequently, suspicious formed stools may contain cysts .sigmoidoscopy material may also reveal B. coli organisms when collected from patients suffering fromsigmoidorectal infection .L5: A:Class:Mastigophara(Flagellates)Giardia lambliaTrophzoiteThe typical Giardia lamblia trophozoite ranges from 8 to 20 μm in length by 5 to 16 μm in width. Theaverage G. lamblia trophzoite, however, measures 10 to 15 μm long. The G. lamblia trophzoite is describedas pear or tear – drop in shape. The broad anterior end of the organism tapers off at the posterior end. The G.lamblia trophozoite characteristically exhibits motility that resembles a falling leaf. The trophzoite isbilaterally symmetrical, containing two ovoid to spherical nuclei, each with a large karyosome, usuallycentrally located. The trophozoite is supported by an axostyle made up of two axonemes. Two slightlycurved rod – like structures, known as median (parabasal) bodies, sit on the axonemes posterior to thenuclei .The typical G. lamblia trophzoite has four pairs of flagella. One pair of flagella originates from theantrior end, and one pair extends from the posterior end. The remaining two pairs of flagella are locatedlaterally, extending from the axonemes in the center of the body. The G. lamblia trophozoite is equippedwith a sucking disc. Covering one half to three quarters of the ventral surface, the sucking disc serves as thenourishment point of entry by attaching to the intestinal villi of an infected human .Nucleiparabasal bodiesFlagellaFig. ( 1 ) : Giardia lamblia trophzoite .AxonemesAxostyle
Table (1) : Giardia lamblia trophozoite : Typical characteristicsSize range8 to 20 μm long 5 to 16 μm wideShapePear / tear drop“ Falling leaf “MotilityAppearanceNucleiBilaterally symmetricalTwo ovoid – shaped , each with a large karyosome No peripheral chromatinFour pair , origination of each : One pair anterior end One pair posteriorend Two pair central laterallyTwo median bodies , two axonemes , sucking discFlagellaOther structureCystThe typical ovoid G. lamblia cyst ranges in size from 8 to 17 μm long by 6 to 10 μm wide, with an averagelength of 10 to 12 μm . The colorless and smooth cyst wall is prominent and distinct from the interior of theorganism. The cytoplasm is often retracted away from the cyst wall, creating a clearing zone. Thisphenomenon is especially possible after being preserved in formalin. The immature cyst contains two nucleiand two median bodies. Four nuclei, which may be seen in iodine wet preparations as well as on permanentstains, and four median bodies are present in the fully mature cysts. In addition, mature cysts contain twiceas many interior flagellar structures.NucleiCystparabasal bodieswallCytoplasmbeginning toretracted fromcyst wallTable (2) : Giardia lamblia cyst : Typical characteristicsSize range8 to 17 μm long , 6 to 10μm wideShapeOvoidNucleiImmature cyst – 2, Mature cyst – 4Central karyosomes, No peripheral chromatinCytoplasmOther structuresRetracted from cell wallMedian bodies , two or four , Interior flagellar structures
Life cycleUpon ingestion, the infective G. lamblia cysts enter the stomach. The digestive juices, particularly gastricacid, stimulate the cysts to excyst in the duodenum. the resulting trophozoites become established andmultiply approximately every 8 hours via longitudinal binary fission . The trophozoites feed by attachingtheir sucking discs to the mucosa of the duodenum. Trophozoites may also infect the common bile duct andthe gallbladder. Changes resulting in an unacceptable environment for trophozoite multiplication stimulateencystation, which occurs as the trophozoites migrate into the large bowel. The cysts enter the outsideenvironment via the feces and may remain viable for as long as 3 months in water.Clinical symptomsGiardiasis (“Traveler’s Diarrhea”). Symptomatic infections with Giardia lamblia may be characterizedby a wide variety of clinical symptoms, ranging from mild diarrhea, abdominal cramps, anorexia, andflatulence to tenderness of the epigastric region steatorrhea, and malabsorption syndrome. Patients sufferingfrom a severe case of giardiasis produce light – colored stools with a light fat content that may be caused bysecretions produced by the irritated mucosal lining. Fat soluble vitamin deficiencies, folic acid deficiencies,hypoproteinemia with hypogammaglobulinemia, and structural changes of the intestinal villi may also beobserved in such cases.Laboratory diagnosisThe specimen of choice for the traditional recovery technique of G. lamblia trophozoites and cysts is stool.In addition, doudenal contents obtained by aspiration, as well as upper small intestine biopsies, may also becollected for examination. Several other diagnostic techniques are available for identifying G. lamblia,including Countercurrent Immunoelectrophoresis (CIE), which detects the G. lamblia fecal antigen,immunofluorescence and Enzyme – Linked Immunosorbent Assay (ELISA).L7: Trichomonas vaginalisTrophozoitesAlthough typical Trichomonas vaginalis trophozoites may reach up to 30 μm in length the average length, is8 to 15 μm long. The trophozoites may appear ovoid, round, or pearlike in shape. Rapid, jerky motility isaccomplished with the aid of the organism’s four to six flagella, all of which originate from the anterior end.Only one of the flagella extends posteriorly. The flagella may be difficult to find on specimen preparations.The characteristic undulating membrane is short, relatively speaking extending only one half of the bodylength. The single nucleus is ovoid, nondescript, and not visible in unstained preparations. Trichomonasvaginalis trophozoites are equipped with an easily recognizable axostyle. That often curves around thenucleus and extends posteriorly beyond the body. Granules may be seen along the axostyle. Fig. (1) .NucleusFour anterior flagellaUndulatingmembrane(halfof body length)Granules along axostyle commonOne posterior flagellumFig. (1): Trichomonas vaginalis trophzoite.
Table (10) : Trichomonas vaginalis trophozoite : Typical characteristicsShapeOval or round to pearMotilityNucleiRapid , jerkyFlagellaAll originating anteriorly; Three to five extending anteriorly, One extendingposteriorlyUndulating membrane extending half of body lengthProminent axostyle commonOther featuresOne, ovoidCyst; There is no known Trichomonas vaginalis cyst stage.Life cycleTrichomonas vaginalis trophzoites reside on the mucosal surface of the vagina in infected women. Thegrowing trophozoites multiply by lonitudinal binary fission and feed on local bacteria and leukocytes. TheTrichomonas vaginalis trophozoites thrive in a sligtly alkaline or slightly acid PH environment, such as thatcommonly seen in an unhealthy vagina. The most common infection site of T. vaginalis in males is theprostate gland region and the epithelium of the urethra. The detailed life cycle in the male host is unknown.Clinical symptomsTrichomoniasis a vaginal infection caused by the microorganism Trichomonas vaginalis, marked byitching, burning, and frothy, pale yellow to green,bad-smelling vaginal discharge. With long-terminfection all symptoms may disappear, although the organisms are still present. In men, infection is usuallywithout symptoms but may be shown by a continuing or recurrent irritation of the urethra. Infection iscarried by sexual intercourse, rarely by moist washcloths, or, in newborns, by passage through the birthcanal. Diagnosis is by microscopic examination of fresh substances released through the vagina. Treatmentis by metronidazole given by mouth. Reinfection is common if sexual partners are not treated at the sametime.Laboratory diagnosisTrichomonas vaginalis trophozoites may be recovered utilizing standard processing methods in spun urine,vaginal discharges, uretheral discharges and prostatic secretions. Although permanent stains may beperformed, examination of saline wet preparations is preferred in many instances.Trichomonas tenaxTrophozoitesThe typical Trichomonas tenax trophozoite is described as being oval to pear shaped and measuring 5 to 14μm long, with an average length of 6 to 9 μm. The single ovoid vesicular nucleus is filled with severalchromatin granules and is usually located in the center anterior portion of the organism. The T. tenax
trophozoite is equipped with five flagella, all of which originate at the anterior end. Four of the flagellaextend anteriorly and one extends posteriorly. An undulating membrane that extends two thirds of the bodylength and its accompanying costa typically lie next to the posterior flagellum. A thick axostyl runs alongthe entire body length, curving around the nucleus, and extends posteriorly beyond the body of the organism.a small anterior cytosome is located next to the axostyle opposite the undulating membrane.Cyst There is a known cyst stage of T. rflagellumPosteriorAxostyleUndulating membraneFig. (1): Trichomonas tenax trophzoite.(Two thirds of body length)Table (1) : Trichomonas tenax trophozoite : Typical characteristicsShapeNucleiFlagellaOther structuresOval to pearOne, vesicular filled with chromatin granules, ovoidFive total, all originating anteriorly: four extends anteriorly, Oneextends posteriorlyUndulating membrane extending 2/3 of body length Thick axostyleSmall anterior cytosome opposite undulating membrane.Life cycleTrichomonas tenax trophozoites survive in the body as mouth scavengers that feed primarily on localmicroorganisms. Located in the tartar between the teeth, tonsillar crypts pyorrheal pockets, and gingivalmargin around the gums, T. tenax trophozoites multiply by lonitudinal binary fission. These trophozoites areunable to survive the digestive process.Clinical symptomsThe typical Trichomonas tenax infection does not produce any notable symptoms. On a rare occasion, T.tenax has been known to invade the respiratory tract, but this appears to have mainly occurred in patientswith underlying thoracic or lung abscesses of pleural exudates.Laboratory diagnosisThe specimen of choice for diagnosing Trichomonas tenax trophozoite is mouth scrapings. Microscopicexamination of tonsillar crypts and pyorrheal pockets of patients suffering from T. tenax infections oftenyields the typical trophozoites. Tartar between the teeth and the gingival margin of the gums are the primaryareas of the mouth that may also potentially harbor this organism. T. tenax may also be cultured ontoappropriate media .
L8: B:Class Haemoflagellates: Leishmania & Trypanosoma -Leishmania:A. L.donovani: causes visceral Leishmianiasis, Kalaazar and Dum Dum fever. Spleenomegaly &hepatomegaly. Parasite in human present in amastigote form, while in the insect (Sand fly) promastigote.B. L.tropica : causes tropic sore or Baghdad boil, oriental sore and cutenaeousLeishmianiasis, the insect transport L.tropica is sand fly.C. L. braziliensis : causes Mucocutaneous leishmaniasis. Trypanosoma: The cell of this genus is tall with one central nucleus and the motile generator located in theterminal of parasite.1. The flagellate belong to these two genus pass through the life cycle; the live cycle between two host:vertebrate host (terminal host like human)and arthropod host (mediated host like the fly) in many stages withdifferent shapes, through the shape of the body, presence of flagellate or absent, the shape locate of motilegenerator and the presence of waved membrane or absent ,as following:A.Amastigote: the parasite circular or ovum in shape,the nucleus lies near the center and it in front of itpresent motile generator which extend short flagella from it and have not waved membrane.B. Promastigote: the body is spindle with nucleus in the center and motile generator located near thebeginning of the body arise a flagellate from generator extend out of the body and have not waved membrane.C. Epimastigote: the body is tall and motile generator lies in front of the nucleus that move little away fromthe center of the body and arise on it flagellate that connectwith the body and with the waved membranetherefore extend with free end.D. Trypomastigote:The body is spindle and the nucleus lies in the center,the motile generator lies in the lastpart of the parasite and arise from it a flagellate extend along the external adage to the waved membrane andthe end of flagella is free.Note:the parasite that belong to Leishmania pass through the life cycle in amastigoteand promastigote forms while Trypanosoma pass through the life cycle with all forms. Trypanosoma:T.gambiense: causing sleeping disease to human and the mediated host is Tse Tse fly.T.cruzi: cause chagas disease, American trypanosomiasis.
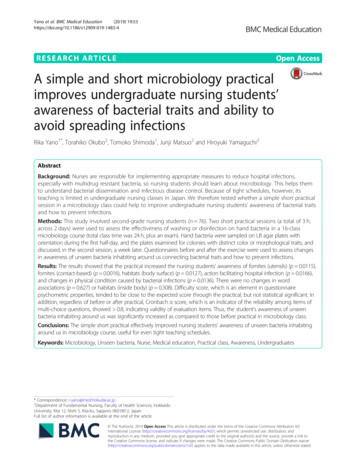
Parabasal bodyKinetoplastBelpharoplastAxonemeNucleusFig. ( ) : Leishmania tropica AmastigoteBelpharoplastNucleusParabasal bodyFlagellumAxonemeKinetoplastFig. ( 2 ) : Leishmania PromastigoteFig. ( 3) trypomastigoteLife cycleSandflies of the genera Phlebotomus are responsible for transmitting Leishmania tropica promastigotes intounsuspecting humans via blood meal, resulting in a skin bite. The promastigotes quickly invade thereticuloendothelial cells and transform into amastigotes, which actively reproduce, causing tissue destruction
reproduction and invasion of additional cells then occurs . The skinand mucous membrane areas of the bodyare primarily affected. The amastigote serves as the infective stage for the sandfly. Upon ingestion, during ablood meal of an infected human, the amastigotes transform back into promastigotes in the fly midgut.These promastigotes multiply, and the resulting developed forms eventually migrate into the salivary glandof the fly, where they are ready to be transferred to a new human during a blood meal. Thus the cyclerepeats itself.Fig. ( ) : Leishmania Life cycle .Clinical symptomsCutaneous Leishmaniasis. Also known as Old World leishmaniasis, Oriental sore, and Baghdad or Delhiboil, cutaneous leishmaniasis is characterized by one or more ulcers containing pus that generally self – heal.Infected patients initially develop a small red papule , located at the bite site , that a typcally 2cm or more indiameter and may cause intense itching . the incubation time and the appearance of the papule vary witheach subspecies . diffuse cutaneous leishmaniasis (DCL) occurs especially on the limbs and face whenimmune response fails to take place .Laboratory diagnosis1. thick blood film (amastigot). 2. skin test: is used to measure delyed hypersensitivity.3. detection of antibody by ELISA. 4. can be cultured on NNN media (Novy Macneel Nicolle).
L9: 4-Class: SporozoaA:Malaria (Plasmodium species)a. Plasmodium falciparum causes malignant tertian malariab. P. malariae: causes Quartean malariac. P. vivax: causes benign tertian malariad. P. ovale: causes benign tertian malariaMalaria is an acute infectious disease of the blood, caused by one of four species of the protozoal genus,. P.falciparum accounts for some fifteen percent of all malaria cases, and P. vivax for eighty percent of malarialcases.The plasmodial parasite is transmitted to humans through the bite of a female Anopheles mosquito, or by aninfected, blood-contaminated, needle.Sporozoans reproduce asexually in human cells by a process called schizogony, in which multiple nucleardivisions are followed by envelopment of the nuclei by cell walls producing merozoites (ring stage). These,in turn, become trophozoites. Sexual reproduction occurs in the mosquito, where new spores (sporozoites)are formed process called sporogony. Schizogony (asexually in human; intermediated host),sporogony(Sexual reproduction in the mosquito; definitive host)Diagnosis depends on detection of the parasite inside red blood cells. Thick blood smears stained withGiemsa stain provide the most sensitive visual test. Thin blood smears, in which more detail can bediscerned, are used to determine the species involved, which is important in planning a course of therapy.Plasmodium vivaxRing formThe cytoplasmic ring of the typical P. vivax ring form measures approximately one third diameter of the redblood cell in which it resides. A single chromatin dot serves as the connecting point of this delicate ring. Avacuole is visible inside the ring. The parasite may be first visible as a crescent – shaped mass at the outeredge of the red blood cell .Developing trophozoitesAlthough remnants of the cytoplasmic ring may be visible, the parasite takes on more of an irregularlyshaped ameboid appearance. Asingle large chromatin dot is present among the cytoplasmic material.thevacuole remains visible and basically intact until the late stage of devel
Practical Microbiology for Nurses 2018 By A.Professor Dr. Nada Khazal K. Hindi Dr.Hiba Jassim Dr.Mays Hadi . lab:1 Fungi Fungi grow at comparatively slow rates , are requiring several days to weeks to form macroscopically visible colonies. Usuall