Transcription
Community-Based Health Planning and Services (CHPS)C o m m u n i t y H e a l t h O f fi c e r Training ManualC O M M U N I T Y H E A LT H O F F I C E RTraining Manual( F a c i l i t a t o r ’s G u i d e )lumeVo1Volume 1ENTPMELOAL DEVFROM THE AMERICAN PEOPLEYour Health Our ConcernMNDIDWIVESGHANAIUNAONYour Health Our ConcernCHPS-TA CENTREMINISTRY OF HEALTH/GHANA HEALTH SERVICE NATIONAL HEALTH LEARNING MATERIALSUCOSAPMOTIUNENTIUNGHO ANPM AENRNTICHPS-TAGHSICERVINTECHPS-TAYUSAIDAL T HHESETICERVS TAT E S A GPEOPLEFROM THE AMERICANEEDGHSSEELNCAL DEVICERVFROM THE AMERICAN PEOPLEONUSAIDGHSUSAIDAL T HHESEUSAIDYELENCAAL DEVTIARNONRNINTETIUSAIDINTEYUSAIDNCTS TAT E S A GEEDS TAT E S A GGHANAAL T HHEDTEYour Health Our Concern
Community-Based Health Planning and Services (CHPS)COMMUNITY HEALTH OFFICERTraining Manual(FACILITATOR’S GUIDE)Volume1ENTPMPR FOR GHANA ESOYourTECHealthOur &ConcernTI IUNENTIUSAIDYour Health Our ConcernCHPS-TAGHSICERVELSEAL DEVAL T HHEGHFROM THE AMERICAN PEOPLESICERVAONYRNTIUSAIDSETEGHSYour Health Our ConcernAL T HHEES STATES AGEDNCGHSINTECHPS-TAE,CHPS-TAEALTHHIDWIVMNDICERV UNCILSE COUNCHPS-TACA RANAL DEVOAFROM THEPEOPLET I AMERICANFROMTHE AMERICAN PEOPLEELOELAL DEUSAIDFROM THE AMERICAN PEOPLELVEICERVRNUSAIDUSAIDYAAL DEVUSAIDRNRNONTAT E S AGEDSINTEINTETITENCYUSAIDNCTAT E S AGEDSONSEINTETITEYUSAIDNCTAT E S AGEDSGHANAAL T HHETEYour Health Our ConcernMNDIDWIVESRVICENURSESAERVICENURSESE,E,PR FOR GHANA ESOTE C TI ON &PR FOR GHANA ESOTE C TI ON &E,RVICIDWIVESCA RCA RPR FOR GHANA ESOTE C TI ON &MNDUNCILCOAIDWIVESUNCILCONURSESMNDUNCIL CARCOAMINISTRY OF HEALTH/GHANA HEALTH SERVICE NATIONAL HEALTH LEARNING MATERIALS CENTRE
2009 The Population Council, Inc./Ministry of Health/Ghana Health ServiceEditorial OfficeNational Health Learning Materials CentreHuman Resources Development DivisionMinistry of Health/Ghana Health ServiceP.O. Box 1908, Kumasi, GhanaTel: 233 51 29434Editors: Andrew Adjei Druye, Justice Acheampong, Bridget Brenya-Boateng,Mabel Asafo Kissiwah, Joseph Sarfo Antwi, Solomon Anum-Doku, Alice Baffoe,Ken Gbeve, Amerley A. OllennuCover Design: Kwabena AgyepongDesign: Kwabena Agyepong, Francis K. N. Nunoo, Mawuli Albert GadzanakiLay out: Kwabena Agyepong, Francis K. N. Nunoo, Alex Ronald ArhinAll rights reserved. No part of this publication may be reproduced, stored inretrieval system, recording and/or otherwise, without the permission of thePopulation Council or Ministry of Health/Ghana Health Service, Ghana.ISBN 9988-8481 6 3Legal DisclaimerCare has been taken to confirm the accuracy of the information presentedaccording to generally accepted practices. However, the authors, editors andpublishers are not responsible for errors and omissions or for any consequencesfrom application of the information in this book and make no warrantyexpressed or implied, with respect to the content of the publication.DisclaimerThis publication was made possible through support provided by the PopulationCouncil/ Community-based Health Planning and Services Technical AssistanceCooperative Agreement, US Agency for International Development/Ghana,under the terms of Award No. USAID 641-A-00-04-00270. The opinionsexpressed herein are those of the author(s) and do not necessarily reflect theviews of the U.S. Agency for International Development.The CHPS-TA partners are Population Council, EngenderHealth, AmericanCollege of Nurse Midwives (ACNM) and the Centre for Development ofPeople (CEDEP).ii
AcknowledgementsAcknowledgementsWe are grateful to the many individual and organization that provided consultation, suggestion,technical assistance and funding for the production of this document.Special thanks to PRIME II for developing the original manual from which these workbookshas adopted. USAID AND CHPS-TA for supporting the scaling up of the CHPS programme inGhana. We are most grateful to the following individuals for the roles they played in developingthese materials.Agyeman Badu AkosaFormer DG - GHSElias K. SoryDG-GHSKen SagoeHRDD - GHSSaid Al-HusseinHFDD - GHSKobina BainsonCHPS - TACHPS - TABarbara JonesIrene B. BangpouriCHPS - TACaronline TettehCHPS - TAIsabella RocksonCHPS - TANow to the staff of the Health learning Materials Centre, we say big thank you for technicalsupport in the manual development.Special mention go to the technical reviewers who ensured that the materials were practical,accurate, current and acceptable to the intended users. They are:Stella DeiwahA. K. AnkuvieTheresa G. MensahSolomon Anum-DokuJustice AcheampongAndrew Adjei DruyeSamuel Kissi BoatengMawuli Albert GadzanakiBridget Brenya-BoatengFrank Ohene KankamVera GaituEllen Sarpong-AkorsahComfort AgbadjaDHD-Kwahu NorthDHD-Kwahu NorthDHD-Birim NorthNHLMC- KumasiNHLMC-KumasiNHLMC-KumasiNHLMC – KumasiNHLMC – KumasiNHLMC – KumasiNHLMC – KumasiRHD- Volta RegionRHD-Volta RegionRHD-Volta Regioniii
Joseph K. SampsonEmmanuel Edum-KankamElizabeth CorneyBeatrice KunfahPhoebe BalaCharlotte EninfulPatricia AntwiYaw Brobbey MpianiivDHD-Sefwi WiawsoRHTS, KintampoDHD-Bia DistrictDHD-Jirapa Lambusie DistrictDHD-Wa West DistrictCHNTS WinnebaDHD-GomoaGHS, HQ , Accra
ForewordForewordThe levels of health care provision are clearly defined and articulated in the Ghana HealthService and Teaching Hospitals Act, 1996 (Act 525). It is a fact that if the health sector is tocontribute to the achievement of the Millennium Development Goals in Ghana, then there isthe need for a paradigm shift in health services provision from over concentration on curativeand institutional care to a more community-based level or close-to-client health services deliverywith household and community involvement.The Community-based Health Planning and Services (CHPS) initiative is one of the newparadigm shifts which have been adopted to re-orient and relocate health services from clinical tocommunity levels, which is contributing to the realization of the goals of primary health care.From the initial trials in Nkwanta and Juaboso Bia district, the CHPS initiative has now becomea national policy in health care delivery. All districts are in the process of implementing thescheme and the training of personnel needed is on going. The effectiveness of the training ofthese personnel for CHPS depends on the availability of appropriate materials. It is for thisreason that this training manual has been developed to guide and support CHO training.The manual consists of fourteen modules which have been organized into three volumes. Themanual which has been tried and tested over a period of five years will continue to be useful inthe training of the personnel needed for CHPS. Over the period, the manual has been reviewedand current issues such as the Millennium Development Goals, poverty reduction, mental healthand regenerative health and nutrition have been integrated.It is my hope that this manual will guide health service providers in improving and expandingCHPS implementation.Dr. Elias SoryDirector General, Ghana Health ServiceMay, 2008v
PrefaceThe Community-based Health Planning and Services (CHPS) is the Government of Ghana’sstrategy to bring quality health care to the door step of the people. The government recognizesthat the main producers of health are individuals and households. By involving individuals andhouseholds in planning and delivering health care CHPS aims to establish sustainable systemsfor improving the community’s health. Community Health Officers serve as the link betweenthe sub-district and the community, working through health extension workers and communityvolunteers.Since CHPS became a national policy the regions and districts have developed various trainingprogrammes and trained Community Health Nurses as CHOs; however, these trainingprogrammes have not been structured as a coherent national training programme on CHPS.Thus, there is the need to develop a structured training programme for improving the quality ofhealth services delivered in CHPS zones.The training package comprises the CHO Manual (Facilitators’ Guide) and the CHO Workbook.The facilitators guide are to be used by facilitators and CHO workbook are for CHO. However,the two documents are complementary to each other. The development of the CHO manual(Facilitator’s Guide) and CHO Workbook has been informed by the job description of the CHOas well as changes in health policies both globally and nationally.There are two objectives for writing the CHO training manual and workbook. First, it is astandard in-service training manual that health managers, CHO Supervisors and trainingfacilitators can use to orient newly qualified community health nurses as well as train existingCHOs to improve service delivery in CHPS. Second, the documents should serve as a resourcefor use by CHOs to improve the management of CHPS zones and improve the quality of servicesdelivered.The CHO Manual (Facilitator’s Guide) is in three volumes which cover the CHO’s work,including delivering reproductive and child health services, curative care, health promotionand prevention, and health care management. Volume one discusses the CHO’s work inthe community, including home visiting, behaviour change communication, and managingCHO activities. Volume two covers maternal and child health care, including familyplanning, antenatal care, safe emergency delivery, postnatal care and HIV/AIDS. Improvingimmunization, promoting good nutrition, disease control and management of common ailmentsand emergencies are important in reducing under-five and maternal mortality; therefore, thesesubjects have been covered in Volume three.Each module has module objectives and content. The content section is sub-divided into units,and each unit relates to the one of the objectives of the module. Each unit in the module startswith a Terminal Performance Objectives (TPO) followed by the topics.vi
How to use the Facilitator’s Guide and WorkbookHow to use the Facilitator’s Guide and WorkbookFacilitator’s GuideThe Facilitators’ Guide contains details of the suggested approaches and activities to enable youto facilitate each unit within the module. References have been provided, but as a facilitator, youare encouraged to consult other reference materials.Advance PreparationYou need to prepare ahead for facilitating each unit. Some of the preparations require gatheringvarious materials, preparing copies of case studies for distribution, session notes and othermaterials that may be needed. You may also need to contact chiefs and opinion leaders of thevarious sites that you intend to use as field visits sites. It is further advised that facilitators shouldmeet to discuss the mode of training and related issues before training starts.Facilitator-Participants’ InteractionAs a facilitator, you are encouraged to use interactive approach to enable your trainees achieveproficiency in applying the requisite skills. You also need to be as innovative as possible to enablethe trainee CHO to achieve the specified TPO. Even though facilitation approaches have beensuggested, you may use other approaches as you deem fit. Lectures and other less participatoryapproaches should be kept to a minimum. You should aim to involve the trainees as much aspossible in the process of skills transfer and acquisition.Periodic refresher training on specific modules using on-the job training (OJT) approaches mustbe organized for the CHO.Field VisitsThe training is to enable CHOs to attain proficiencies in the various skills needed for theirpractice. Therefore you should devote more time in the field to enable them have real hands-onexperience. Make arrangement for transport where necessary.Training Needs AssessmentThis should be conducted ahead of each training. Sample case studies have been prepared fordistribution to potential trainees before they arrive at the training site. Encourage trainees torespond to all the questions and also to complete the CHO Workbook before every session. Theinformation gathered from the use of the case studies, the CHO Workbooks, and the pre-testvii
scores will enable you tailor the training programme to enable maximum benefit to be obtainedby the CHOs.CHO WorkbookThe CHO Workbook contains the content organized as units as well as the activities, includingcase studies, role-plays, and discussion points. The CHO Workbook is similar to the Facilitators’Guide. However, the answers to the various questions and case studies have been deleted fromthe Workbook. This will enable the CHO learn the contents of the module on his/her own usingthe notes included as reference material. It will also enable the CHO use it to take notes duringtraining.Advance Preparation for CHO TraineesEach trainee should receive the CHO Workbook at the beginning of the in-service training.Trainees should be encouraged to read through the Workbook, reference notes and complete allthe assignments listed. The facilitator should also give the trainees a number of case studies tostudy and provide answers. Encourage trainees to consult the reference listed in the module aswell as any other reference materials that may be available to you. The case studies are meant toassess trainees’ knowledge of some procedures that they need to perform when they are in thefield. A pre-test should be conducted at the start of the training to complete the assessment oftrainees’ training needs.Participation in Training SessionsDuring the training, facilitators should interact closely with the trainees to maximize theacquisition of knowledge, appropriate attitudes and skills.Supervisory Visits and SupportRegular supportive supervision is encouraged after the training programme. You should receivesupervisory visits from your supervisor(s) to help you consolidate the skills you have acquiredfrom the training and improve your performance as CHO. Your supervision may organize Onthe Job Training (OJT) for you during these supervisory visits. These OJTs will be based on yourneeds as identified by yourself and your supervisor. It is therefore important to keep records ofyour experiences in the field and the cases that you encounter. This will enable you and yoursupervisor plan the OJTs effectively.viii
AbbreviationsAbbreviationsANCAnte natal careAPGARAppearance, pulse, grimace, activity, respiration -APHAnte-partum haemorrahageARTAnti-retroviral therapyAVSCAssociation of Voluntary Surgical ContraceptionBCCBehaviour change communicationBCGBacille Calmette-Guerin vaccineBFBlood filmBNIBasic needs incomeBPBlood pressureBTLBilateral tubal ligationCBACommunity-based agentCBDCommunity-based distributionC-COPEClient-oriented provider efficient serviceCDCommunicable diseaseCD1 or C.D.1Communicable disease form 1CDSCommunity decision systemCHCCommunity Health CompoundCHOCommunity Health OfficerCHPSCommunity-based Health Planning and ServicesCHVCommunity health volunteerCHWCommunity health workerCOCCombined oral contraceptiveCPIClient provider interactionCSMCerebro-spinal meningitisCWCChild welfare clinicDDHSDistrict Director of Health ServiceDHDDistrict Health Directorateix
xDHMTDistrict Health Management TeamDMPA/NET-ENDepot Medroxy Progrestone AcetateDOTDirectly observed HaemophilusGHSGhana Health ServiceHRDDHuman Resource Development DivisionIDSRIntegrated disease surveillance and responseIEC or IE&CInformation, education and communicationIMCIIntegrated management of childhood illnessesIPInfection preventionIPCInter personal communicationITNInsecticide-treated netIUDIntra uterine deviceIVIntravenousLBWLow birth weightLCDLiquid crystallized displayMAPMen as partnersMISManagement information systemsMOHMinisty of HealthMTCTMother-to-child- transmissionNGONon-governmental organisationNHLMCNational Health Learning Materials CentreNHRCNavrongo Health Research CentreOHPOverhead projectorOJTOn-the-job trainingOPVOral poliovirus vaccineORSOral rehydration saltPASPublic address systemPIDPelvic inflammatory diseasePLWHAPeople living with HIV and AIDS
AbbreviationsPNCPost natal careRCHReproductive and child healthRHMTRegional Health Management TeamRPRRapid Plasma Reagin TestRTIRespiratory tract infectionSCHNSenior Community Health NurseSDHTSub- District Health TeamSHEPSchool health education programmeSHISchool health inspectionSTDSexually transmitted diseaseSTGStandard treatment guidelinesSTISexually transmitted infectionTBATraditional birth attendantTPOTerminal performance objectivesTTTetanus toxoidVCTVoluntary counselling and testingVDRLVenereal Disease Reference LaboratoryVHCVillage health committeeVVMVaccine vial monitor5 W and HWho? What? When? Where? Why? and How?WHOWorld Health OrganisationWIFAWomen in fertile agexi
Table of ContentsAcknowledgementsForewordPrefaceHow to use the Facilitator’s Guide and WorkbookAbbreviationsThe Community-Based Health Planning and Services (CHPS) ConceptModule 1Unit 1Unit 2Unit 3Unit 4Managing Community Health Officer ActivitiesPreparing a Monthly Calendar for CHO ActivitiesMobilising Resources for Monthly CHO ActivitiesImplementing Planned CHO ActivitiesMonitoring and Evaluating Planned CHO Activities16121720Module 2Unit 1Unit 2Unit 3Home Visiting For Health ActivitiesPlanning and Preparing for Home VisitsConducting Effective Home VisitsConducting Effective School Hygiene Inspection39445157Module 3Unit 1Unit 2Supporting Community Health Volunteers (CHVs)Managing Supervisory ActivitiesProviding Technical Support to the CHVDuring Supervisory VisitsOrganising Regular Supervisory MeetingsManagement of Supplies and Logistics7176Unit 3Unit 4Behaviour Change CommunicationModule 4Unit 1Effective CommunicationUnit 2Behaviour Change ProcessUnit 3Inter-Personal Communication (IPC)/ CounsellingUnit 4Using Learning Aids (Teaching and LearningMaterials) 5
Table of ContentModule 5Working With CommunitiesUnit 1Getting To Know your CommunityUnit 2Conducting a Community Needs AssessmentUnit 3Mobilising Communities around Specific Health ActivitiesUnit 4Using Participatory Tools to SolveCommunity Health ProblemsReferences155159165170176201xiii
The Community-Based Health Planning andServices (CHPS) ConceptHealth Situation Post-independenceBringing basic health care services to all Ghanaians has been the major objective of theGovernment of Ghana. Since independence, the Government of Ghana has worked on improvinghealth care services by building large hospitals in cities and big towns and health centres insmaller towns and villages. While the hospitals satisfied the needs of the urban populations,many people in rural communities did not have access to even basic health services, becausethey lived far away from health facilities. Thus, a vast majority of the rural population was leftwithout any health services. As a result, children died from preventable diseases such as malaria,diarrhoea, measles, acute respiratory tract infection and cholera. Pregnant women also diedfrom complications because the danger signs were not recognized early enough, services wereunavailable or there was lack of transport, bad roads, or other difficulties.To improve access to health service, the Government introduced the outreach services. Selectedcommunities became outreach posts. Staff from the health centres travelled there on regularlyscheduled days to provide health care. The staff always returned to the health facility until thenext scheduled date. However, the outreach points did not improve access significantly. Why?Only those rural people who could go to the outreach point got access to health services.Origin of CHPSThe government decided to do something about the situation. The Ministry of Health askedcommunity members how they wanted health services to be delivered to them. The people saidthey wanted health services delivered at their doorstep and that they wanted to be involved in theprocess. Therefore, the Ministry chose Navrongo in the Kassena-Nankana district of the UpperEast region to test the various ways in which health services can be delivered close to the people.The pilot project was the Community-based Health and Family Planning Project.The Upper East region was the poorest region in Ghana. The Ministry therefore chose the UpperEast region because if the strategy worked among poor communities, it was likely to succeed inother parts of the country that were relatively better off. The Ministry provided a nurse who livedamong the people and attended to their health needs. The people also committed themselvesto support the programme by providing accomodation for the nurse. They also agreed to selecthealth volunteers to work with the nurse in addition to forming health committees to oversee thecommunity health care delivery system and supervise the volunteers.It is important to note that community members played a vital role in the Navrongo research.In spite of that, some questions remained at the back of the minds of both the health workersxiv
The Community-Based Health Planning and Services (CHPS) Conceptand community members. The Navrongo Health Research Centre was tasked to test the variousoptions and assess their effect on the health of the people. Five years later, all the questions wereanswered. The people reported that the community health nurses and the community volunteerswere working together very well. The results of this experiment were obvious to the community.Fewer and fewer of their children were dying because a lot of them received life-saving care at theright time. More and more pregnant women survived during child birth because trained healthpersonnel were available to assist them have a safe delivery. Women said they had access to familyplanning counselling and services which were now close to them.From Research to PolicyThe Ministry of Health and the Ghana Health Service were happy with these results. Resultsof the project were replicated as Community-based Health Planning and Services (CHPS)initiatives in Nkwanta, Birim North and Abura-Asebu-Kwamankese districts. These districtsalso found that the strategy was very effective in meeting the basic health needs of the people.Thus the Ministry’s thinking that if the strategy worked in Navrongo it could work in other partsof the country came true.Based on these results, in 2000, the Ministry of Health introduced the CHPS initiative as anational strategy for increasing access to primary health care services in underserved locations.The overall goal of CHPS is to improve the health status of people living in Ghana, by facilitatingactions and empowerment at household and community levels. CHPS aims to provide healthservices to the large number of people who live in disadvantaged communities including thosethat are remote or poor. It is based on a strategy that has been tested by community membersand found to be effective and different from the traditional way of delivering health services. Thetraditional way of providing health services is for people to visit the hospital or any health facilitywhen they are sick. The emphasis was on treatment or curative care. In CHPS, the slogan is:“prevention is better than cure”.All districts in Ghana are now implementing CHPS. Under CHPS, health services arecommunity-based. This means a trained health worker goes to live in the community andinvolves the community members in planning and delivery of health services.Key Elements of CHPS The Community (as Social Capital) Households and individuals (as Target) Planning with community members as prime beneficiary of health services (communityparticipation) Service delivery with their involvement (client-focused, need based services)xv
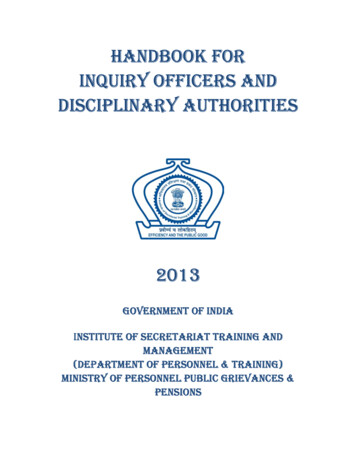
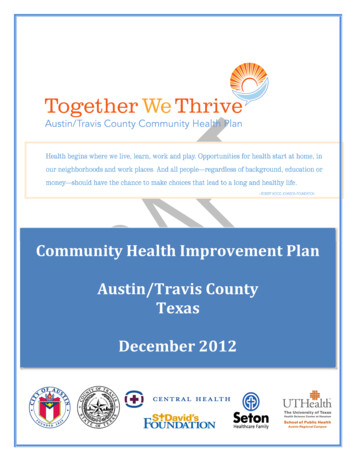
CHPS in Organisational structureThe Ghana Health Service organisational structure has a national headquarters that providesprogrammatic direction and support to the regions. The regions provide technical support to andcoordinate the work of the districts, which in turn support the sub-district. CHPS zones are partof the sub-district system.Ghana Health Service Organisational StructureNATIONAL LEVELREGIONAL LEVELDISTRICT LEVELSub-District LevelCHPSZONExviSub-District LevelCHPSZONECHPSZONESub-District LevelCHPSZONECHPSZONE
The Community-Based Health Planning and Services (CHPS) ConceptCHPS Implementation ProcessA key component of CHPS is a community-based service delivery that focuses on improvedpartnership with households, community leaders and social groups – addressing the demand sideof service provision and recognising the fact that households are the primary producers of health.A CHO engages each Community within the zone (catchment area) in micro planning of healthactivities, sometimes termed “community decision making systems.” The CHPS organizationalchange process relies upon community resources for construction, labour, service delivery, andprogramme oversight including monitoring and evaluation. As such, it is a national mobilizationof grass-root action and leadership in health service delivery.Based on these CHPS activity sequence, six general implementation activities that changeprimary health care services from a sub-district clinic based operation to a comprehensivecommunity-based programme are achieved. Each of the specific elements is referred to as a“CHPS milestone”:1. Planning: “CHPS zones,” are geographical areas where services are to be delivered, aremapped district-wide, dialogue with communities about their health needs is held, and asituation analysis of the existing health services within a district is conducted.2. Community Entry: Activities with chiefs and leaders residing within a CHPS zone areconducted in order to introduce and gain acceptance for the process, a durbar to introduceCHPS to the entire community is held, and a Community Health Committee, responsiblefor community-level and volunteer components of the CHPS process, is selected andtrained.3. Community Health Compound (CHC): This is the site where the CHO will live andprovide services. This phase includes securing funds for building or renovating a structureto serve as the CHC, selecting a site for the CHC that is acceptable and easily accessible tothe entire community, and mobilizing communal labour for CHC construction.4. Community Health Officer (CHO): This is the title given to a certified community healthnurse who has received additional training in order to provide the full complement of CHPSservices. This phase includes the training and deployment of the nurse to the CHPS zoneand holding a durbar to introduce the CHO to the CHPS zone residents.5. Essential Equipment: In this phase, equipment essential for conducting CHPS servicesis procured. This includes a motorbike for CHO community and home visitation andpurchasing bicycles for health volunteers as well as essential service delivery equipmentsuch as weighing scales, BP apparatus, thermometer.6. Volunteers: These are community residents who will aid the CHO by conducting healthpromotion activities and providing basic services. This phase consists of selecting andtraining the community health volunteers, convening a durbar to introduce them, holdingxvii
training for the Community Health Committee to oversee the work of volunteers and theprocurement and distribution of their supplies, and training the CHO on how to work withhealth committees and volunteers. The training sessions for each group of worker usuallycombine all the components described above.Completion of these six CHPS milestones heralds in a functional CHPS, ready to providecomprehensive primary health care services with strong health system strengthening at thecommunity level.Roles of CHO in the CHPS Zone1. Planning health services and programmes with community members2. Implementing health programmes with community participation3. Supervising community level health workers, including health care assistants, TBAs,volunteers, and health committee members4. Preparing and submitting monthly CHPS activity reports to sub-districtIconsThe following icons have been included in the CHO Training Manual to highlight main headingsin the book. These also add some aesthetic value to the manual. Below are the icons and how theyhave been used in the manual.Case study iconFacilitator/Participants’ InteractionIt is our expectation that you find this manual very useful.xviii
The Community-Based Health Planning and Services (CHPS) ConceptModule 1Managing CommunityHealth Officer Activities1
Module 1 Managing Community Health Officer ActivitiePurpose and OrganisationA Community Health Officer (CHO) needs special skills, personal qualities and attributes formanaging health activities in the community. This module is designed to introduce him/her toways of planning health activities, implementing the planned activities and assessing whethertargets set have been achieved. This includes ordering and storing equipment and supplies.Facilitation ApproachThe facilitation approaches to be used to impart this knowledge and the accompanying skillsfocus on discussing participants’ experiences, group work, role-plays, (real or simulatedsituations) case studies and field visits.ObjectivesReview these objectives now and all subsequent unit objectives as you begin each unit by: Reading each objectives yourself and Having a participant read the objectives aloud to the groupBy the end of this module, the CHO will be able to:1. Prepare a calendar for CHO activities2. Mobilise resources to carry out planned CHO activities3. Implement planned monthly activities4. Monitor and evaluate planned CHO activitiesContentsUnit 1: Preparing a Monthly Calendar for CHO Activities.Unit 2: Mobilising Resources for Monthly CHO Activities.Unit 3: Implementing Planned CHO Activities.Unit 4: Monitoring and Evaluating Planned CHO Activities.2
The Community-Based Health Planning and Services (CHPS) ConceptExpected OutcomeKnowledge Mobilising resources for monthly activities Stor
COMMUNITY HEALTH OFFICER Training Manual Community-Based Health Planning and Services (CHPS) Your Health Our Concern USAID G H A N A AT H E A L T S E R V I C E G H S . from application of the information in this book and make no warranty expressed or