Transcription
8/13/2018Neonatal Resuscitation:What you need to know!Cristina Zeretzke-Bien, MD FAAP, FACEPDepartment of Emergency MedicineDivision of Pediatric Emergency MedicineUniversity of FloridaObjectives: Recognize which neonates requireresuscitation Understand the steps to resuscitation (NRPguidelines) Understand the subsequent management ofa baby that has required resuscitationclinical case1
8/13/2018Physiology Difficulties Transitioning– Risk factors Maternal conditions (advanced age, diabetes,hypertension, substance abuse) Fetal conditions (prematurity, postmaturity, multiplegestation, anomalies) Antepartum problems (oligohydramnios,polyhydramnios, placental anomalies) Delivery (breech, transverse, meconium, maternalnarcotics, difficult delivery)Physiology Difficulties Transitioning– Lack of respiratory effort– Blockage of the airways– Impaired lung function– Persistent pulmonary hypertension– Cardiac anomalies2
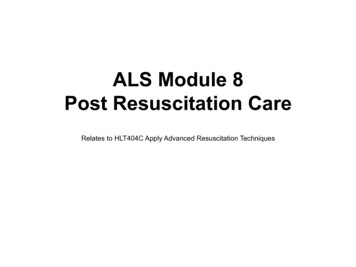
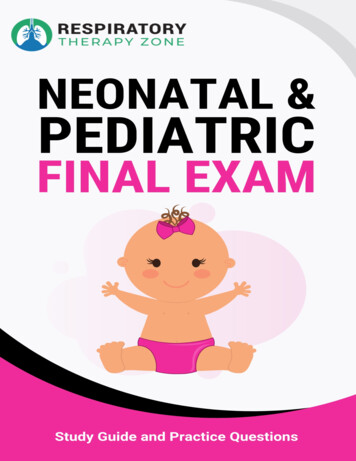
8/13/2018Inverted Pyramid of NewbornResuscitationInverted triangle and frequency (bar on right) of interventions performed in the delivery room.Modified from: Vento M,. Saugstad OD. Resuscitation of the term and preterm infant. Semin FetalNeonatal Med 2010;15(4): 216–2223
8/13/2018Who Requires Resuscitation?Answer 3 questions:1) Term gestation?2) Breathing or Crying?3) Good tone?Who Requires Resuscitation?4
8/13/2018Newborn Resuscitation General Overview of Resuscitation Steps Warm, suction, dry and stimulate Further intervention Breathing Circulation DrugsNewborn ResuscitationThe most recent changes to NRP:A. No longer routinely perform tracheal suctioningfor non-vigorous infants with meconiumstainingB. Use of cardiorespiratory monitor is thepreferred method for assessing the heart ratein newborn infantsC. Recommend to intubate prior to chestcompressionsD. There were changes to NRP?5
8/13/2018Newborn ResuscitationMeconiumNon-vigorous newbornswith meconium stainedfluid DO NOT requireroutine intubation andtracheal suctioningNewborn ResuscitationApproximately what percentage of terminfants have meconium stainedamniotic fluid?A: 5%B: 12%C: 27%D: 53%E: All of them .They ALL haveMeconium!“Meconium stained amniotic fluid is a perinatal risk factorthat requires the presence of one resuscitation teammember with full resuscitation skills, including endotrachealintubation”-NRP Instructor Update6
8/13/2018Newborn ResuscitationtMeconium– In 2000, routine suctioning for vigorous infants withmeconium stained fluid was no longer recommended– 2012 study found for each 30 second delay of bagvalve mask ventilation increased mortality andmorbidity by 16%– 2015 First randomized study comparing suctioning vsno suctioning in non-vigorous infants found nodifference in meconium aspiration syndrome,asphyxia, mortality or PPHNNewborn ResuscitationMeconium Take Home Message Little or no evidence suggesting a benefit tosuctioning and at least some evidence ofpotential harm Routine suctioning is no longer recommended If the infant requires respiratory support thisshould begin as soon after birth as feasiblypossible7
8/13/2018PPV Use correct mask sizeUse bags with volumes between 200-750 mlDo not overinflate lungsAdminister breaths at 40-60 per minuteAssess heart rate and oxygen saturation afterPPV is started– Effective resuscitation should be evident byrising HRNewborn ResuscitationCASE 1Introduction – Multiparous female to ED with severecontractions; is preterm (28 weeks); precipitous deliveryof pre-term neonate as put into resuscitation bay.PMH for mother –G6P6, Normal prenatal visits, estimategestational age 28 weeks currently, no other issues.Exam for mother – Awake, alert, stable, can provideappropriate history as needed8
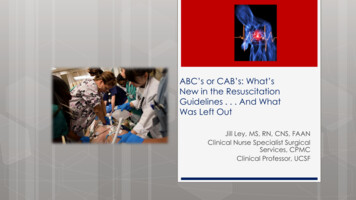
8/13/2018Newborn ResuscitationCASE 1Initial Description of Neonate –Placed in warmer; is not breathingor crying; poor muscle tone;cyanotic; note clear amniotic fluid.Exam –Cyanotic neonate, unresponsive,floppyNo respiratory effort/apneicHeart rate 50’s ( 60)APGAR 1Copyright: Author: Jules Atkins, RM, Supplied by:Brandi Catt, 2006-01-279
8/13/2018Newborn Resuscitation What is the next step?– “ABCDs” Initial steps – provide warmth, suction Airway asnecessary, dry, stimulate Reassess Ventilation corrective steps (Breathing) Reassess Chest compressions Reassess Give DrugsNewborn Resuscitation Initial steps– Provide warmth Warm towels Radiant warmer– Clear airway asnecessary– Dry andstimulate– ReassessTerm Gestation?Breathing or crying?Good tone?YesRoutineCareNoWarmPosition airwayClear airway if neededDryStimulate60 secHR less than 100?Gasping orApnea?10
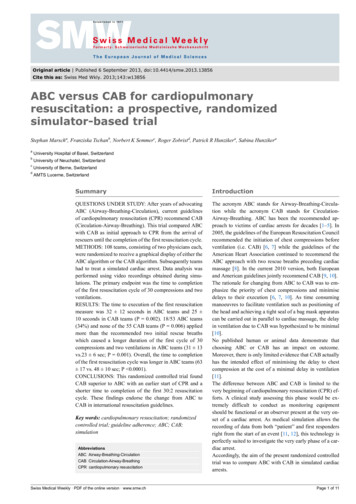
8/13/2018Newborn ResuscitationCASE 1ReassessmentPatient remains:CyanoticApneicPulse is in the 50sCopyright: Author: Jules Atkins, RM, Supplied by:Brandi Catt, 2006-01-27Newborn Resuscitation Subsequent steps– Positive-pressureventilation (PPV) Self-inflating bag Position neck inneutral position Ventilate at 40-60bpm ECG (3-lead)monitoring– SpO2 monitoring Right hand or wristHR less than 100?Gasping orApnea?NoYesPositive-PressureVentilationSpO2 monitoringLaboredBreathingCyanosisYesClear airwaySpO2 monitorCPAP?30 secHR below 100?– Reassess11
8/13/2018Newborn ResuscitationCASE 1ReassessmentSomewhat improved heart rateand colorHeart rate increases to 90’swith continued PPVOxygen saturation in the 80’sCopyright: Author: Jules Atkins, RM, Supplied by:Brandi Catt, 2006-01-27Newborn ResuscitationQuick Tangential Point Pulse oximetry– Attached to preductal location on right upper extremity– Saturation may normally remain low for several minutes afterdeliveryTargeted preductal SpO2 afterdelivery1 min2 min3 min4 min5 min10 min60-65 percent65-70 percent70-75 percent75-80 percent80-85 percent85-95 percent12
8/13/2018Newborn Resuscitation Subsequent steps– Heart rate between60-100 BPM Ventilationcorrective steps Continue BMVventilation (30 sec)NoPostresus.careHR below 100?YesVentilation correctivestepsHR 100 but 60?Yes ContinueventilationNoHR 60?Newborn ResuscitationQuick Tangential Point Ventilation Corrective Steps – 3 possible reasons for ineffectiveventilation– Inadequate mask seal– Airway is blocked– Not enough pressure usedMeasures to improve positive-pressure ventilationMMask adjustmentRReposition airwaySSuction mouth and noseOOpen mouthPPressure increaseAAirway alternative13
8/13/2018Newborn ResuscitationCASE 1ReassessmentHeart rate increases to 100with continued PPVAttempts to providesupplemental oxygen result indecreasing oxygen saturationand decreasing heart rateObvious inadequaterespiratory effortCopyright: Author: Jules Atkins, RM, Supplied by:Brandi Catt, 2006-01-27Newborn ResuscitationNoHR below 100?Postresus.careYesYour kind of stuckhere aren’t you Ventilation correctivestepsHR 100 but 60?Yes ContinueventilationNoHR 60?14
8/13/2018Newborn ResuscitationWhat to do if positive-pressure ventilation is to becontinued Consider placing anorogastric tube to Consider endotrachealintubation for – Suction gastric contents– Serve as vent for air instomach– Bag-mask ventilation is ineffective or prolonged– Chest compressions– Special circumstancesNewborn ResuscitationCASE 1ReassessmentHeart rate with PPV remainsabove 100Color improvedContinue to provide respiratorysupport (oxygen saturation inlow 90’s)NICU team present withwarmerCopyright: Author: Jules Atkins, RM, Supplied by: BrandiCatt, 2006-01-2715
8/13/2018Endotracheal Tube Selection forNewborn ResuscitationTube SizeGestational Age(Weeks)Weight (Grams)2.5 28 1,000328 – 341,000 – 2,0003.534 – 382,000 – 3,0003.5 - 4 38 3,000Newborn ResuscitationQuick Tangential Point Vascular access– Umbilical vein catheter Aseptic technique Depth of 2-4 cm16
8/13/2018Newborn ResuscitationQuick Tangential Point Drugs– Epinephrine Action – increases heart rate and myocardialcontractility, causes peripheral vasoconstriction Indication – heart rate 60 despite adequateventilation and chest compressions Dose – 0.01 mg/kg of 1:10,000 solution IVNewborn Resuscitation Summery of resuscitation steps– Initially provide warmth, clear airway, dry and stimulate infant– If meconium staining and non-vigorous infant, suction beforestimulation– If infant continues with poor respiratory effort or HR 100, startPPV with BMV, initiate pulse oximetry– Intubate if BMV is ineffective or prolonged, or chestcompressions are being performed– If HR 60 despite adequate ventilation, start chestcompressions at 90 per minute– If HR rate 60 despite adequate ventilation and chestcompressions, administer IV epinephrine17
8/13/2018The End!18
Department of Emergency Medicine Division of Pediatric Emergency Medicine University of Florida Recognize which neonates require resuscitation Understand the steps to resuscitation (NRP guidelines) Understand the subsequent management of a baby