Transcription
Obstetric Anaesthesia Guidelines 7:Obstetric Anaesthesia EmergenciesIncluding Maternal Collapse and ResuscitationVersion4Version DateDec 2019Author(s)PagesRama Varadan, Suzanne Taylor, Mathew Tinker28Implementation dateReview DateDocument ReferenceDec 2022
Contents1Management of Unexpected Difficult / Failed Intubation in Obstetrics52Management of a “Total Spinal93Local Anaesthetic Toxicity Guideline AAGBI104Malignant Hyperthermia115Cardiopulmonary Resuscitation in Pregnancy125.1Best Practice Points . 125.2Background . 125.3Possible causes of cardiac arrest at term . 125.4Resuscitation in Pregnancy. 125.4.1Physiological changes of pregnancy . 135.4.2Veno-caval Occlusion . 135.4.3Cardiac Output . 135.4.4Oxygen Consumption and FRC . 165.4.5Intubation . 165.4.6Gastric Contents . 165.5Perimortem Caesarean Section . 176Maternal Collapse187Amniotic Fluid Embolism (AFE)2087.1Introduction . 207.2Definition. 207.3Objectives . 217.4Practice recommendations . 217.5Risk factors . 217.6Presentation. 217.7Management . 217.8Key messages . 22Management of women with suspected Neurological disorders- Seizures 228.1.1Definition. 222
8.1.2Objectives . 228.1.3Risk factors/Red flag signs. 228.1.4Differential diagnosis . 238.1.5Management . 238.1.6Learning points . 239Anaphylaxis2310Cardiac Diseases2611Drug Overdoses26V3 Updates Nov18 – Incorporates MBRRACE guidance / GAP analysisSection 2.1- added advice on early cardiac compressions in sudden onset severe shocksection 2.4.2- advice on aortocaval compressionsection 2.4.5 – Incorporates advice on sizes on ET Tubes on resus trollies/cartsV4 Updates Dec19- more comprehensiveSection 2 Management of total spinalSection 3 LASTSection 4 MHSection 5.4.5Intubation sectionSection 6 Maternal collapseSection 8 Management of women with suspected neurological disordersSection 9 AnaphylaxisSection 10 Cardiac diseaseSection 11 Drug overdoses3
Obstetric anaesthetic emergenciesFailed intubationTotal SpinalLocal anaesthetic toxicityMalignant hyperpyrexiaCauses of maternal collapseHaemorrhage- APH, PPHSepsisAmniotic fluid embolismSeizures: eclampsia, intracranial catastrophe, hypoglycaemiaAnaphylaxisCardiac Disease- Peripartum cardiomyopathy/ aortic dissectionDrug Overdose- Magnesium toxicity, Local anaesthetic toxicityCauses of maternal cardiac arrestHypoxiaHaemorrhageThromboembolic event: Pulmonary embolism, myocardial infarction, amniotic fluid embolismToxinsHypo, hyperthermiaHypo, hyperkalaemiaTamponadeTension pneumothorax4
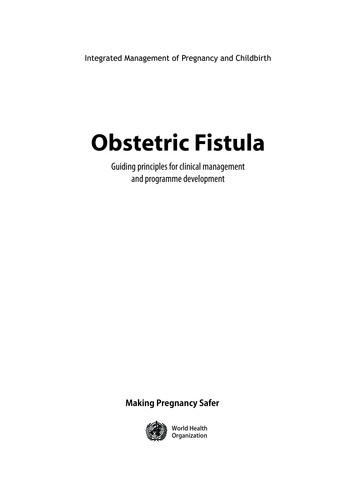
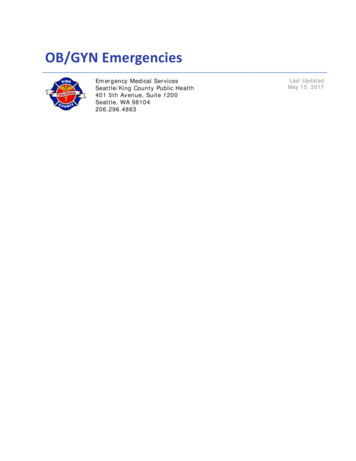
1 .Management of Unexpected Difficult / Failed Intubation in Obstetricshttps://das.uk.com/guidelines/obstetric airway guidelines 20155
6
7
8
2Management of a “Total SpinalA “total spinal” block is extremely rare but can occur with frightening rapidity and result in death of the motherand unborn baby if not quickly recognised and treated. Usually it happens when topping up an epidural forsurgical intervention with high doses of local anaesthetics, which are inadvertently injected intrathecally. Call for help straight away; you may need several pairs of hands. Reassure the mother and start ABC resuscitation: i.e. respiratory and cardiac support. Give 100% oxygen with bag and face mask and assist ventilation. Establish wide-bore intravenous access and infuse fluids rapidly. Treat hypotension with fluids, vasopressors, left lateral tilt and elevate legs. Monitor blood pressure and oxygen saturation and CTG continuously. You may need to intubate and ventilate (with small doses of midazolam/ induction agent) if breathing isdifficult or the patient starts to lose consciousness. Watch for warning signs: hypotension, bradycardia, husky voice and weak hands. The combination ofbradycardia, hypotension and hypoxia may lead to cardiac arrest. Hence bradycardia should be treatedpromptly with atropine. Ventilation needs to be continued until spinal block recedes and the patient is able to breath unaided. Consider urgent delivery of fetus if severe fetal bradycardia develops during resuscitation of mother. Admit to high dependency or intensive care unit post-operatively for close observation of vital functionsand support if needed.9
3 Local Anaesthetic Toxicity Guideline AAGBI10
4 Malignant Hyperthermia11
5 Cardiopulmonary Resuscitation in Pregnancy5.1Best Practice Points All staff involved in intrapartum care should be familiar with basic life support guidelines for the pregnantpatient and should follow them during resuscitation attempts. 30 degree left lateral tilt should be used to minimise aortocaval compression and maximise cardiac output. In sudden onset severe maternal shock e.g. anaphylaxis, the presence of a pulse may be an unreliableindicator of adequate cardiac output. In the absence of a recordable blood pressure or other indicator ofcardiac output, the early initiation of external cardiac compressions may be life-saving. Caesarean section should be performed after 4 minutes of unsuccessful resuscitation. Senior obstetric, anaesthetic and neonatal staff should be involved as early as possible. Record keeping should be meticulous ensuring that treatment given and timings are clearly identified.5.2BackgroundCardiac arrest in pregnancy is thought to occur in approximately 1:30,000 maternities1. Maternal and fetalsurvival rates are low following cardiac arrest.( Exact figures are not known but it has been suggested thatmaternal survival is approximately 40% 6). This is partly due to the generally catastrophic events leading tocardiac arrest, but also the physiological changes of pregnancy can hamper resuscitative efforts.Possible causes of cardiac arrest at termObstetric Causes5.3 Massive Haemorrhage Amniotic Fluid Embolism Eclampsia/HELLP syndrome Magnesium Sulphate ToxicityNon - Obstetric Causes Pulmonary embolism Septic shock Cardiovascular disease Myocardial infarction Peripartum cardiomyopathy Trauma Anaesthetic complications5.4Resuscitation in PregnancyIn the event of maternal cardiorespiratory arrest, resuscitation should begin immediately and should followcurrent basic and advanced life support guidelines (see below). Physiological changes of pregnancy and thepresence of the fetus demand some additions to the normal algorithms: 30o left lateral tilt of the mother Early tracheal intubation Perimortem Caesarean sectionThese are explained below:12
5.4.1 Physiological changes of pregnancyThe following is a list of the major physiological and anatomical changes that make resuscitation in pregnancydifficult and the steps that can be taken to minimise their effects.5.4.2 Veno-caval OcclusionAortocaval compression significantly reduces cardiac output from 20 weeks of gestation onwards andthe efficacy of chest compressions during resuscitation. [C]From around 20 weeks of gestation onwards the gravid uterus reduces venous return in the supine position. Atterm, the vena cava is completely occluded in 90% of supine pregnant women. Compression of the aorta andinferior vena cava in the supine position by the uterus decreases cardiac output to 25-30%.Aortocaval compression should be suspected in any supine pregnant woman who develops severehypotension after induction of anaesthesia, even if some lateral tilt has been applied. If there is a delay indelivery, putting the woman into the left lateral position may be the only option if other manoeuvres fail or if thewoman has refractory severe hypotension.During resuscitation, tilt the mother approximately 15- 30o to the left in order to reduce aortocaval compression.This can be achieved by using a rescuer’s knees as a ‘human wedge’, pillows or a purpose made wedge underthe patient’s right side, and by then moving the uterus to the left by manual displacement.5.4.3 Cardiac OutputMaternal cardiac output increases by 40-50% in late pregnancy to satisfy a 20% increase in resting oxygendemands of the fetoplacental unit. In late pregnancy the uterus receives approximately one tenth (some reportssuggest 30%) of the cardiac output.When cardiopulmonary arrest occurs, chest compressions are needed to produce a cardiac output. In thenonpregnant situation, they achieve around 30% of the normal cardiac output 2-4. Aortocaval compressionfurther reduces cardiac output to approximately 10% of the nonpregnant cardiac output.5 When a pregnantpatient is tilted the efficiency of compressions is reduced further but the detrimental effect of aortocavalcompression is greater than that of left tilt.13
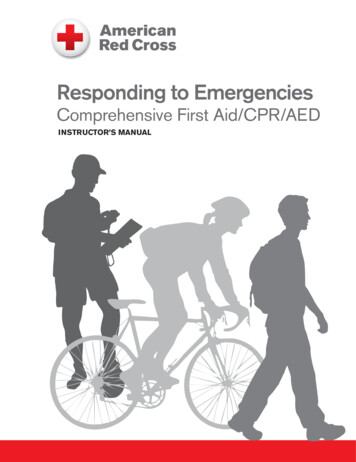
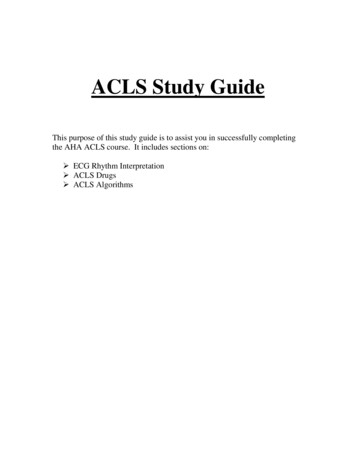
Adult Basic Life Support Algorithms (Resus Council UK 2015 Guidelines)BLS14
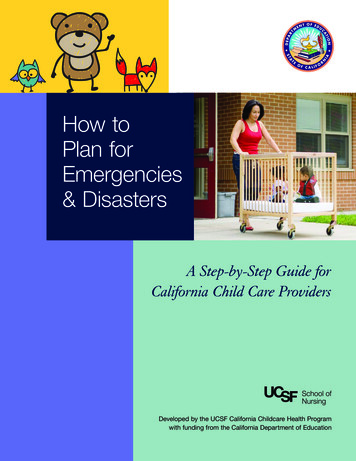
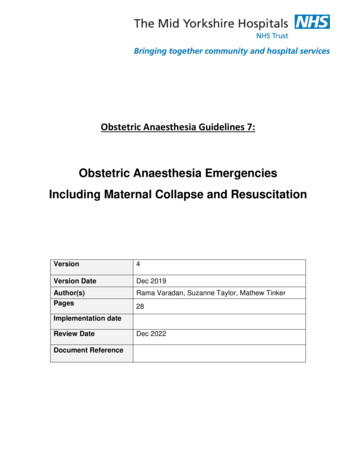
Left Lateral Tilt /Manual displacementof UterusALSAdult Advanced Life Support Algorithms (Resus Council UK 2015 Guidelines)15
5.4.4Oxygen Consumption and FRCChanges in lung function, diaphragmatic splinting and increased oxygen consumption make pregnantwomen become hypoxic more readily and make ventilation more difficult. [C]Oxygen storage is reduced due to a 20% decrease in functional residual capacity of the lungs. Maternalcardiac output increases by 40-50% in late pregnancy to satisfy a 20% increase in resting oxygen demands ofthe fetoplacental unit.These changes make it difficult to provide enough oxygen delivery using CPR toresuscitate a near term pregnant mother.Hypoxia occurs very rapidly. For this reason, early tracheal intubation is ideal although attemptsat intubation should not override oxygen delivery. Irreversible brain damage will occur4-6 minutes following cerebral hypoxia.5.4.5IntubationSupplemental high flow oxygen should be administered as soon as possible to counteract rapiddeoxygenation. [GPP]Bag and mask ventilation should be undertaken until intubation can be achieved. [GPP]Difficult intubation is more likely in pregnancy. [C]Weight gain in pregnancy, large breasts inhibiting the working space and laryngeal oedema can all contributeto making intubation more difficult.6-75.4.6 Gastric ContentsPregnant women are at an increased risk of aspiration. [C]Pregnant women are at a significantly higher risk of regurgitation and aspiration, secondary to theprogesterone effect relaxing the lower oesophageal sphincter and delayed gastric emptying, along with theraised intra-abdominal pressure secondary to the gravid uterus. Aspiration pneumonitis in pregnant women,known as Mendelson’s syndrome,8 can be severe, particularly as the gastric pH is lower than in thenonpregnant population. The risks can be minimised by early intubation with effective cricoid pressure, and theuse of H2 antagonists and antacids prophylactically in all women considered to be at high risk of obstetricintervention during labour. [Evidence Level 2 ]Early Intubation will protect the airway from aspiration of gastric contents but see caveat above.It is recommended that all resuscitation carts used in maternity units should include endotracheal tubes nolarger than 7.0mm and include smaller sizes such as 6.0mm and 5.0mm.16
5.5Perimortem Caesarean SectionThe concept of perimortem Caesarean section was introduced in 19869. The theory is that resuscitation islikely to be ineffective in the third trimester because of aortocaval compression and that timely delivery willoptimize outcome for mother and baby. As CPR produces (at maximum) 30% of normal cardiac output and theuterus takes 30% of cardiac output at term, CPR is unlikely to sustain maternal and foetal life. A recent review9has supported this hypothesis. Perimortem Caesarean section should be initiated within 4 minutes of cardiacarrest if resuscitation is unsuccessful, in order that cardiac output may be re-established within 5 minutes. Thiswill minimise the danger of hypoxic neurological damage to the mother. This means that decision forperimortem section should be made at 2-3 minutes, if no return of spontaneous circulation has been achievedwithin this time from initiating CPR. A pair of gloves, scalpel and some swabs will suffice initially and transfer totheatre is not necessary until after the baby is delivered. The neonatal resuscitation team should be present atdelivery. It is prudent to trigger the massive haemorrhage protocol in an undelivered woman at the time thedecision to proceed to peri-mortem caesarean section is made, and within the same time frame for a deliveredwoman in whom there is also no return of spontaneous circulation at four minutes after advanced life supportcommences.Further Care The neonatal team will take charge of the baby. The mother should be transferred to ITU/HDU.Early involvement of ITU specialists is essential. Relatives should be kept fully informed of events by seniorstaff. Records should be reviewed to make sure they are complete and any further retrospective informationshould be added once the patient is stable.Unsuccessful Resuscitation In the event of unsuccessful resuscitation the bereavement team should also beinvolved. The head of midwifery and the clinical director should be informed. Refer to “maternal death”guidelines for further information.Staff Debrief All staff involved in a maternal cardiac arrest should be involved in a formal debrief. This shouldbe organised by senior midwifery and medical staff.17
6 Maternal CollapseMaternal collapse is defined as an acute event involving the cardiorespiratory systems and/or central nervoussystems, resulting in a reduced or absent conscious level (and potentially death), at any stage in pregnancyand up to 6 weeks after delivery. Maternal collapse can result from a number of causes. A systematicapproach should be taken to identify the cause. [B]This section aims to cover situations which may be classed as an emergency that may involve anaestheticinput, as the condition may lead to the patient becoming critically ill or suffering a cardiac arrest.Causes of maternal collapse18
Common causes of maternal collapse HaemorrhageSepsisAmniotic fluid embolismSeizures: eclampsia, intracranial catastrophe, hypoglycaemiaAnaphylaxisCardiac Disease – Ischemic heart disease, arrthymia’s, peripartum cardiomyopathy/ aorticdissectionDrug overdose and toxicity - Magnesium sulphate and local anaesthetics1. HaemorrhageThis is among the most common causes of maternal collapse and was responsible for 13 maternal deathsbetween 2012 and 2014.10 Major obstetric haemorrhage has an estimated incidence of 6 in 1000 maternities. 11Causes of major obstetric haemorrhage include postpartum haemorrhage, major antepartum haemorrhagefrom placenta praevia, placental abruption, uterine rupture and ectopic pregnancy. In most cases of massivehaemorrhage leading to collapse, the cause is obvious, but concealed haemorrhage should not be forgotten,including following caesarean section and ruptured ectopic pregnancy. Other rarer causes of concealedhaemorrhage include splenic artery rupture12 and hepatic rupture. Blood loss is often underestimated,13-14especially slow, steady bleeding, and fit, healthy women can tolerate significant loss prior to showing signs ofdecompensationManagement refer to obstetric haemorrhage including placenta praevia/ Accreta guideline MYH-GUIDE-362. SepsisSepsis has been recognised for centuries as a significant cause of maternal morbidity and mortality, andsubstandard care continues to feature in the cases that result in death.10 Bacteraemia, which can be present inthe absence of pyrexia or a raised white cell count, can progress rapidly to severe sepsis and septic shockleading to collapse.15 The most common organisms implicated in obstetric sepsis are the streptococcal groupsA, B and D, pneumococcus and Escherichia coli. [Evidence level 2–]Septic shock should be managed in accordance with the MYH-GUIDE-48 and Surviving Sepsis Campaign guidelines.The Surviving Sepsis Campaign has updated the management of sepsis and septic shock. 16 The speed andappropriateness of therapy administered in the initial hours after severe sepsis develops are likely to influenceoutcome with early resuscitation improving survival rates. A multidisciplinary team approach is required,including midwives, consultant obstetricians, anaesthetists, haematologists, intensivists and microbiologists.The following ‘Care Bundle’ should be applied immediately or within 6 hours, and has been shown tosignificantly improve survival rates:17,181. Measure serum lactate.2. Obtain blood cultures and culture swabs prior to antibiotic administration.19
3. Administer broad spectrum antibiotic(s) within the first hour of recognition of severe sepsis and septic shockaccording to local protocol.4. In the event of hypotension and/or lactate more than 4 mmol/l:a) Give an initial minimum of 30 ml/kg of crystalloidb) Once adequate volume replacement has been achieved , a vasopressor (norepinephrine, with vasopressin orepinephrine in addition, if required) and/or an inotrope (for example, dobutamine) may be used to maintain meanarterial pressure more than 65 mmHg.Further management consists of:5. In the event of hypotension despite fluid resuscitation (septic shock) and/or lactate more than 4 mmol/l:a) dynamic variables of fluid status are preferred to static variables and the use of central venous pressure alone toguide fluid resuscitation can no longer be justifiedb) consider steroids if unresponsive to adequate fluid resuscitation and vasopressor therapy.6. Maintain oxygen saturation at more than 94% (88%–92% in women at risk of hypercapnic respiratory failure) withfacial oxygen.18 Consider transfusion if haemoglobin less than 70 g/l.Ongoing management involves continued supportive therapy, removing the septic focus, administration ofblood products if required, and thromboprophylaxis.17 [Evidence Level 1 ]7 Amniotic Fluid Embolism (AFE)7.1IntroductionAFE is one of the leading causes of maternal mortality according to the recently released UKOSS (UKObstetric Surveillance System) seventh annual report 2013.7.2DefinitionAmniotic Fluid Embolism is the entry of amniotic fluid into the maternal circulation. AFE is defined clinicallyaccording to the criteria below:In the absence of any other clear cause, acute maternal collapse with one or moreof the following features:EitherCardiac arrhythmias or arrestCoagulopathyConvulsionHypotensionMaternal haemorrhageAcute fetal compromiseShortness of breathPremonitory symptoms, e.g. restlessness, numbness, agitation, tinglingOrWomen in whom the diagnosis was made at post-mortem examination by finding fetal squamous cells or hairin the lungs20
7.3ObjectivesThis guideline aims to: Ensure clear, evidence-based and referenced guidance is in place to inform the clinical practice of allmembers of the multidisciplinary obstetric team in relation to the risks and management of amniotic fluidembolism. To ensure safe and consistent care is provided at the MYHT. To promote effective and seamless teamwork in an emergency situation.This guideline should be used in conjunction with Obstetric Haemorrhage and obstetric collapse guidelines.7.4Practice recommendationsAlthough, the incidence of AFE quoted is 2/100,000 pregnancies 19estimates of incidence vary considerably(1.3-12.5 / 100,000 pregnancies) 19. Maternal mortality attributed to AFE varies from 16-86%. UKOSS has dataon 119 confirmed cases of AFE from 2005 till 2013. In the recent MMBRACE report 20there were 8 confirmedcases of maternal mortality attributed to AFE.7.5Risk factors Induction of labour Caesarean section Multiple pregnancy Older ethnic minority women7.6PresentationAFE presents at or before delivery in 53% of cases, the remainder occurring within six hours of delivery,usually in the first 30 minutes. The most common features at first presentation are21 Premonitory symptoms (62%) Acute fetal compromise (46%) Seizures (38%) Shortness of breath (33%) Hypotension (28%) Cardiac arrest (20%)7.7ManagementThe treatment of AFE is supportive22Remember ABC Adequate oxygenation and ventilation Maintenance of cardiac output Aggressive correction of coagulopathy.The incidence of uterine atony is increased in AFE and may contribute to a postpartum haemorrhage. TheMajor Obstetric Haemorrhage protocol (MOH) should be instituted at time of decision for perimortemCaesarean section, and within same time frame for delivered woman with no response to CPR at 4 minutes.Transfusion should be with red cells as soon as possible to avoid haemodilution, and in a ratio of 1:1:1 redcells:FFP:platelets in the first instance. Keep checking fibrinogen and platelet levels and arterial blood gases21
and lactate at frequent intervals. See Obstetric Haemorrhage and obstetric collapse guidelines for moredetails.7.8Key messagesInduction of labour is a high risk factor for AFE.Remember Airway, Breathing, Circulation.Perimortem caesarean section should be carried out within five minutes or as soon as possible after cardiacarrest and is carried out for the benefit of the woman; there is no need to confirm fetal viability.Massive obstetric haemorrhage protocol should be initiated in an undelivered woman at the time the decisionto proceed to peri-mortem caesarean section. Hysterectomy should not be delayed in case of intractablebleeding from atonic uterus. It is important to replace major blood loss with red cells, plasma and platelets assoon as possible.8 Management of women with suspected Neurological disorders- SeizuresNeurological disorders were the 5th leading cause of maternal death and the 3rd leading cause of directmaternal death in the 2013-15 MBRRACE-UK report, published in 2017. Stroke accounted for 12 deathsbetween 2013-15, with 7 from subarachnoid haemorrhage and 5 from intracranial haemorrhage. A further 16women died from stroke between 6 weeks and 1 year post-natal.These numbers do not include intracranial haemorrhage from pre-eclampsia. There were no deaths reportedfrom thrombotic stroke.8.1.1 DefinitionNeurological disorders can encompass a whole range of conditions from severe epilepsy to stroke. We areconcerned with those causing maternal collapse, which is mainly haemorrhage, neurological infection(meningitis) and other causes of acute raised intracranial pressure. For the purposes of this document we willbe focussing on stroke secondary to haemorrhage.Pregnancy should not alter the investigation and treatment of a woman presenting with a stroke (MBRRACE2017)8.1.2 ObjectivesThis guideline aims to:1. Ensure clear, evidenced-based guidance is in place to inform the clinical practice to all members of theMDT in relation to the risks and management of neurological causes of maternal collapse.2. To ensure safe and consistent care is provided.3. To highlight a high index of suspicion in patients presenting with atypical headache.4. To promote effective and seamless teamwork in an emergency situation.Although the incidence of maternal death due to stroke is rare, 0.48 per 100000 maternities, its managementand prognosis is reliant on early recognition, CT scan and referral/transfer to a neurosurgical centre.8.1.3Risk factors/Red flag signs22
Headache in pregnancy is common. Patients presenting with new onset headache or headache with atypicalfeatures need a full neurological examination, including fundoscopy to establish a concern and excludeintracranial pathology (MBRRACE 2017).Atypical features:1.2.3.4.8.1.41.2.3.4.5.6.7.8.VomitingNeck stiffnessVisual disturbanceFocal neurologyDifferential diagnosisSimple/tension headacheMigraine – can get focal neurology. May be past medical racranial haemorrhageInfectionCortical vein thrombosisSpace-occupying lesion8.1.5 ManagementThis relies on an index of suspicion, full history and examination, including fundoscopy, and CT scan or referralto neurologist/medics. In the case of maternal collapse1. ABC2. Early anaesthetic/critical care involvement3. Adequate oxygenation and ventilation (keep pO2 10-15kPa and pCO2 3.5-4.5), may need to beintubated to maintain normal ventilation variables.4. Maintain good cardiac output.5. Appropriately sedated (to reduce CMR)8.1.6 Learning points1. High index of suspicion with full neurological management, including fundoscopy is needed for promptdiagnosis.2. Diagnosis needs early CT scan.3. In maternal collapse follow ABC.4. Needs early anaesthetic help.9 AnaphylaxisAnaphylaxis is a severe, life-threatening generalised or systemic hypersensitivity reaction,23 resulting inrespiratory, cutaneous and circulatory changes, and possibly gastrointestinal disturbance and collapse.23
24
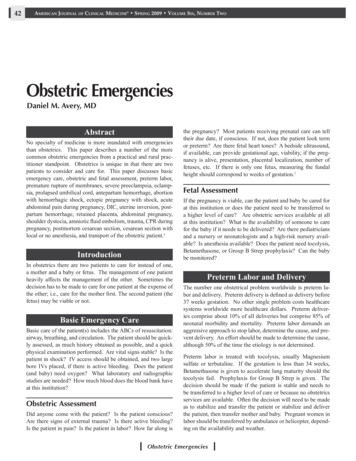
Resuscitation Council Anaphylaxis management algorithm25
10 Cardiac DiseaseCardiac disease was the most common overall cause of indirect maternal death in the latest MBRRACEreport,10 being responsible for 51 maternal deaths between 2012 and 2014. The majority of deaths 161secondary to cardiac causes occur in women with no previous history,10 ,24 and almost one in five deathsoccurred in an ambulance or accident and emergency department. The main cardiac causes of maternaldeath are ischaemia and sudden arrhythmic cardiac death with a structurally normal heart. 10Most cardiac events have preceding signs and symptoms. Aortic root dissection can present in otherwisehealthy women, and signs and symptoms,such as central chest or interscapular pain, a wide pulse pressure(mainly secondary to systolic hypertension) and a new cardiac murmur, must prompt appropriate imaging and,if required, referral to a cardiologist. The incidence of congenital and rheumatic heart disease in pregnancy areincreasing, secondary to increased survival rates with improved management of congenital heart disease andincreased immigration. In addition, women with mechanical prosthetic heart valves are at particularly increasedrisk of complications in pregnancy.24 These cases should be managed by an appropriately skilled andexperienced multidisciplinary team, usually in regional centres.10 Other cardiac causes include:cardiomyopathy; dissection of the coronary artery; acute left ventricular failure; infective endocarditis; andpulmonary oedema.After successful resuscitation, cardiac cases should be managed by an expert cardiology team. [GPP]After initial resuscitation, the ongoing management of cardiac disease is similar to that in the nonpregnantstate, although in many cases, delivery will be necessary to facilitate this. [Evidence Level 4]Although thrombolysis can be associated with significant bleeding from the placental site, it should be given towomen with acute coronary insufficiency, although caution should be exercised in the perioperative period.25 Ifavailable, percutaneous angioplasty allows accurate diagnosis and definitive therapy. [Evidence Level 4]11 Drug overdose and toxicityMany drug overdoses have specific therapy which is dependent on the drug in question and appropriate helpshould be sought in the management of such cases. In obstetric practice, the two main drugs that can give riseto overdose or toxic problems are magnesium sulphate and local anaesthetic agents.Magnesium sulphateThe antidote to magnesium toxicity is 10 ml 10% calcium gluconate given by slow intravenousinjection.Local anaesthetic agents- See section 3References1.Morris S, Stacey M. Resuscitation in pregnancy. BMJ 2003;327:1277-9.2. Sanders AB, Meislin HW, Ewy GA. The physiology of cardiopulmonary resuscitation. JAMA 1984;252:3283–6.3. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 3: AdultBasic Life Support. Circulation 2000;102 (Suppl 1);22–59.4. Donegan JH. Cardiopulmonary resuscitation. Springfield, IL: Charles C Thomas Ltd.; 19825. Kerr MG. The mechanical effects of the gravid uterus in late pregnancy. J Obstet Gynaecol Br Commonw1965;2; 513–296. Mushambi MC, Kinsella SM, Popat M, Swales H, Ramaswamy KK, Winton AL, et al.; ObstetricAnaesthetists' Association; Difficult Airway Society. Obstetric Anaesthetists' Association and Difficult Airway26
Society guidelines for the management of difficult and failed tracheal intubation in obstetrics. Anaesthesia2015;70:1286–306.7. Kinsella SM, Winton AL, Mushambi MC,
Reassure the mother and start ABC resuscitation: i.e. respiratory and cardiac support. Give 100% oxygen with bag and face mask and assist ventilation. Establish wide-bore intravenous access and infuse fluids rapidly. Treat h