Transcription
S aintl ouisu niversityg eriatrice valuationmnemonics ands creening Tools
This book is published bySaint Louis University School of MedicineDivision of Geriatric Medicineand theGeriatric Research, Education, and Clinical CenterSt. Louis VA Medical CenterThis project is supported by funds from the Division of State, Communityand Public Health (DSCPH), Bureau of Health Professions (BPHr), HealthResources and Services Administration (HRSA), Department of Health andHuman Services (DHHS) under grant number D31HP08827; Gateway GeriatricEducation Center for 1.2 million. This information or content and conclusionsare those of the authors and should not be construed as the official positionor policy of, nor should any endorsements be inferred by the DSCPH, BHPr,HRSA, DHHS, or the U.S. Government.Joseph H. Flaherty, M.D.Nina Tumosa, Ph.D.SLU Geriatric Evaluation Mnemonic Screening Tools1
table of contentsTitle PageIntroduction4AGING SUCCESSFULLY Passport to Aging5Aging Successfully Poster6-7ALCOHOLCAGE Questionnaire8ANTICOAGULATIONHEMORR2HAGES 9CHADS2 10CANCER SCREENING Caution11DEHYDRATION Simple Screen for Dehydration12DELIRIUM Acute Change in MS13CAM14COCOA-PHSS15Delirium16Be Aware/Prevent17Avoid Restraints18Dementia VAMC Slums Exam19Dementia20The Caring Guide21DEPRESSION GDS22Sig E Caps23Cornell Scale for Depression 24DIZZINESSBPPV25Dizziness26-27V2ertigo PM28ELDER ABUSE Neglect29EYES AND EARS Vision30Hearing31FALLSDual Tasking32-33Again I’ve Fallen34Timed Up & Go35Safe and Sound361-Leg Standing 375-Chair Stands382SLU Geriatric Evaluation Mnemonic Screening Tools
table of contentsTitlePage39FRAILTY Frail40Frailty41FUNCTION ADLsIndicators for Patient Therapy I 42Indicators for Patient Therapy II 43Indicators for PatientTherapy III 4344HOSPITALIZATIONDr. Iatros45Bed Rest is Bad46DC Plan47Foley Guidelines48HYPOGONADISM ADAM49INCONTINENCEDrip2 or DouseInt’l Prostate Symptom Score 50-51OAB-V8 5253Help Me SleepINSOMNIA54-55MEDICATIONSBeer’s56Avoid Too Many57NUTRITIONMeals On SISRisk Factors for Osteoporosis 6465PAINPain Assessment Tool66Pains67PALLIATIVECARE&ENDOFLIFE Pain WisdomManaging End-of-Life Symptoms 68-69PRESSUREULCERSStaging Pressure Ulcers 7071Management Guidelines72SLEEP Epworth QuestionnaireSLU Geriatric Evaluation Mnemonic Screening Tools3
IntroductionMnemonics have long been used as memory aids(especially to assist people in passing examinations).The mnemonics here have been developed becauseof the often complex and multifactorial nature ofillnesses and syndromes in the elderly and the timeconstraints of the present health care environment.These mnemonics are intended to assist the clinician in developing differential diagnoses, risk assessments, or evaluation and management plans forcommon geriatric problems. These mnemonics willalso enable the clinician to do this in a quick, yetcomprehensive manner.The screening tools have been chosen to complement the problems, syndromes, and illnesses that arecovered by the mnemonics.4SLU Geriatric Evaluation Mnemonic Screening Tools
Aging SuccessfullySaint louis University Division of geriatricsPassport to aging Successfully*Please complete this questionnaire before seeing your physician and take it with you when you go.NaMeageBlOOD PReSSURelaying down:standing:WeigHTnow:6 months ago:change:HeigHT at age 20:now:CHOleSTeROl LDL:HDL:VaCCiNaTiONSinfluenza (yearly)PneumococcalTetanus (every 10 years)TSH Date:FaSTiNg glUCOSe Date:Do you SMOKe?How much alCOHOl do you drink?per dayDo you use your SeaTBelT?Do you chew TOBaCCO?eXeRCiSe: How often do you.do endurance exercises (walk briskly 20 to 30 minutes/day or climb 10 flights of stairs)/weekdo resistance exercises?/weekdo balance exercises?/weekdo posture exercises?/weekdo flexibility exercises?/weekCan you See aDeQUaTelY in poor light?Can you HeaR in a noisy environment?are you iNCONTiNeNT?Have you a liViNg Will or durable POWeR OF aTTORNeY FOR HealTH?Do you take aSPiRiN daily (only if you have had a heart attack or have diabetes)?Do you have any concerns about your PeRSONal SaFeTY?When did you last have your STOOl TeSTeD for blood?When were you last screened for OSTeOPOROSiS?are you having trouble ReMeMBeRiNg THiNgS?Do you have enough FOOD?are you SaD?Do you have PaiN?if so, which face bestdescribes your pain?Have you discussed PSA testing with yourdoctor?What is your ADAM score?12FeMaleSMaleS0Do you have trouble passing urine?345When was your last pap smear?When was your last mammogram?Do you check your breasts monthly?Are you satisfied with your sex life?Now, please answer the four questionnaires on the next page.* This questionnaire is based on the health promotion and prevention guidelines developed by Gerimed and Saint Louis University Division of Geriatric Medicine.SLU Geriatric Evaluation Mnemonic Screening Tools5
Aging SuccessfullyAging SucA guide to HeAltH PromPrior to birth0-20 years1. Chooselong-livedparents1. Exerciseregularly20-40 years1. Exercise regularly2. Avoid obesity2. Have yourmotherget regular check-ups duringpregnancy3. Have your mother not smokeor drink alcohol2. Avoidobesity3. Ingest adequatecalcium3. Ingestadequatecalcium4. Eat nutritious foods5. Wear your seatbelt4. Have your mothertake pre-natalvitamins includingfolate.6. Do not smoke ordrink7. Get your vaccinations8. Avoid violence and illicitdrugs4. Eat fish5. Wear yourseatbelt5. Drink inmoderationand do not smoke6. Drive at asafe speed7. Avoidviolence andillicit drugs8. Check your breasts regularly(females)6SLU Geriatric Evaluation Mnemonic Screening Tools
Aging SuccessfullycceSSfullymotionover tHe lifeSPAn40-60 years60-80 years1. Exercise regularly2. Avoid obesity3. Ingestadequatecalcium andvitamin D4. Eat fish5. Wear your seatbelt6. Drink in moderation and donot smoke7. Have yourbloodpressurechecked8. Get yourcholesterol and glucosechecked9. Screen forbreast and coloncancer, highblood pressure,and diabetes10. Have Pap smears (females)11. Have regular mental activityand socialize!12. Avoid takingtoo manymedicines13. Considerhormonereplacement(men)80 1. Exerciseregularly,includingbalance andresistanceexercises1. Exercise regularly,including balanceand resistanceexercises2. Avoid weight loss2. Avoid weight loss3. Ingest adequate calcium andvitamin D3. Ingest adequate calcium andvitamin D4. Be screened for osteoporosis5. Wear your seatbelt4. Eat fish6. Drink in moderation and do notsmoke5. Wear yourseatbelt6. Drink in moderation and do notsmoke7. Screen for breast and coloncancer, high blood pressure,osteoporosis, and diabetes8. Get yourcholesterolchecked9. Have flu andpneumococcal vaccinations10. Have Papsmears (females)11. Have regularmental activityand socialize!12. Avoid takingtoo manymedicinesSee yalater,Doc!7. Have your bloodpressure checked8. Do monthly breast self-exams9. Have flu and pneumococcalvaccinations10. Safety-proof your hometo prevent falls. If you areunsteady, use a cane andconsider hip protectors11. Have regular mental activity.Socialize, and avoid beingdepressed.12. Avoid takingtoo manymedicines13. Keep doing what youare doing.Remember, most ofyour physicians won’treach your age!SLU Geriatric Evaluation Mnemonic Screening Tools7
AlcoholCage Questionnaire For Alcoholism*Ever felt the need to cut down on your drinking?Yes/NoEver felt annoyed by criticism of your drinking?Yes/NoEver felt guilty about your drinking?Yes/NoEver take a morning drink (eye-opener)?Yes/No*Two affirmative answers may be suggestive of alcoholism.Ewing, J Am Med Assoc 252:1905-1907, 1984.Copyrighted 1984, American Medical Association8SLU Geriatric Evaluation Mnemonic Screening Tools
AnticoagulationHemorr2hagesH epatic or renal disease1E thanol abuse 1M alignancy 1O lder (age 75 years)1R educed platelet count or function1R e-bleeding Risk 2H ypertension (uncontrolled)1A nemia 1G enetic factors 1E xcessive fall risk1S troke 1TOTAL SCOREScoring:Risk of Hemorrhage: With each additional point, the rate ofbleeding per 100 patient-years of warfarin increases:1.9 (0.6-4.4) for 02.5 ( 1.3-4.3) for 15.3 (3.4-8.1) for 28.4 (4.9-13.6) for 310.4 (5.1-18.9) for 412.3 (5.8-23.1) for 5Gage BF, et al. Am Heart J 151(3):713-9, 2006.SLU Geriatric Evaluation Mnemonic Screening Tools9
AnticoagulationChads2Risk of Stroke for People with Atrial Fibrillation ifWarfarin* Not UsedC ongestive heart failure1H ypertension 1A ge 75 or older1D iabetes 1S troke or TIA in the past2TOTAL SCORERisk of stroke: With each additional point, the rate of strokeper 100 patient-years without antithrombotic therapy (i.e., theuse of aspirin instead of warfarin) increases:1.9 (95% CI, 1.2-3.0) for a score of 0;2.8 (95% CI, 2.0-3.8) for 1;4.0 (95% CI, 3.1-5.1) for 2;5.9 (95% CI, 4.6-7.3) for 3;8.5 (95% CI, 6.3-11.1) for 4;12.5 (95% CI, 8.2-17.5) for 5;18.2 (95% CI, 10.5-27.4) for 6.Gage BF, et al. Validation of clinical classification schemes for predicting stroke: results from theNational Registry of Atrial Fibrillation. J Am Med Assoc 285(22):2864-70, 2001.*For calculating warfarin dosing, see www.warfarindosing.org.10SLU Geriatric Evaluation Mnemonic Screening Tools
Cancer ScreeningCautionCancer Warning SignsC hange in bowel or bladder habitsA sore that does not healU nusual bleeding or dischargeT hickening or lump in breast or elsewhereI ndigestion or difficulty in swallowingO bvious change in wart or moleN agging cough or hoarsenessSLU Geriatric Evaluation Mnemonic Screening Tools11
DehydrationSimple Screen for DehydrationD rugs, e.g., diureticsE nd of lifeH igh feverY ellow urine turns darkD izziness (orthostasis)R educed oral intakeA xilla dryT achycardiaI ncontinence (fear of)O ral problems/sippersN eurological impairment (confusion)S unken eyesThomas DR, et al. J Am Med Dir Assoc, June 2008.12SLU Geriatric Evaluation Mnemonic Screening Tools
Mental Status: DELIRIUMAcute Change in MSMedications that can Cause or have been Reported to Cause anAcute Change in Mental StatusA ntiparkinson’s drugsC orticosteroidsU rinary incontinence drugsT heophyllineE mptying drugs1C ardiovascular drugs2H 2 blockers3A ntibiotics4N SAIDs5G eropsychiatry drugs6E NT drugs7I nsomnia drugs8N arcotics9M uscle relaxants10S eizure drugs1 E.g., metoclopramide, compazine.2 In particular, centrally-acting drugs (e.g., clonidine), digoxin, some antiarrhythmics.3 Particularly for patients with renal insufficiency because these drugs are renally excreted.4 Although not a common cause of mental status change, several antibiotics have been reported in theliterature in the form of case reports.5 Also not common, but case reports exist.6 A large category because, in general, most of these are centrally-acting.7 Some are worse than others. In general, non-sedating antihistamines are probably safe, butcombination drugs are risky.8 Beware of over-the-counter sleeping agents. Most contain diphenhydramine.9 Usually only seen with acute use, not chronic. Meperidine (Demerol) not recommended in the elderly.10 These are centrally-acting, not locally at muscles.Flaherty JH. Commonly prescribed and over-the-counter medications: Causes of confusion. Clin GeriatrMed 14:101-127, 1998.SLU Geriatric Evaluation Mnemonic Screening Tools13
Mental Status: DELIRIUMCAMThe Confusion Assessment Method Diagnostic AlgorithmFeature 1: Acute Onset and Fluctuating CourseThis feature is usually obtained from a family member or nurse andis shown by positive responses to the following questions: Is thereevidence of an acute change in mental status from the patient’sbaseline? Did the (abnormal) behavior fluctuate during the day, that is,tend to come and go, or increase and decrease in severity?Feature 2: InattentionThis feature is shown by a positive response to the following question: Didthe patient have difficulty focusing attention, for example, being easilydistractible, or having difficulty keeping track of what was being said?Feature 3: Disorganized thinkingThis feature is shown by a positive response to the following question:Was the patient’s thinking disorganized or incoherent, such asrambling or irrelevant conversation, unclear or illogical flow of ideas,or unpredictable switching from subject to subject?Feature 4: Altered Level of ConsciousnessThis feature is shown by any answer other than “alert” to thefollowing question: Overall, how would you rate this patient’s level ofconsciousness? (Alert [normal], Vigilant [hyperalert], Lethargic [drowsy,easily aroused], Stupor [difficult to arouse], or Coma [unarousable]).The diagnosis of delirium by CAM requires the presence of features 1and 2 and either 3 or 4.CAM Instrument and Algorithm adapted from Inouye S, van Dyck E, Alessi C, Balkin S, Siegal A,Horwitz R. (1990). Clarifying confusion: the confusion assessment method. Ann Intern Med 113(12),941-8. Reprinted with permission.14SLU Geriatric Evaluation Mnemonic Screening Tools
Mental Status: DELIRIUMCocoa PhssDifferentiating Delirium from DementiaDeliriumC onsciousnessDementiaO rientationDecreased or hyperalert, Alert“clouded”DisorganizedDisorientedC ourseFluctuatingSteady slow declineO nsetAcute or subacuteChronicA ttentionImpairedUsually normalP sychomotorAgitated or lethargicUsually normalH allucinationsPerceptual disturbances, Usually not presentmay have hallucinationsS leep-wake cycle AbnormalUsually normalS peechSlow, incoherentAphasic, anomic,difficulty finding wordsSLU Geriatric Evaluation Mnemonic Screening Tools15
Mental Status: DELIRIUMDelirium(s)Differential Diagnosis for Patients with Delirium(Remember, delirium usually has more than one cause)D rugs1E yes, ears2L ow O2 states (MI, stroke, PE)3I nfectionR etention (of urine or stool)I ctalU nderhydration/UndernutritionM etabolic(S) ubdural1 See mnemonic ACUTE CHANGE IN MS (page 11)2 Poor vision and hearing are considered more risk factors than true cause, but should be “fixed” orimproved, if possible. Cerumen is common cause of hearing impairment.3 Low O2 state does NOT necessarily mean hypoxia, rather it is a reminder that patients with a hypoxicinsult (e.g., MI, stroke, PE) may present with mental status changes with or without other typicalsymptoms/signs of these diagnoses.16SLU Geriatric Evaluation Mnemonic Screening Tools
Mental Status: DELIRIUMBe Aware PreventRisk Factors for Delirium (B-E A-W-A-R-E) and TargetedInterventions (P-R-E-V-E-N-T) Based on Intervention Trial to PreventDelirium.*B aseline dementia?E ye problems?A ltered sleep/wake cycle?W ater or dehydration problems?A dding 3 medications, especially sedating and psychoactiveones?R estricted mobility?E ar problems?P rotocol for sleep (back massage, relaxation music, decreasednoise, warm milk or caffeine-free herbal tea)R eplenish fluids and recognize volume depletionE ar aids (amplifier or patient’s own hearing aid)V isual aids (patient’s own glasses, magnifying lens)E xercise or ambulation as soon as possibleN ame person, place and time frequently for reorientationT aper or discontinue unnecessary medications. Use alternativeand less harmful medications.* Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent intervention to prevent deliriumin hospitalized older patients. N Engl J Med 340:669-76, 1999.SLU Geriatric Evaluation Mnemonic Screening Tools17
Mental Status: DELIRIUMAvoid RestraintsNon-Pharmacological Approaches to Patients with BehavioralProblems (Associated with Dementia or Delirium)A void exacerbating factorsV ague complaints? May represent delirium or other medicalillnessO ut of room; out of bedI nsomnia protocol (e.g., warm milk, back rub/massage)D istraction techniquesR elatives or friends to sit with/visit patientE nvironmental adaptationsS cheduled acetaminophen for possible painT herapies (RT, PT, OT)R eview medications as cause of problemsA larm on bed; low bedsI Vs or other tubes, monitors bothering patients? Discontinueif possible or “hide” themN urses’ station (bring patient out to station to sit)T oilet frequentlyS ensory impairments? Get glasses, hearing aides18SLU Geriatric Evaluation Mnemonic Screening Tools
Mental Status: DEMENTIASLU Geriatric Evaluation Mnemonic Screening Tools19
Mental Status: DEMENTIADementiaPotential Reversible Causes of DementiaD rugsE yes, earsM etabolic (e.g., thyroid, calcium)E motion (i.e., depression)N ormal pressure hydrocephalus (Wacky, Wobbly, and Wet)T umor (or other space-occupying lesion)I nfection (e.g., neurosyphilis)A nemia (i.e., B12 deficiency)20SLU Geriatric Evaluation Mnemonic Screening Tools
Mental Status: DEMENTIAThe Caring GuideManagement Guidelines for Caregivers of Persons with DementiaT ime1H ome Health2E yes, Ears3C ar4A dvance DirectiveR estraints5I ncontinenceN o G roup Support6G ait7U ndernutrition/UnderhydrationI dentification (ID bracelet)8D rugs9E motions101 Evaluate amount of time caregiver (CG) is spending with patient; consider respite.2 Does CG need help in the home (e.g., choreworker, nursing aide)?3 Impaired communication can be stressful and burdensome for CG. Cerumen is common cause ofhearing deficit.4 Is patient still driving?5 Restraints (especially physical) can be associated with increased agitation.6 The Alzheimer’s Association (AA) is a good source of support groups for CGs. Visit www.alz.org.7 Dementia may be a risk factor for falls.8 Check with the AA for details about their Safe Return program (web or call).9 See mnemonic ACUTE CHANGE IN MS on page 11.10 Both patient and CG are at increased risk for depression.SLU Geriatric Evaluation Mnemonic Screening Tools21
Mental Status: DEPRESSIONGDSGeriatric Depression Scale (Short Form)yes1. Are you basically satisfied with your life?2. Have you dropped many of your activities and interests? yesyes3. Do you feel that your life is empty?4. Do you often get bored?yesyes5. Are you in good spirits most of the time?6. Are you afraid that something bad is going to happen to you? yesyes7. Do you feel happy most of the time?8. Do you often feel helpless?yes9. Do you prefer to stay at home rather than going outyesand doing new things?10. Do you feel you have more problems with memory than most? yes11. Do you think it is wonderful to be alive now?yes12. Do you feel pretty worthless the way you are now?yes13. Do you feel full of energy?yesyes14. Do you feel your situation is hopeless?15. Do you think that most persons are better off than you? yesNONONONONONONONONONONONONONONOScoring: Score one point for each “depressed” answer (in box).Score of 5 suggests probable depression.For other languages, see http://www.stanford.edu/ yesavage/GDS.htmlSheikh JL, Yesavage JA. Clin Gerontol 5:165-72, 1986. Yesavage JA, et al. J Psychiatr Res 17:27, 1983.22SLU Geriatric Evaluation Mnemonic Screening Tools
Mental Status: DEPRESSIONSig E CapsSigns and Symptoms of DepressionS leep problemsI nterest (lack of) (Anhedonia)G uilt/“Worthlessness”E nergy (lack of)C oncentration problemsA ppetite problemsP sychomotor retardationS uicide ideationsSLU Geriatric Evaluation Mnemonic Screening Tools23
Mental Status: DEPRESSIONCornell Scale for Depression in DementiaName Age Sex DateInpatientNursing Home ResidentOutpatientPerson performing evaluation: Clinician Nurse Family Member OtherScoring SystemA unable to evaluate0 absent1 mild or intermittent2 severeBase ratings on symptoms and signs occurring during the week prior to interview.No score should be given in symptoms resulting from physical disability or illness.A. Mood-Related Signs1. Anxiety: anxious expression, ruminations, worryinga 0 1 22. Sadness: sad expression, sad voice, tearfulnessa 0 1 23. Lack of reactivity to pleasant eventsa 0 1 24. Irritability: easily annoyed, short-tempereda 0 1 2B. Behavioral Disturbance5. Agitation: restlessness, handwringing, hairpullinga 0 1 26. Retardation: slow movement, slow speech, slow reactionsa 0 1 27. Multiple physical complaints (score 0 if GI symptoms only)a 0 1 28. Loss of interest: less involved in usual activitiesa 0 1 2(score only if change occurred acutely, i.e., in less than one month)C. Physical Signs9. Appetite loss: eating less than usuala 0 1 210. Weight loss (score 2 if greater than 5 lbs. in one month)a 0 1 211. Lack of energy: fatigues easily, unable to sustain activitiesa 0 1 2(score only if change occurred acutely, i.e., in less than one month)D. Cyclic Functions12. Diurnal variation of mood: symptoms worse in morninga 0 1 213. Difficulty falling asleep: later than usual for this individuala 0 1 214. Multiple awakenings during sleepa 0 1 215. Early morning awakening: earlier than usual for this individual a 0 1 2E. Ideational Disturbance16. Suicide: feels life is not worth living, has suicidal wishes ora 0 1 2makes suicide attempt17. Poor self-esteem: self-blame, self-deprecation, feelings of failure a 0 1 218. Pessimism: anticipation of the worsta 0 1 219. Mood congruent delusions: delusions of poverty, illness, loss a 0 1 2A score of 8 suggests significant depressive symptoms.Alexopoulos G, Abrams R, Young R, et al. Cornell Scale for Depression in Dementia. Biol Psych 23, 271-84,1988.24SLU Geriatric Evaluation Mnemonic Screening Tools
DizzinessBenign Paroxysmal Positional Vertigo (BPPV)BPPV is one of the most common causes of dizziness. It is often characterizedby vertigo that occurs a few seconds after specific head movements, such asrolling over in bed, bending over, or looking upward. The vertigo usuallylasts no more than a minute. The symptoms are most often experienced whenpatients lie down, which distinguishes BPPV from orthostatic hypotension.BPPV may be recurrent.The Dix-Hallpike test is specific for the diagnosis of BPPV.While sitting on an examining table, the patient’s head is turned eitherto the right or to the left by about 45 . The patient is then moved rapidlyfrom a sitting position to a supine position with the head hanging off ofthe back of the examining table while the head continues to be in the same45 position. The patient is instructed to keep his/her eyes open so that theexaminer can see eye movement during the entire procedure. If BPPV ispresent, vertigo will begin after a latency of 5 to 10 seconds and usuallywill last 30 seconds to a minute. Rotary nystagmus will occur and thepatient will complain of dizziness.After the nystagmus and the vertigo subside, the patient is returned to thesitting position. The rotary nystagmus may reverse in direction and thepatient may again experience vertigo. If a positive response occurs, thesame maneuver is repeated. Usually, the severity of the vertigo and therotary nystagmus are reduced during the repeat maneuver. This reductionis termed “fatigue.” The opposite ear is then tested in a similar fashion.The offending ear is the one that is toward the ground when BPPV occursduring the Dix-Hallpike maneuver.Sloane PD. Evaluation and Management of Dizziness in the Older Patient. Clin Geriatr Med 12:785801, 1996. http://www.earaces.com/BPPV.htm. Parts of this are reprinted from http://www.earaces.com/bppv.html with permission from Atlantic Coast Ear Specialists, P.C.SLU Geriatric Evaluation Mnemonic Screening Tools25
DizzinessDurationSeconds tominutes (E)DiagnosisManagementOrthostatic Treat underlying cause; stop orhypotension decrease offending medications.Use medications for posturalhypotension.Impairment in 1 ofOccurs withMultipleCorrect or maximize sensorythe following: vision,ambulation (C) sensory im- deficits; PT for balance andvestibular function, spinalpairmentsstrength training.proprioception, cerebellum, lower-extremityperipheral nervesUnsteady gait with short Occurs withIschemic cer- Aspirin; modification of vascusteps; reflexes and/orambulation (C) ebral disease lar risk factors; PTtone.Provoked by head or neck Seconds toCervicalBehavior modification; reducemovement; reduced neck minutes (E)spondylosis cervical spasm and inflammarange of motiontionLightheadedness1-30 min afterstandingPrimarySymptomFeaturesClassification of DizzinessDizziness26SLU Geriatric Evaluation Mnemonic Screening Tools
SLU Geriatric Evaluation Mnemonic Screening ToolsLow-frequency sensorineural hearing lossand tinnitusVascular disease riskfactors, cranial nerveabnormalitiesAcute onset, non-positionalBrought on by position Seconds tominutes (E)change, positive DixHallpike test (See BPPVon page 49)BenignparoxysmalpositionalvertigoEpley maneuver to repositioncrystalline debris (see www.audiometrics.com/bppv.htm);exercises provoking symptomsmay be of help.Labyrinthitis Consider methylprednisone,Days(vestibular 100mg/d po x 3d with subseneuronitis) quent gradual taper over 3 wksto improve vestibular functionrecovery. Consider meclizine foracute symptom relief.Consider meclizine for acuteMeniere’sMinutes tosymptom relief; diuretics and/ordiseasehours (E)salt restriction for prophylaxis.Aspirin; modification of vascular10 min to sev- TIAsrisk factorseral hours (E)PosturalBehavior modificationimpingementof vertebralarteryNote: C chronic; E episodic.Reuben DB, et al. Geriatrics At Your Fingertips: 2007-2008, 9th edition. New York: The American Geriatrics Society; 2007.VertigoDrop attacks Provoked by head or neck Seconds tomovement, reduced ver- minutes (E)tebral artery flow seen onDoppler or angiographyDizziness27
DizzinessV2ertigo PMV ision problem, hyperVentilationE quilibrium disordersDep R essionT ransient ischemic attacks, heart diseaseI nfarction (cerebral)G rowths (tumors)O rthostatic dysregulationP aroxymal positioning vertigoM edications28SLU Geriatric Evaluation Mnemonic Screening Tools
Elder Neglect or AbuseNeglect AbuseRisk Factors and Clues for Possibility* of Neglect or Abuse**N o money or low incomeE motion (depression) of either patient or caregiverG rave illness (cancer, Alzheimer’s)L oss of weight or dehydrationE arlier evidence of neglect or abuseC ognitive or physical impairmentT oo many or too few doctor/emergency department visitsA lcohol or drug useB ehavioral problemsU nkempt or poor hygieneS kin tears, bruises or soresE asily frightened*Caution should be used before labeling someone neglectful or abusive without complete information.**Neglect and abuse are combined in this mnemonic because it is often difficult to differentiate betweenthe two, and both may be a consequence of the patient’s or caregiver’s circumstances. They may not beintentional.SLU Geriatric Evaluation Mnemonic Screening Tools29
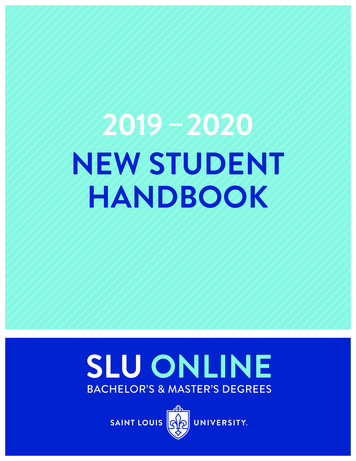
Eyes and EarsSnellen ChartNear Vision AssessmentHold in good light, 14 inches from eye.30SLU Geriatric Evaluation Mnemonic Screening Tools
Eyes and EarsThe Hearing Handicap Inventory for theElderly (HHIE) Screening Version(4 points for each positive answer)Note: One of the most common causes of impaired hearing iscerumen. Always examine ear canals when hearing is abnormal.1. Does a hearing problem cause you to feel embarrassed when youmeet new people?2. Does a hearing problem cause you to feel frustrated when talking tomembers of your family?3. Do you have difficulty hearing when someone speaks in a whisper?4. Do you feel handicapped by a hearing problem?5. Does a hearing problem cause you difficulty when visiting friends,relatives, or neighbors?6. Does a hearing problem cause you to attend religious services lessoften than you would like?7. Does a hearing problem cause you to have arguments with familymembers?8. Does a hearing problem cause you difficulty when listening totelevision or radio?9. Do you feel that any difficulty with your hearing limits or hampersyour personal or social life?10. Does a hearing problem cause you difficulty when in a restaurantwith relatives or friends?Probabilityof hearingimpairment given anHHIE score:Score0-810-2426-40Likelihood ratio (95% CI)0.36 (0.19-0.68)2.30 (1.22-4.32)12.00 (2.62-55.0)Lichtenstein MJ, et al. Validation of screening tools for identifying hearing-impaired elderly in primarycare. J Am Med Assoc 259(19);2875-8, 1988.SLU Geriatric Evaluation Mnemonic Screening Tools31
32I.WALKING SPEEDa. Determine average walking speedb. Determine average walking speed while counting backward from 100by sevensc. If dual tasking doubles the average walking speed then the patientshould be referred to physical therapy.Testing a person’s ability to dual task, to maintain postural control in the concurrentperformance of cognitive tasks, allows healthcare providers to predict a person’s riskof falling. Cognitive function and basic balance can be tested together with some basicparadigms. These include:Good balance requires an interaction of both the central and peripheral nervous systems.In older adults, cognitive ability plays a key role in maintaining that good balance. Withaging, there is a decline in the ability to perform these two tasks (thinking and moving)at the same time (dual tasking). This is a major reason for increasing rates of falls withaging. Persons who are identified as having trouble dual tasking can be treated withphysical therapy to reduce their fall risks.Determining Fall RiskDual TaskingFallsSLU Geriatric Evaluation Mnemonic Screening Tools
II. Get-Up-And-Go Testa. Determine the time required to perform the Get-Up-And-Go testb. Determine the time required to perform the Get-Up-And-Go test whileholding a full glass of waterc. If dual tasking results in doubling the time the person requires toperform the Get-Up-And-Go task, then the person should be referred tophysical therapy.III. DANCINGa. Determine how well a patient can dance a simple waltzb. Determine how well a patient can execute an unexpected turn whilewaltzingc. If dual tasking results in the patient stumbling during the turn, then theperson should be referred to physical therapy.IV. ONE-LEG STANDa. Determine how long a patient can stand on one leg without fallingb. Determine how long a patient can stand on one leg with eyes closedwithout fallingc. If shutting the eyes results in the patient falling in less than half thetime they can stand on one leg without
This book is published by Saint Louis University School of Medicine Division of Geriatric Medicine and the Geriatric Research, Education, and Clinical Center St. Louis VA Medical Center This project is supported by funds from the Division of State, Community and Public He