Transcription
A Special Health Report from Harvard Medical SchoolCoping withANXIETY AND PHOBIASIn this report Recognizing and treatingcommon anxiety disorders The most effectivemedications and therapies Managing panic attacks Advice for worriersHarvardMedicalSchool Anxiety and sleep: Tips forovercoming insomniaPrice: 24.00
Coping with Anxiety and PhobiasA Special Health ReportHarvard Medical School PublicationsFaculty Medical AdvisorMichael Mufson, M.D.Assistant Professor of PsychiatryHarvard Medical SchoolEditorAnn Marie DadolyWriterSusan GilbertEditor, Special Health ReportsKathleen Cahill AllisonIllustratorScott LeightonCopy EditorJames Clyde SellmanProduction CoordinatorAmy E. YeagerSpecial Health ReportsHarvard Medical School publishes SpecialHealth Reports on a wide range of topics. Toorder other reports or additional copies ofthis report, please see the order form at theback of this report.To obtain multiple-copy discount rates, pleasewrite or call:Consumer Health Publishing GroupAttn: SR Bulk Orders1100 Summer St., 2nd FloorStamford, CT 06905(203) 975-8854, ext. 110NewslettersHarvard Medical School publishes thefollowing monthly newsletters:Harvard Health LetterHarvard Heart LetterHarvard Men’s Health WatchHarvard Women’s Health WatchHarvard Mental Health LetterBooksPublished by Harvard Medical SchoolAnthony L. Komaroff, M.D., Editor in ChiefBooks published by Harvard Medical Schoolinclude:The Arthritis Action Program: An Integrated Planof Traditional and Complementary Therapies(Simon and Schuster, 2000)Eat, Drink, and Be Healthy: The Harvard MedicalSchool Guide to Healthy Eating (Simon andSchuster, 2001)Harvard Medical School Family Health Guide(Simon and Schuster, 1999)Copyright 2002 by the President and Fellows ofHarvard College. Written permission is required toreproduce, in any manner, in whole or in part, thematerial contained herein. Submit reprint requestsin writing to:Harvard Health Publications10 Shattuck St., Suite 612Boston, MA 02115(617) 432-1485Fax: (617) 432-4719Healthy Women, Healthy Lives: A Guide toPreventing Disease from the Landmark Nurses’Health Study (Simon and Schuster, 2001)Six Steps to Increased Fertility: An IntegratedMedical and Mind/Body Program to PromoteConception (Simon and Schuster, 2000)Web SiteFor the latest information and mostup-to-date publication list, visit us onlineat www.health.harvard.edu
ContentsWhat Are Anxiety Disorders?. . . . . . . . . . . . 3Links to Depression . . . . . . . . . . . . . . . . . . . . . . . . . 4What Causes Anxiety?. . . . . . . . . . . . . . . . . . 5Genetic Underpinnings . . . . . . . . . . . . . . . . . . . . . . . 5The Brain. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Brain Cell Communication. . . . . . . . . . . . . . . . . . . . 7Hormones and the HPA Axis . . . . . . . . . . . . . . . . . . 8Life Experiences . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Personality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Gender Differences in Anxiety. . . . . . . . . . 12Anxiety in Children and Teenagers . . . . . . 13Anxiety and Aging . . . . . . . . . . . . . . . . . . . . 15Types of Anxiety Disorders . . . . . . . . . . . . . 16Panic Attack. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Panic Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Specific Phobia (Simple Phobia) . . . . . . . . . . . . . . . 18Social Phobia (Social Anxiety Disorder) . . . . . . . . . 19Obsessive-Compulsive Disorder . . . . . . . . . . . . . . . 21Post-Traumatic Stress Disorder(Stress Response Syndrome) . . . . . . . . . . . . . . . . . . 22Acute Stress Disorder . . . . . . . . . . . . . . . . . . . . . . . 24Generalized Anxiety Disorder . . . . . . . . . . . . . . . . . 25Anxiety Disorder Due to a GeneralMedical Condition . . . . . . . . . . . . . . . . . . . . . . . . . 26Substance-Induced Anxiety Disorder. . . . . . . . . . . . 27How Anxiety Is Diagnosed . . . . . . . . . . . . . 28Medical History and General Physical Exam . . . . . 28Screening Tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Psychiatric Evaluation . . . . . . . . . . . . . . . . . . . . . . 28Treating Anxiety . . . . . . . . . . . . . . . . . . . . . . 29What You Should Know About Medications . . . . . . 29Medications for Anxiety Disorders . . . . . . . . . . . . . 31Psychological Therapy for Anxiety. . . . . . . . . . . . . . 34Other Treatments . . . . . . . . . . . . . . . . . . . . . . . . . . 37Exercise for Anxiety . . . . . . . . . . . . . . . . . . . . . . . . 37
ContentsMaking Treatment Work for You . . . . . . . . 38Persist With Treatment. . . . . . . . . . . . . . . . . . . . . . 38Learn to Cope With Stress . . . . . . . . . . . . . . . . . . . 38Don’t Drink Coffee or Smoke . . . . . . . . . . . . . . . . 38Seek Social Support . . . . . . . . . . . . . . . . . . . . . . . . 39On the Horizon . . . . . . . . . . . . . . . . . . . . . . . . 40Comparing Medication andPsychosocial Therapies . . . . . . . . . . . . . . . . . . . . . . 40New Benzodiazepines and Antidepressants . . . . . . . 40New Types of Drugs . . . . . . . . . . . . . . . . . . . . . . . . 40Surgery for Obsessive-Compulsive Disorder . . . . . . 40Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Resources. . . . . . . . . . . . . . . . . . . . . . . . . . . . 42The goal of materials provided by Harvard HealthPublications is to interpret medical information for thegeneral reader. This report is not intended as a substitutefor personal medical advice, which should be obtaineddirectly from a physician.
A S P E C I A L R E P O R T F R O M H A RVA R D M E D I CA L S C H O O LCOPING WITHANXIETY ANDPHOBIASveryone worries sometimes. Everyone gets scared. These are normal, even healthy,responses to threatening situations. But if you feel extremely worried or afraidmuch of the time, or if you repeatedly feel panicky, consider seeking medical advice.Anxiety takes many forms. It can make you so uneasy around people that you isolateyourself, skirting social gatherings and passing up potential friendships. It can fill youwith such obsessive thoughts or inexplicable dread of ordinary activities that youcannot work. Anxiety disorders can be mild, moderate, or severe, but overcoming anxiety generally takes more than just “facing your fears.” Many people need help in dealing with these problems.But getting help has always been easier said than done. As with many mentalhealth issues, there has long been a stigma surrounding anxiety. People are ashamedto admit to phobias and persistent worries, which seem like signs of weakness. Theshame, combined with the tendency of people with anxiety to avoid others, is perhaps the biggest obstacle to relief and recovery. Without treatment, many individualsbecome more fearful and isolated. In extreme cases, they are so imprisoned by theiranxiety that they are unable to leave home.Sigmund Freud regarded anxiety as the result of inner emotional conflict or external danger. While these factors often contribute to anxiety, scientists now know thatanxiety disorders are biologically based illnesses. Indeed, the last 30 years have transformed our understanding of anxiety. Sophisticated brain imaging equipment hasmade it possible to trace the neural pathways of fear and anxiety. In the process, scientists have discovered certain abnormalities in the brainsof anxiety sufferers. Research also suggests that genes maycontribute to these abnormalities. While there are still morequestions than answers, our growing knowledge about anxiety has already led to safer, more effective treatments.Anxiety disorders, which include panic attacks andphobias, are among the most common mental illnesses,affecting about 19 million American adults and millions ofchildren. For every individual with an anxiety disorder,many more are affected by it, including spouses, children,other relatives, friends, and employers.EMany ordinary situations, suchas driving through a tunnel, cantrigger the symptoms of anxiety.
A Harvard Medical School ReportOn the other hand, never before have there been so many therapies to help control anxiety and preserve the relationships that can be undone by it. Medicationscan, in many cases, reduce or eliminate anxiety symptoms. Several types of therapy,especially cognitive-behavioral therapy, also help control anxiety by teaching peopleto adopt more positive thought and behavior patterns. Some medications nowbeing developed may even help prevent anxiety disorders in people who are genetically predisposed to them.This report will provide up-to-date information about the causes and treatmentsof anxiety disorders. But we hope that it will give you something more: an incentiveto seek help and feel better.COPING WITH ANXIETY AND PHOBIAS2
3What Are Anxiety Disorders?t’s likely that if you ask any two people with ananxiety disorder to describe it, they’ll paint different pictures. One person might dread speaking in public, while another is gripped by intense fear at the merethought of getting on an airplane. Someone else mightdescribe herself as a “chronic worrier,” because she regularly frets about all sorts of things. Another experiencesunpredictable episodes of panic, with shortness ofbreath, sweating, and chest pains. Many people wouldundoubtedly mention that they have trouble sleeping.Why the broad array of symptoms? It’s becauseanxiety disorders aren’t actually a single condition, butrather a spectrum of related disorders, including panicattacks, panic disorder, phobias, obsessive-compulsivedisorder, post-traumatic stress disorder, generalized anxiety disorder, anxiety due to a medical condition, andITable 11.substance-induced anxiety. (See “Anxiety Disorders ata Glance,” below.) However, some of the same imbalances in brain chemistry are thought to underlie manydifferent anxiety disorders, which helps explain whymore than half of all people with one anxiety disorderalso have another. While each anxiety disorder has itsown set of symptoms, they also have some symptomsin common. (See “Common Symptoms,” page 4.)It’s not that people with anxiety disorders havethese symptoms and other people don’t. At some time,most people feel afraid, tense, or even anxious enoughto become short of breath. The difference is that individuals who don’t have anxiety disorders experiencethese reactions in response to genuine threats. For example, a fire is raging in the house next door, or yourcar breaks down, leaving you stranded on a desertedAnxiety Disorders at a GlanceTypeMain SymptomsSee PagePanic AttackA sudden wave of intense apprehension, fearfulness, or terror, with physicalsymptoms such as shortness of breath, palpitations, and chest pains.16Panic DisorderRecurrent panic attacks that occur suddenly and without warning, and causepersistent concern. Attacks often occur for no apparent reason.17Specific Phobia(Simple Phobia)Substantial anxiety caused by exposure to a particular feared object or situation.18Social PhobiaSubstantial anxiety caused by certain social situations or performing in front ofa group.19ObsessiveCompulsiveDisorderRecurrent distressing thoughts and uncontrollable repetitive behaviors intendedto reduce anxiety provoked by those thoughts. Symptoms last more than 1 houra day and cause significant distress or interfere with normal functioning.21Acute StressDisorderAnxiety symptoms that last for up to 1 month following a traumatic experience.24Post-TraumaticStress DisorderDistressing thoughts, anger, and other anxiety symptoms that occur for more than1 month following a life-threatening or severe traumatic experience.22GeneralizedAnxiety DisorderExcessive anxiety and worry about a variety of things on most days for at least 6months. Physical symptoms, such as muscle tension, increased heart rate, anddizziness, may also occur.25Anxiety DisorderDue to a GeneralMedical ConditionPronounced anxiety, panic attacks, obsessions, or compulsions caused by a ced anxiety, panic attacks, obsessions, or compulsions caused by amedication, drug abuse, or exposure to a toxin.27
4A Special Health Report from Harvard Medical School!Common SymptomsThe following symptoms are characteristic of allanxiety disorders: Irrational feelings of fear, dread, or danger Tension Worry Physical symptoms such as agitation, trembling,nausea, hot or cold flashes, dizziness, shortnessof breath, or frequent urinationhighway at 3 a.m. In such situations, anxiety can be alifesaver, spurring you to flee the area near the burningbuilding or to call the police for help. But people withanxiety disorders face worry and fear in ordinary, relatively harmless situations. For example, while tappingthe keyboard of a computer, they may fear contractinga life-threatening virus (a sign of obsessive-compulsivedisorder). They may be gripped by worry nearly everyday about getting into a car accident, losing their jobs,having their children do poorly in school, or other possible but unlikely prospects (a sign of generalizedanxiety disorder). People with anxiety disorders arehypersensitive to the possibility of danger, but their extreme vigilance serves no purpose. They are spinningtheir neurological wheels, so to speak.It’s possible to live with mild anxiety disorders.But when the anxiety is severe enough to interfere witheveryday life, treatment is usually the only way to control the disorder. Treatment options include medication, psychotherapy, or both. Without treatment, it’slikely that the disorder will worsen or that anotheranxiety disorder will develop. Treatment is also important for conditions such as depression and alcohol ordrug dependence that often accompany anxiety.Links to DepressionAbout 20%–30% of people with anxiety disorders alsosuffer from depression. Some have the two conditionssimultaneously, while others have one first, recoverfrom it, and then develop the other. Anxiety can alsobe a symptom of depressive disorders, and depressioncan be a symptom of anxiety disorders.The two are much more closely linked than wasonce thought. Scientists have found that the same kindof abnormalities in neurotransmitters (chemical messengers) that promote depression can also trigger anxiety. For example, the brain structures that react toperceived threats are hypersensitive in some people withdepression, as well as in some with anxiety disorders.Given the similarity of the two conditions, it’s no surprise that most of the medications used to treat anxiety are antidepressants.What If You Are Just Plain Worried?Not everyone who suffers from frequent worry has an anxiety disorder. Perhaps you are one of the many “worried well.”If you don’t have an anxiety disorder, but think you worry too much, the following advice may help you lighten up. Practice relaxation techniques.Listen to music or to relaxationrecordings to take your mind offwhatever is worrying you. Progressive muscle relaxation, a technique in which you relax one setof muscles at a time, can alsorelieve tension. Exercise regularly. Studies havefound that exercise improvesmood and modestly decreasesanxiety symptoms. Particularexercises are less important thanfrequency. Exercise regularly. Aimfor at least 30 minute of moderateactivity on all, or most, days. (See“Exercise for Anxiety,” page 37.) Consider biofeedback. If the techniques mentioned above don’t dothe trick, biofeedback may help.Biofeedback helps you becomemore aware of your body’s responses to stress and teaches youto control them using relaxation andcognitive techniques. A clinicianwho is experienced in biofeedbackcan help you do so by measuringspecific body functions, such asheartbeat, and feeding them back toyou in the forms of sounds or lights.(See “Biofeedback,” page 37.)
What Causes Anxiety?5ders. One study found that this genetic variation wasany people assume that anxiety arises from amore than three times more common in people withtraumatic event or overwhelming stress. Whilegeneralized anxiety disorder than in a control group.it’s true that experiences such as the death of a parentIt was also more prevalent in people with obsessiveduring childhood or another early trauma can play acompulsive disorder.significant role, these kinds of events aren’t always atIn a 2000 study in the Journal of Abnormal Psycholthe root of the problem. Not everyone who has livedogy, researchers took blood samples from 72 people tothrough a tragedy or terrifying occurrence develops ansee who had the 5-HTT gene variation. The particianxiety disorder, and not everyone who develops anpants then breathed a carbon dioxide-oxygen mix thatanxiety disorder has endured these ordeals. New recauses shortness of breath, a sensation that sometimessearch suggests that anxiety is partly genetic. Certainprovokes fearfulness and anxiety. The test only progenetic variations may cause imbalances in brain chemvoked fear among those with the genetic variation. It’sistry that can predispose someone to anxiety. The bioimportant to note that none of the parlogical tendency toward anxiety may be latentticipants—even those with the gene varifor years until an exceptionally stressful event It’s unlikelytriggers its expression.that there’s any ant—had symptoms of anxiety disordersbefore the experiment. Thus, the findingsingle anxietysuggests that the 5-HTT gene variationgene. ManyGenetic Underpinningsdoesn’t cause anxiety by itself, but sets thegenesprobablystage for anxiety to develop in response toPeople with a parent or sibling who has had ana sufficiently stressful situation.anxiety disorder are at greater risk of developing work togetherone. For many years, experts debated whether to induce theMore Genes Suspectedthis link was due to nature (a genetic predis- disorder.position that’s passed from one generation toResearchers are currently investigatingthe next) or nurture (anxiety-provoking behaviors thatseveral other genes that may help trigger anxiety. Aare learned in families or are caused by stressful exduplication on a region of chromosome 15 is espeperiences growing up). It’s now clear that these factorscially common in families with high rates of panicoften interact.disorder and phobia, according to a 2001 study inStill, much is unknown, and the genetics are hardlyCell. Potential genetic markers for panic disorder havestraightforward. Researchers studying families with aalso been found on chromosomes 1 and 11, and a poshistory of anxiety disorders have scrutinized their gensible marker for agoraphobia (see page 19) was foundetic makeup in hope of finding certain common feaon chromosome 3.tures. Several candidates have been identified. SomeTaken together, these findings amount to early eviare variants of genes, while others are regions on chrodence of a genetic basis for anxiety disorders. But bemosomes that seem similar. But none of these geneticcause the study of genes related to anxiety is in itstraits appear uniformly in people with anxiety disorinfancy, the particular genes involved and how their varders. Therefore it’s unlikely that there’s any single “anxiations induce anxiety have yet to be uncovered. Thusiety gene.” Many genes probably work together tofar, no genetic tests are available to determine whetherinduce the disorder.an individual is at higher risk for anxiety.MOne Anxiety Gene UncoveredSo far, one anxiety-related gene has been identified inhumans: 5-HTT. It regulates serotonin, a neurotransmitter that affects mood. A variation of this genespeeds the neurons’ metabolism of serotonin, leavingless of the chemical available in the brain. Low levelsof serotonin seem to be characteristic of anxiety disorders, depression, and other mental health disor-The BrainFor decades, scientists have believed that anxiety resultsfrom abnormalities in brain chemistry. They based thisconviction on the effects of drugs that reduce anxiety byincreasing the availability of certain neurotransmittersin the brain. The first antianxiety drugs were benzodiazepines, which raise levels of the neurotransmitter
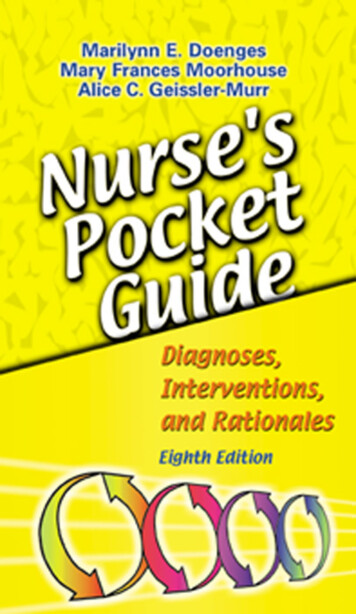
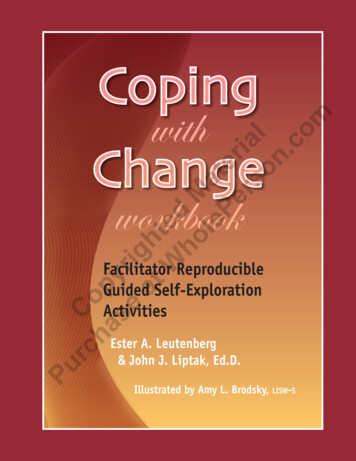
6A Special Health Report from Harvard Medical SchoolAmygdala. The amygdala, a small structure deepin the brain (see Figure 1, below), coordinates the body’sfear response. The amygdala is part of the limbic system, a complex group of structures associated withemotions. In the face of danger, two brain circuits areactivated. One circuit feeds sensory information aboutthe danger—the sight of the burning building, the smellof the fire, and so on—to the cerebral cortex, which isRegions That Influence Anxietythe thinking part of the brain. The cerebral cortex evaluates this information and makes a rational judgmentNew brain imaging technologies have begun to anabout it. For example, that judgment may determineswer some of these questions. Positron emission tomogthat the fire is small, but tell you to get out of the houseraphy (PET), functional magnetic resonance imaginganyway and call the fire department.(fMRI), and other tools have allowed scientists toThe other circuit relays the sensory informationobserve brain activity even while an anxiety attack isto the amygdala, which sends impulses to the autooccurring. These images have helped identify the strucnomic nervous system. This system triggers the “fighttures and circuits that are active when an anxiety attackor-flight” response even before the cerebral cortexstrikes. The use of this technology to study mental illhas made sense of the information. Once activated, itnesses is new, but here’s a summary of what has beenincreases heart rate, routes blood to muscles, releasesdiscovered:stress hormones and glucose into the bloodstream, and spurs other responses to help youfight off or flee danger.The amygdala stores memories of frightening and other emotional experiences. Inpeople with anxiety disorders, the amygdalamay be so sensitive that it overreacts in situations that aren’t threatening. Research onanimals suggests that different parts of theamygdala are activated for different anxietydisorders.Hippocampus. Another brain structure inCerebralthe limbic system, the hippocampus has a cencortextral role in processing emotions and longAmygdalaterm memories. Research has found that thehippocampus is smaller than normal in someHippocampuspeople with post-traumatic stress disorderLocus ceruleusBrain stem(see page 22). It’s also smaller in some womenwho were abused as children, an experiencethat increases the risk for post-traumatic stressdisorder and other anxiety disorders. But it’sThe Brain and Anxietyunclear whether the response to the traumaSeveral regions of the brain influence anxiety. The amygdala isassociated with emotions and coordinates the body’s responsemakes the hippocampus smaller or whether itto fear. The cerebral cortex evaluates data about a perceivedwas already small in certain individuals and itsthreat and forms judgments about it, shaping the response tosize predisposes them to anxiety disorders.fear. The hippocampus processes emotions and long-termLocus ceruleus. The locus ceruleus is anmemories. The locus ceruleus helps determine which stimuliareaof the brainstem that helps determinedeserve attention.which brain stimuli are worth paying attentionFigure 1.to. In experiments with animals, when the lo-gamma-aminobutyric acid (GABA). Later, drugs that increase serotonin levels and affect norepinephrine andother neurotransmitters associated with mood alsoproved effective. But these findings have raised evenmore questions. For example, what brain structuresare involved? What malfunctions in the brain induceanxiety? And what role do neurotransmitters play?
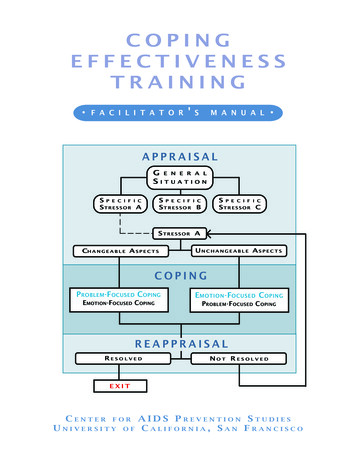
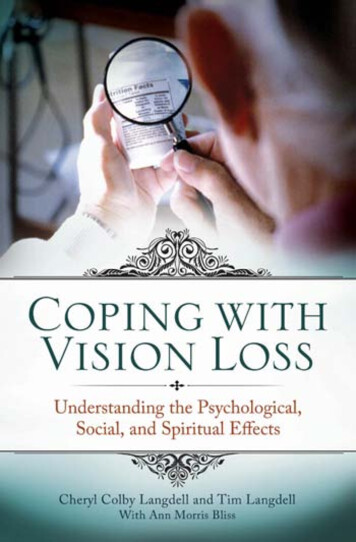
Coping with Anxiety and Phobiascus ceruleus was electronically stimulated, the animals displayed anxiety-like symptoms. Some researchers speculate the same may be true in humans.Brain Cell CommunicationUnderstanding the intricate workings of neurons andneurotransmitters can help identify the sources ofanxiety disorders and may lead to the developmentof treatments.How Neurotransmitters WorkIf you trained a high-powered microscope on a slice ofbrain tissue, you might be able to see a loosely braidednetwork of neurons, or nerve cells, that send and receive messages. Stretching from each neuron are short,branch-like fibers called dendrites and one longer, moresubstantial fiber called the axon. At the end of the axonis the axon terminal.Communication within and between neurons isconveyed by a combination of electrical and chemical signals. (See Figure 2, below.) When a nerve cellbecomes activated, it passes an electrical signal calledan action potential down the axon to the axon terminal, where chemical messengers known as neurotransmitters are stored. The electrical signal releasesneurotransmitters into the space between the firstneuron and the dendrite of a neighboring one, whichis called the synapse. As the concentration of a neurotransmitter rises in the synapse, neurotransmittermolecules begin to bind with receptors embedded inthe membranes of the two nerve cells.The release of a neurotransmitter from one neuron can activate or inhibit a second neuron. If the signal is activating, or excitatory, the message continuesto pass further along that particular neural pathway. Ifit’s inhibitory, the signal will be suppressed. The neurotransmitter also affects the neuron that released it.Once a certain amount of the chemical has beenreleased, a feedback mechanism instructs the neuronto stop pumping it out and to start bringing it backinto the cell. This process is known as reabsorption orreuptake. Enzymes break down the remaining neurotransmitter into smaller molecules.When the System FailsAt optimal levels, the neurotransmitters of the centralnervous system enable people to feel, learn, and move—in general, to function properly. But these complexsystems can go awry. For example, receptors may beoversensitive or insensitive to a specific neurotransmitter.The response to its release, therefore, could be excessiveor inadequate. The supply of a neurotransmitter may beinadequate because a cell pumped out too little or anoverly efficient reuptake mopped up too much beforethe chemical had a chance to bind to the receptors onAxonSynapseHow Neurons Communicate1 Electrical signal travels down neuron12 Chemical neurotransmitter is released53 Neurotransmitter binds to receptor site4 Signal continues into new neuron5 Reuptake occurs; neurotransmitter istransported back into the cell thatreleased itNeurotransmitter234Figure 2.7Receptor site
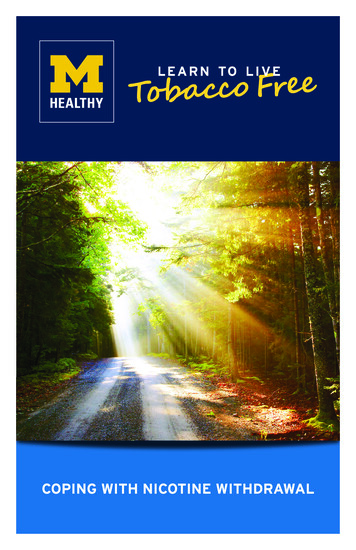
8A Special Health Report from Harvard Medical Schoolfear conditioning, and stress response. Excess norepinephrine may trigger anxiety. Most neurons that release norepinephrine are located in the locus ceruleus,Neurotransmitters and Anxietya part of the brain that may induce anxiety when itmalfunctions.The following neurotransmitters are known to play aDopamine: perhaps best known for being essentialrole in anxiety:to movement. Dopamine, when not available in suffiGamma-aminobutyric acid (GABA): an amino acidcient quantities, leads to the movement difficulties charknown as an inhibitory neurotransmitter because it’sacteristic of Parkinson’s disease. Dopamine also seemsthought to hinder the activity of other neurotransmitto influence motivation and reward.ters; it may help quell anxiety.Although there’s little evidence linking dopamine toSerotonin: helps regulate mood, sleep, and appeanxiety in people, some research suggests a connectiontite, and inhibits pain; people with anxiety are believedto social phobia. For one thing, people who take medto have low levels of serotonin in the brain. Low levelsications that block dopamine sometimes develop socialof serotonin are also linked to depression.phobia. In addition, dopamine-enhancing antidepresNorepinephrine: constricts blood vessels andsants, such as monoamine oxidase (MAO) inhibitors,raises blood pressure; it plays a role in sensitization,are more effective in treating social phobia than tricyclic antideA. Too little neurotransmitter releasedpressants, which have little effecton dopamine.On the other hand, too muchLack ofFailures in Neurondopaminemay contribute orderCommunicationin some patients. The antidepresFailures in the way neuronssant buspirone (BuSpar), whichcommunicate can affect moodblocks dopamine slightly, hasand anxiety. There are severalbeen helpful for some people withcauses of such failures, including the two shown here. As theobsessive-compulsive disorder.other neurons. (See Figure 3, below.) Any of these systemfailures can significantly affect mood and anxiety.first illustration reveals, sometimes the cell that is releasingthe signal doesn’t releaseenough of the neurotransmitter.Or, as the second illustrationshows, the neuron releasesenough of the neurotransmitter,but reabsorbs too much of ittoo quickly, so it doesn’t bindadequately to the receptorsites of the neighboring cell.Receptor sitesNeurotransmitterB. Reabsorbs too much neurotransmitterReabsorbedneurotransmitterReceptor sitesFigure 3.NeurotransmitterHormones and theHPA AxisWhile neurotransmitters helptransmit signals along nerve pathways, other chemicals, called hormones, carry messages to organsor groups of cells throughout thebody. Imbalances of certain hormones increase the risk for anxiety and induce anxiety symptoms.These hormones circulate in apathway called the hypothalamicpituitary-adrenal (HPA) axis, whichinfluences mood. The hypothalamus is a part of the brain aboveyour brainstem, the pituitary glandsits below your brain, and theadrenal glands are located atop
Coping with Anxiety and Phobiasyour kidneys. Together these bodies govern a multitude of hormonal activities in the body and may playa role in anxiety disorders. The autonomic nervous system, which triggers the fight-or-flight response and directs functions throughout the body, starts in thehypothalamus. (See Figure 4, bel
Specific Phobia Substantial anxiety caused by exposure to a particular feared object or situation. 18 (Simple Phobia) Social Phobia Substantial anxiety caused by certain social situations or performing in front of 19 a group. Obsessive-Recurrent distressing tho