Transcription
CROWNS INPEDIATRIC DENTISTRY
INTRODUCTION Treatment of severely decayed primary teeth isone of greatest challenges to pediatric dentists. A higher esthetic standard is expected by parentsfor restoration of their children’s carious teeth. Thus the choice of full coverage restorations forprimary teeth must provide an aestheticappearance in addition to restoring function anddurability.
CLASSIFICATION OF CROWNSi) ACCORDING TO ESTHETICSa) Esthetics : Polycarbonate crown,Strip crown,Preveneered crown,Artglass Crown,Pedo jacket crown,Pedo pearls,Cheng crown,Dura crown,New millenium crown.b) Non esthetics: Stainless steel crownii)ACCORDING TOPOSITION IN ARCHa) Anterior crownsb) Posterior crownsGarg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry. Journal of Advanced Medical and Dental SciencesResearch, 2016; 4(2): 41-26.
iii) ACCORDING TO BONDING ABILITY WITHTOOTH:LUTED CROWNS SS crownsVeneered stainless crownZirconia crownsPolycarbonate crownsPedo pearlsBONDED CROWNS Strip crownsPedo jacket crownsNew millennium crownsART glass crownsGarg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry. Journal of Advanced Medical and Dental SciencesResearch, 2016; 4(2): 41-26.
STAINLESS STEELCROWN It is defined as prefabricated crown forms that are adapted toindividual teeth and cemented with a biocompatible cement. Stainless steel crown was introduced by Rocky MountainCompany (1947) & popularized by Dr William Humphrey in1950Marwah N. Textbook of Pediatric Dentistry,3rd ed. Jaypee;2014.
CLASSIFICATION OF STAINLESS STEELCROWN1. BASED ON COMPOSITION2. BASED ON SIZE3. BASED ON SHAPE4. COMMERCIALLYAVAILABLE
BASED ON COMPOSITION1. STAINLESS STEEL (18:8)17-19% Cr8-13% Ni67% Fe2. NI-BASED CROWNS (ICONEL 600)72% Ni14% Cr6-10% FeGarg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry. Journal of Advanced Medical and Dental SciencesResearch, 2016; 4(2): 41-26.
BASED ON SIZE Stainless steel crowns are available in six sizes forboth primary molars and permanent first molars. Sizes 4 and 5 are the most often used. Size 7 is available for extra large teeth.Garg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry. Journal of Advanced Medical and Dental SciencesResearch, 2016; 4(2): 41-26.
BASED ON SHAPE Untrimmed: long, usually requires trimmingeg- Rocky mountain Pretrimmed or pre festooned: short in lengthbut are not contoured & has parallel sides.eg- Unitek, 3M, Denvo crowns Precontoured: Designed to snap over preparation without anyalterationseg- Ni-Chromium crowns, Unitek, 3M
INDICATIONS1. Extensive decay in primary & youngpermanent teeth2. Restoration of fractured molars3. Following pulp therapy4. Children with bruxism5. Teeth with developmental defects6. Abutment for a space maintainer ordentureGarg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry. Journal of Advanced Medical and Dental SciencesResearch, 2016; 4(2): 41-26.
CONTRAINDICATIONS1. More than two thirds of roots are resorbed2. The tooth exhibits excessive mobility3. Patients with nickel allergies
ADVANTAGES Superior to multi-surface restorations with respectto durability and replacement Better retention and resistance More acceptable to patient & dentist More cost effective – comparatively simpleprocedure restoring even severely affected primaryteeth.DISADVANTAGE Poor aestheticsGarg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry. Journal of Advanced Medical and Dental SciencesResearch, 2016; 4(2): 41-26.
Step by Step Procedure for Crown PreparationCrown selectionPreoperative occlusal evaluationRubber Dam applicationWedges placementTooth preparationCrown adaptationCrown contouringCrown finishingCementationPost cementation instructions
STEPS Crown selectionSelect smallest crown that restores pre existing proximalcontacts Factors to be considered MD width of tooth- Measured with calipers & matchedwith the SSCHeight of crown- Same as that of uncut tooth withcervical margin not more than 1 mm below & parallel tothe gingival marginLight resistance to seatingCasamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy through Adolescence, 5th ed.Elsevier;2013.
TOOTH PREPARATION OCCLUSAL REDUCTIONThe cusp height & marginal ridge of adjacent teeth givesoperator a good baseline to judge the amount of occlusalreduction.Bur: No. 330 or tapered diamond burCasamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy through Adolescence,5th ed.Elsevier;2013.
PROXIMAL REDUCTION Contact area should be cleared with ledge or shoulder free 69L or 169L tapered fissure bur is used to reduce Gingivoproximal line angle should have feather edge finishlineTandon S. Textbook of Pedodontics, Vol 1, 3rd ed. Paras Medical Publishers, Dharya Ganj, New Delhi, 2018.
BUCCAL & LINGUALREDUCTION Only minimal reduction is required Buccal & lingual cervical bulges canbe left uncut if they do not interferein placement of crown. FINISHING All line angles must be rounded Occlusobuccal & occlusolingual lineangles are rounded by holding thebur at a 30-45o angle to the occlusalsurface & sweeping it in a mesiodistaldirectionCasamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy through Adolescence, 5th ed.Elsevier;2013.
EVALUATION CRITERIA FOR TOOTHPREPARATION (TRAUTMAN)1. Occlusal clearance- 1.5-2mm2. Proximal reduction towards occlusal and lingual followingnormal proximal contour3. An explorer can be passed between prepared tooth atgingival margin4. B/L reduced 0.5mm, reduction ending in featheredge 0.51mm into gingival sulcus5) B/L surfaces converge slightly towards occlusal surface6) All point & line angles are rounded and smoothed.Casamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy through Adolescence, 5th ed.Elsevier;2013.
TRIAL ADAPTATION OFCROWN Place crown on lingual side & rotate ittowards buccal side (crown should fitloosely with 2-3mm excess) With scaler scratch line around gingivalmargin on crown Cut crown with crown & bridge scissor1mm below scratch line Retry crown on tooth, if there is blanchingof gingivaTandon S. Textbook of Pedodontics, Vol 1, 3rd ed. Paras Medical Publishers, Dharya Ganj, New Delhi, 2018.
CROWNCONTOURING Contouring is done at middle 1/3rdof crown with a No. 114 plier toproduce a belling effect This gives crown a more evencurvatureTandon S. Textbook of Pedodontics, Vol 1, 3rd ed. Paras Medical Publishers, Dharya Ganj, New Delhi, 2018.
CROWN CRIMPINGCrimping done at cervical 1/3rd ofcrown with a No. 800-417 plierThis aids in:-- Mechanical retention of thecrown- Protection of cement fromexposure to oral fluids- Maintenance of gingivalhealthTandon S. Textbook of Pedodontics, Vol 1, 3rd ed. Paras Medical Publishers, Dharya Ganj, New Delhi, 2018.
FINAL ADAPTATION OF CROWN1. The crown must fit snugly against preparation.2. It cannot be removed with fingers3. Crown margins should extend 1mm gingiva togingival crest & should closely engage toothstructure on all surfaces4. It should seat without cutting or blanching gingiva5. When in occlusion should permit closure withoutinterference.Casamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy through Adolescence, 5th ed.Elsevier;2013.
CROWN FINISHING Use a large green stone to make aknife edge finish at cervical margin Smooth and polish margins with arubber wheelCEMENTATION After removing debris tooth surface is dried.GIC, ZnOE, ZnPO4 are used1/2 or 2/3rd crown is filled with cementSeated on tooth along predetermined path ofinsertion Occlusion is rechecked & excess cement isremoved
POST CEMENTATION INSTRUCTIONS Avoid heavy chewing with crowns for 24 hrs Recall on next day to check hypersensitivity reaction atgingival margin Maintenance of oral hygiene Recalled once every 6 months for evaluationCasamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy through Adolescence, 5th ed.Elsevier;2013.
CAUSES OF STAINLESS STEEL CROWNFAILURES Improper cementation methods with lost crown oropen margins Poor crown adaptation and subsequently poorretention. Failure to pulp treatment. Recurrent caries especially in the interproximal areas.Tandon S. Textbook of Pedodontics, Vol 1, 3rd ed. Paras Medical Publishers, Dharya Ganj, New Delhi, 2018.
SS CROWN STERILIZATION According to AAPD Guidelines for Infection Controlin the Dental Health-Care Setting 2003, stainlesssteel crowns falls in category of critical instrument (itis one which penetrates soft tissue or bone, contactsblood stream or other sterile tissue). For all critical dental instruments that are heatstable, sterilization by steam under pressure, that is,autoclave is advocated.
STAINLESS STEEL CROWN MODIFICATIONS Mink & Hill (1971) :1. Undersize tooth or the oversize crown.2. Oversize tooth or undersize crown.3. Deep sub gingival caries4. Open contactOther modifications:a) Open-faced stainless steel crown. (Hartman CR , 1983)b) Additional tooth reduction or adjacent stainless steelcrowns witharch length loss (McEvoy ,1977)
Sajjanshetty S, Patil PS, Hugar D, Rajkumar K. Pediatric preformed metal crowns - An update. Journal of Dentistryand Allied Science, 2012; 1(2): 29-32.
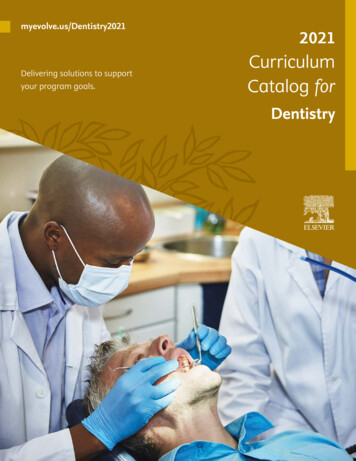
Oversized tooth & undersized crown A vertical cut is made on the buccalsurface of the crown. The margins are pulled apart and anadditional piece of band material is spotwelded to the buccal surfaceDeep subgingival cariesIt can be done by lengthening the crown with aspot welded and soldered piece of bandmaterial.
OPEN FACED STAINLESS STEEL CROWN In anterior teeth SSC’s can be modified by this method. Labial surface trimmed away to leave a crown perimeter which isthen restored with a resin veneering .Yang JN, Mani G. Crowns for primary anterior teeth. International Journal of Pedodontic Rehabilitation, 2016; 1: 75-78.
ADVANTAGESDISADVANTAGESThe aesthetics are fairThe time for placement is long.They are very durable andretentivePlacement of the compositefacing may be compromisedwhen gingival hemorrhage ormoisture is present or whenthe patient exhibits less thanideal cooperationThe materials are fairlyinexpensiveYang JN, Mani G. Crowns for primary anterior teeth. International Journal of Pedodontic Rehabilitation, 2016; 1: 75-78.
VENEERED STAINLESS STEEL CROWNS Available with variety of facing materials such as compositeresin or thermoplastic resin bonded by a variety ofmechanical & chemical bonding approaches to ssc’s.Yang JN, Mani G. Crowns for primary anterior teeth. International Journal of Pedodontic Rehabilitation, 2016; 1: 75-78.
ADVANTAGESThey arepleasing.DISADVANTAGESaesthetically They are 3 times more expensivethan stainless steel, strip andpolycarbonate crownsThey have the durability of As crimping is limited to linguala steel crownsurfaces there is not closeadaptation of crown to tooth.There are reports of the veneerfacing fracturing, however it canbe easily repaired using the openfaced stainless steel crowntechniqueYang JN, Mani G. Crowns for primary anterior teeth. International Journal of Pedodontic Rehabilitation, 2016; 1: 75-78.
COMPOSITE STRIPCROWNS Composite strip crowns are compositeforms filled celluloid crowns.Composite Strip Crowns Technique Select primary celluloid crown form witha mesiodistal width equal to tooth byplacing incisal edge of crown againstincisal edge of tooth. Remove caries with a medium-largeround bur.
Reduce interproximal surfaces by 0.51mm. Interproximal walls should beparallel & gingival margin should befeather edge. Reduce facial surface-1mm & lingualsurface-0.5mm. Round all line angles. Trim selected crown by removing collarand with scissors. Place a small vent hole on mesial distaledge surface with a bur or explorer toallow escape of trapped air whencomposite filled crown is seated. Fit the crown on the prepared tooth.
Select appropriate shade of composite& fill crown with resin. Etch & apply bonding agent. Seat filled crown form on tooth. Remove excess material from vent hole. Light cure from both sides. Remove celluloid form by cutting materialwith composite finishing bur or scalpel. Adjust occlusion & smoothing gingivalmargins
ADVANTAGESDISADVANTAGESIt provides superior aesthetics & It is extremely technique sensitivethe cost of materials arereasonableThe time required for placement Adequate moisture control mightis reasonable.be difficult on an uncooperativepatientLeaves smooth shiny surfaceNot recommended on patientswith a bruxism habit or a deepbite A study by Tate, et al. in 2002 showed that composite strip crownshad a failure rate of 51%, compared to an 8% failure rate of stainlesssteel crowns.Yang JN, Mani G. Crowns for primary anterior teeth. International Journal of Pedodontic Rehabilitation, 2016; 1: 75-78.
CHENG CROWNS Anterior stainless steel crowns faced with a high qualitycomposite (mesh-based with a light cured composite.)Advantages: Completed in one visit Natural looking Stain resistant Doesn’t cause wear of opposing teethDisadvantages: Fracture of veneers during crimping Expensive
PEDO COMPU CROWNS Pedo Compu crowns are also stainless steel crownswhich a high-quality composite facing and meshbased with a light-cured composite crown. Like Cheng crowns, they are also plaque resistant andhave good color stability.
WHITER BITER CROWNS These crowns have a polymeric coating withpolyester/epoxy hybrid composition. Although the coating is thin, it does not peelor chip easily.
POLYCARBONATE CROWNS Polycarbonate crowns are heat-molded acrylicresin shells that are adapted to teeth with selfcured acrylic resin.
Nu Smile CROWNS SpeciallyFormulatedHybridCompositeSubstructure 2 shades for Anterior Crowns (XL & NL). 1 shade for Posterior Crown (XL only)
Advantages: Single appointmentEasy placement techniqueReduces operatory timeLess technique sensitiveDisadvantages: More tooth preparation due to their greater bulk. Avoid crimping - facing susceptible to fracture, sothe tooth is prepared to fit the most appropriatecrown.Yang JN, Mani G. Crowns for primary anterior teeth. International Journal of Pedodontic Rehabilitation, 2016; 1: 75-78.
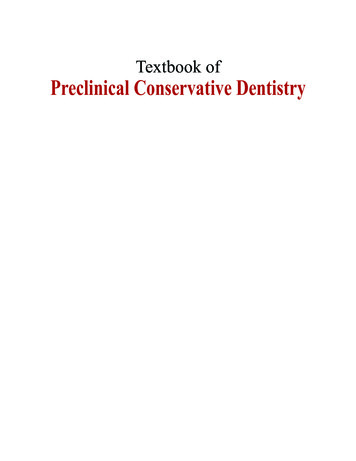
KINDER KROWNS Composite veneer facingbonded to fenestrated SSCbase. Two shades– Pedo 1 shade– Pedo 2 shade Better mechanical retentionbecause it is designed withincisal lock. Because itincreases surface area whichturn increases bondingKinder Krown ‘Incisal Lock’
PEDO PEARLSHeavy gauge aluminum crowns coated with FDA food gradepowder coating and epoxy-resin.ADVANTAGES:DISADVANTAGES: Less durability and crownsare relatively soft Universal anatomy-use oneither side Easy to cut and crimp, Self-cured or dual-curedwithout chipping or peeling.composite for repairing Non bulky & fits easily
PEDO JACKET CROWN It is a tooth colored copolyester materialwhich is filled with resin and left on tooth afterpolymerization instead of being removed.
PEDIATRIC ZIRCONIA CROWNS Zirconia is a crystalline dioxide of zirconium Kinder zirconiaEZ pedoNusmile zirconiaCheng zirconiaCrownsez crownsZirkiz crowns
KINDER ZIRCONIA CROWNS Available in natural shades and contour Great depth colour forms the lifelikeappearance.
AdvantagesAnterior crowns Posterior crownsAutoclavableLeft and rightLeft and rightPrecisely manufactured Shade pedo 1 and pedo Shade- pedo 1 and pedo 2.to ensure proper fit2Pedo 1- lighter bleachedshade.Pedo 2- darkerRough external surfacefor easy handlingLength- regular &short2 sizes- small and largeProvides betterretentionKhatri A. Esthetic zirconia crown in pedodontics. International Journal of Pedodontic Rehabilitation, 2017; 2: 31-33.
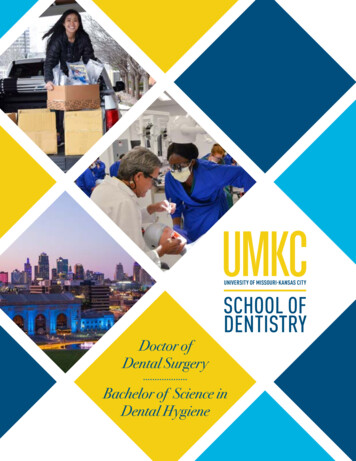
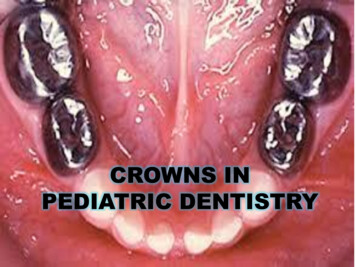
NUSMILE ZIRCONIA It is made up of high grade monolith Zirconiaceramic. It has increased durability with strength more thanenamel. Provides excellent esthetics Prevent the visibility of dark tooth discolouration ofpulpally treated teeth
BEFOREAFTERAshima G, Bhatia SK, Gauba K, Mittal HC. Zirconia Crowns for Rehabilitation of Decayed Primary Incisors: AnEsthetic Alternative. The Journal of Clinical Pediatric Dentistry, 2014; 39(1): 18-23.
CONCLUSION Operator preferences, esthetic demands by parents, the child’sbehavior, and moisture and hemorrhage control are all variableswhich affect the decision and ultimate outcome of whateverrestorative treatment is chosen. Crowns remain the best restoration in many cases, and estheticcrowns will have a larger role in pediatric dentistry ifimprovements are made to reduce the bulk, increase theretention and reduce the cost.
REFERENCES Dean JA. Dentistry for the Child and Adolescent, McDonald and Avery’s, 1st SouthAsia ed.Elsevier;2016. Casamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy throughAdolescence, 5th ed.Elsevier;2013. Tandon S. Textbook of Pedodontics, Vol 1, 3rd ed. Paras Medical Publishers, DharyaGanj, New Delhi, 2018. Marwah N. Textbook of Pediatric Dentistry,3rd ed. Jaypee;2014. Garg V, Panda A, Shah J, Panchal P. Crowns in pediatric dentistry. Journal ofAdvanced Medical and Dental Sciences Research, 2016; 4(2): 41-26. Ashima G, Bhatia SK, Gauba K, Mittal HC. Zirconia Crowns for Rehabilitation ofDecayed Primary Incisors: An Esthetic Alternative. The Journal of Clinical PediatricDentistry, 2014; 39(1): 18-23. Yang JN, Mani G. Crowns for primary anterior teeth. International Journal ofPedodontic Rehabilitation, 2016; 1: 75-78.
Casamassimo, Fields, Mctigue, Nowak. Pediatric Dentistry Infancy through Adolescence, 5th ed.Elsevier;2013. FINISHING- All line angles must be rounded Occlusobuccal & occlusolingual line angles are rounded by holding the bur at a 30-45o angle to the occl