Transcription
chapter 1Controlling drug deliveryOverviewIn this chapter we will:differentiate drug delivery systems according to their physical state& differentiate drug delivery systems according to their route of administration& differentiate drug delivery systems according to their type of drug release& discuss drug transport across epithelial barriers.&KeyPointsIntroductionPharmacotherapy can be defined as the treatmentand prevention of illness and disease by means ofdrugs of chemical or biological origin. It ranksamong the most important methods of medicaltreatment, together with surgery, physicaltreatment, radiation and psychotherapy. Thereare many success stories concerning the use ofdrugs and vaccines in the treatment, preventionand in some cases even eradication of diseases(e.g. smallpox, which is currently the onlyhuman infectious disease completelyeradicated). Although it is almost impossible toestimate the exact extent of the impact ofpharmacotherapy on human health, there can beno doubt that pharmacotherapy, together withimproved sanitation, better diet and betterhousing, has improved people’s health, lifeexpectancy and quality of life.Unprecedented developments in genomicsand molecular biology today offer a plethora ofnew drug targets. The use of modern chemicalsynthetic methods (such as combinatorialchemistry) enables the syntheses of a largenumber of new drug candidates in shorter timesthan ever before. At the same time, a betterunderstanding of the immune system and rapidprogress in molecular biology, cell biology andmicrobiology allow the development of modernvaccines against old and new challenges.&&Continued developments inchemistry, molecular biologyand genomics support thediscovery and developmentsof new drugs and new drugtargets.The drug delivery systememployed can control thepharmacological action of adrug, influencing itspharmacokinetic andsubsequent therapeuticprofile.TipCombinatorial chemistry is a way tobuild a variety of structurally relateddrug compounds rapidly andsystematically. These are assembledfrom a range of molecular entitieswhich are put together in differentcombinations. A ‘library’ ofcompounds of tens of thousands ofdifferent molecules is then screenedto identify compounds that bind totherapeutic targets.Sample chapter from Pharmaceutics: Drug Delivery and Targeting1
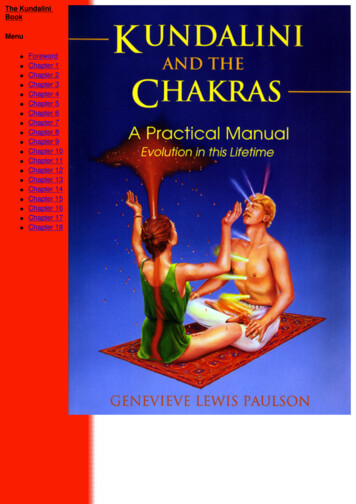
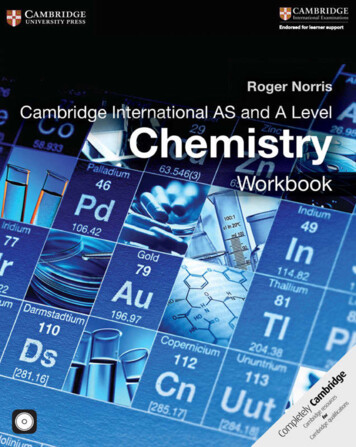
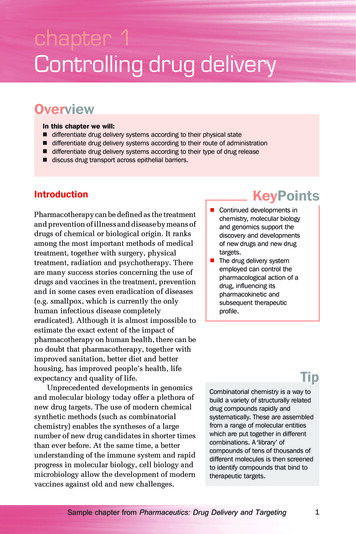
2Pharmaceutics: Drug Delivery and TargetingHowever, for all these exciting new drug and vaccine candidates, itis necessary to develop suitable dosage forms or drug deliverysystems to allow the effective, safe and reliable application of thesebioactive compounds to the patient. It is important to realise that theactive ingredient (regardless of whether this is a small-molecularweight ‘classical’ drug or a modern ‘biopharmaceutical’ drug like atherapeutic peptide, protein or antigen) is just one part of themedicine administered to the patient and it is the formulation of thedrug into a dosage form or drug delivery system that translatesdrug discovery and pharmacological research into clinical practice.Indeed the drug delivery system employedplays a vital role in controlling theUsually the drug concentration in thepharmacological effect of the drug as it canbody is determined in the plasma. Thisinfluence the pharmacokinetic profile of theis done as the plasma is comparativelydrug, the rate of drug release, the site andeasy to access and drugduration of drug action and subsequently theconcentrations can be reliablyside-effect profile. An optimal drug deliverymeasured using techniques such assystem ensures that the active drug is available athigh-performance liquidchromatography (HPLC). However,the site of action for the correct time and duration.the desired site of action for most drugsThe drug concentration at the appropriate siteis not the plasma and in principle itshould be above the minimal effectivewould be better to determine the drugconcentration (MEC) and below the minimalconcentration at the site of action oftoxic concentration (MTC). This concentrationthe drug.interval is known as the therapeutic range and theconcept is illustrated in Figure 1.1, showing thedrug plasma levels after oral administration of a drug from an immediaterelease dosage form.Achieving the desired concentration of a drug is dependent on thefrequency of dosing, the drug clearance rates, the route of administrationTipMTCPlasma concentrationFigure 1.1 Drug plasmalevels after oraladministration of a drug froman immediate-releasedosage from. Thetherapeutic range is theconcentration intervalbetween the minimaleffective concentration(MEC) and the minimal toxicconcentration (MTC). Dt isthe time interval the drug is inthe therapeutic range.MECΔtTimeSample chapter from Pharmaceutics: Drug Delivery and Targeting
Controlling drug delivery3and the drug delivery system employed. Within this book the terms drugdelivery system, dosage form and medicine are used interchangeably.However the term dosage form is often used to refer to the physicalappearance of the medicine whereas the term delivery system is oftenused to refer to the way the medicine releases the drug and delivers it tothe body or more specifically to the target organ, tissue, cell or evencellular organelle.Differentiating delivery systemsaccording to their physical stateFor dosage forms it is common to differentiatethe various types by classifying them accordingto their physical state into gaseous (e.g.anaesthetics), liquid (e.g. solutions, emulsions,suspensions), semisolid (e.g. creams, ointments,gels and pastes) and solid dosage forms(e.g. powders, granules, tablets and capsules).Most dosage forms contain several phases.Sometimes the phases of a dosage form are ofthe same state, for example for an emulsionwhich contains two liquid phases (oil and water).Whilst both phases are liquid, they differ in theirphysical properties, for example density andelectrical conductivity, and are separated fromeach other by an interface. However, more oftenthe dosage form contains phases of differentstates. For example, a suspension contains aliquid and a solid phase. Therefore classificationinto gaseous, liquid, semisolid or solid dosageforms may sometimes appear somewhatarbitrary. Finally, in these multiphase dosageforms usually one or more phases are dispersed,whilst other phases are continuous. In asuspension the solid phase is dispersed and theliquid phase is continuous, and in an oil-inwater emulsion the oil phase is dispersed and thewater phase is continuous. In some dosage formsthe determination of the type and number ofphases is not as straightforward. For example, thephases of creams can be difficult to determine,with the presence of a dispersed water (or oil)phase in addition to several continuous phases(oil, water and surfactant phases). For liposomaldispersions, the state of the phospholipidsKeyPoints&&&&Dosage forms can beclassified according to theirphysical state.Most dosage forms containseveral phases.Systems containing adispersed phase will give rise tophysical instability issues.All systems move to a state ofminimum free energy.TipA phase is a volume element of asystem (here the dosage form),separated from other volumeelements of the system by a phaseboundary (interface to anotherphase). The physical properties withinthe phase do not vary, which meansthat the phase is physicallyhomogeneous. From the requirementof homogeneity within a phase itfollows that the number of moleculeswithin the phase is large compared tothe number of molecules formingthe interface between the phases andsurrounding other phases.TipTo understand dosage forms from aphysical perspective, try to identify thenumber of phases in a dosage form,their state and if they are dispersed orcontinuous.Sample chapter from Pharmaceutics: Drug Delivery and Targeting
4Pharmaceutics: Drug Delivery and TargetingTipsHere are some examples of howdosage forms in their simplest termscan be differentiated according to thestate and dispersion of their phases:& A drug solution is a one-phasesystem as the dissolved drug doesnot fulfil the requirements for aphase. In a solution themolecularly dispersed drug will notseparate out to form largerparticles if the concentration of thedrug is not changed (e.g. byevaporation of the solvent) and theenvironmental conditions(e.g. temperature) are constant.& A suspension is a two-phasesystem containing a continuousliquid phase and a dispersed solidphase.& An emulsion is a two-phase systemcontaining two liquid phases, onedispersed and one continuous.& Ointments are generally two-phaseor multiphase gels, with at leasttwo continuous phases (usually acrystalline or liquid crystallinesurfactant phase and a lipidphase).& Creams additionally contain awater phase which may bedispersed (water-in-oil cream) orcontinuous (oil-in-water cream).& Tablets are essentially compressedpowers, and might thus beclassified as containing a solid andgaseous continuous phase. Ofcourse a tablet contains severalsolid phases, as drug particles areusually present together with othersolid phases (e.g. filler, binder,disintegrant, glidant and lubricantparticles).used to form the liposomes will determine if aliposomal dispersion is a suspension (if thelipids are in a crystalline state) or an emulsion(if the lipids are in a fluid, liquid crystallinestate).It is important to note that the presence of adispersed phase will lead to physical instabilityin the system. For example, in an oil-in-wateremulsion, the dispersed oil droplets have a largerinterfacial area to the water than if the dropletshad coalesced into one large continuous phase.This increased interfacial area leads to anincreased interfacial free energy, according to therelationship:G i ¼ Agwhere Gi is the interfacial free energy of thesystem, A is the interfacial area between thedispersed phase (here the oil droplets) and thecontinuous phase (here the water phase) and g isthe interfacial tension between the two phases.The interfacial free energy of the system (here theemulsion) can be minimised by coalescence ofthe droplets into larger droplets and finally intoone continuous oil phase, as this maximallyreduces the total interfacial area. This is of courseundesirable from a formulation viewpoint.Coalescence of droplets in an emulsion is apharmaceutical instability, but from athermodynamic viewpoint the system has beenstabilised, as the interfacial free energy has beenreduced. In practical terms an emulsion ispharmaceutically stabilised by addingemulsifiers to the systems, that either lower theinterfacial tension (note: if g gets smaller, Gi willget smaller), or that act as a physical barrieragainst coalescence. In either case, increasing theinterfacial area will still increase the surface freeenergy.Differentiating delivery systems accordingto their route of administrationAnother way of differentiating dosage forms is according to their site orroute of administration. Drugs can be administered directly into theSample chapter from Pharmaceutics: Drug Delivery and Targeting
Controlling drug deliverybody, though injection or infusion. This formof drug administration is termed parenteraldrug delivery. Depending on the site ofadministration into the body one candifferentiate between intravenous,intramuscular, subcutaneous, intradermal andintraperitoneal administration. Usuallyaqueous solutions are used for intravenousdelivery, but it is also possible that thedosage form contains a dispersed phase(solid or liquid), provided the dispersedparticles are small enough (e.g. smaller than100–150 nm) to avoid embolism. For otherroutes of parenteral administration thedelivery systems can be aqueous or oily oreven solid (the latter dosage forms are termedimplants).Drugs can also be administered on to theskin to enter into the body. Mostly semisoliddosage forms are used for this, includingcreams, ointments, gels and pastes. However,liquid dosage forms, such as emulsions, orsolid dosage forms, such as transdermalcontrolled drug delivery systems (patches),can also be used. These will be discussedin more depth in Chapter 6. It has to be takeninto account, though, that one of the mainfunctions of the skin as an organ is toprevent particles or compounds entering thebody, rather than allowing them to beabsorbed into the body. The stratum corneumof the skin forms a formidable barrier againstuptake and thus transdermal delivery isdifficult to achieve. Penetration enhancersoften have to be added to the deliverysystem to improve delivery into or through theskin. In transdermal controlled drugdelivery systems ideally the dosage formcontrols the uptake into the skin (ratherthan the uptake being controlled by thestratum corneum).The most important route of drugadministration into the body is throughmucosal membranes. Mucosal membranes aremuch less of a barrier to uptake than the skinand some mucosal membranes (such as theones in the small intestine) are indeed5KeyPoints&–––&The various routes ofadministration of a drug intothe body can be generallyclassified into:direct entry into the bodyentry into the body byovercoming the skinentry into the body by overcomingmucosal membranes.The oral route is often the mostconvenient route for drugdelivery; however, drugsdelivered via this route can bemetabolised by the hepaticfirst-pass effect.TipsParenteral drug deliverySubcutaneous injectionThe needle is inserted into the fattytissue just under the skin. Volumesshould be less than 2.5 ml perinjection site. Insulin is commonlyadministered via this route.Intramuscular injectionInjection into the muscle is preferredto the subcutaneous route if largervolumes (typically up to 5 ml inappropriate sites) have to be given.Intravenous injectionA needle is inserted directly into avein. This is the easiest way to give aprecise dose rapidly. Small volumescan be given as a single dose whereaslarger volumes can be given byinfusion.Intradermal injectionInjection is given into the skin. Thisform of parenteral administration isused in allergy skin testing.Intraperitoneal injectionInjection through the peritoneum (thethin, transparent membrane that linesthe walls of the abdomen).Sample chapter from Pharmaceutics: Drug Delivery and Targeting
6Pharmaceutics: Drug Delivery and Targetingspecialised sites for absorption. There aremany mucosal membranes that can be used forThe US Food and Drug Administrationdrug administration. Of the highest importance(FDA) has compiled an extensive list ofare the mucosal membranes of thedifferent dosage forms and differentgastrointestinal tract, allowing oral drugroutes of administration. These listsdelivery. The suitability and convenience ofcan be found on the FDA Center forthis route of delivery make oral dosage formsDrug Research websites:& http://www.fda.gov/cder/dsm/the most common of all drug delivery systems.DRG/drg00201.htmAlso the buccal, sublingual, rectal and vaginal& http://www.fda.gov/cder/dsm/mucosa and indeed the lung and nasal mucosalDRG/drg00301.htmmembranes can act as absorption sites. Forall of these mucosal membranes dosageforms have been developed, such as buccaland sublingual tablets, suppositories, vaginal rings, inhalers and nasalsprays, to name a few.If drug delivery systems are designed to give a local drug effect andnot systemic activity, they can be described as topical deliverysystems. This is the case for many dermal dosage forms.TipsOral drug deliveryAs stated above, the oral route is the most popular route to administerdrugs. However, some factors should be considered when looking toadminister drugs via this route. In particular the transit time in thegastrointestinal tract may vary considerably:&between patients and within the same patient, with the gastricresidence time being the most variable&with the state of the dosage form (liquid dosage forms are emptiedout of the stomach faster than solid dosage forms)&with the fasted or fed state of the patient.The pH conditions in the gastrointestinal tract also vary considerably,from a low pH in the stomach (1.5–2 in the fasted state to around 5 inthe fed state) to a higher pH in the small and large intestine. The pH inthe small intestine varies from 4 to 7, with an average value ofapproximately 6.5. This may affect stability and will influence the degreeof ionisation of ionisable drugs which in turn will influence theirabsorption (unionised forms of drugs are usually taken up better thanionised forms of the same drug) and solubility (unionised forms areusually less soluble than ionised forms of the same drug).First-pass metabolismImportantly, drugs that are taken up into the body through thegastrointestinal mucosa will be transported to the liver via the portalvein before going into general circulation. As the liver is the mainmetabolic organ of the body, if the drug is susceptible to metabolicdegradation in the liver, this may considerably reduce the activity ofSample chapter from Pharmaceutics: Drug Delivery and Targeting
Controlling drug deliverythe drug. This phenomenon is known as thehepatic first-pass effect. The rectal route mayalso show varying degrees of the first-passeffect, while for other routes of administration(intravenous, vaginal, nasal, buccal andsublingual) the drug is distributed in the bodybefore reaching the liver, and therefore forcertain drugs these may be the preferred routeof administration. However, whilst the liver isthe main metabolic organ of the body,metabolism may also take place in thegastrointestinal lumen and indeed in themucosal membranes.Differentiating drug delivery systemsaccording to their mechanismof drug releaseAnother systematic that can be used todifferentiate drug delivery systems is accordingto the way the drug is released. Broadly, one candifferentiate as follows:&Immediate release – drug is releasedimmediately after administration.&Modified release – drug release onlyoccurs some time after the administrationor for a prolonged period of time or to aspecific target in the body. Modifiedrelease systems can be furtherclassified as:–Delayed release: drug is released only atsome point after the initial administration.–Extended release: prolongs the release toreduce dosing frequency.These terms are also used by thepharmacopoeias and the FDA. Whilstimmediate-release dosage forms aredesigned to give a fast onset of drug action,modifications in drug release are oftendesirable to increase the stability, safetyand efficacy of the drug, to improve thetherapeutic outcome of the drugtreatment and/or to increase patientcompliance and convenience ofadministration.7TipAfter oral administration first-passmetabolism may occur in the liver andthe gut. For example, glyceryl trinitrateis predominantly metabolised in theliver and is therefore often formulatedfor sublingual delivery. In contrast,benzylpenicillin and insulin areprimarily metabolised in the gutlumen while orlistat is metabolisedwithin the gastrointestinal mucosalmembrane.KeyPoints&&&&&Dosage forms can control therate of release of a drug and/orthe location of release.They can be classified intoimmediate-release andmodified-release dosageforms.The modified-release systemscan be further divided intodelayed-, extended- andtargeted-release systems.Extended-release systemscan be further divided intosustained- and controlledrelease systems.Modifications in drug releaseprofiles can be used toimprove the stability, safety,efficacy and therapeuticprofile of a drug.TipsThe various forms of release asdefined by the FDAImmediate releaseAllows the drug to dissolve in thegastrointestinal contents, with nointention of delaying or prolongingthe dissolution or absorption ofthe drug.Sample chapter from Pharmaceutics: Drug Delivery and Targeting
8Pharmaceutics: Drug Delivery and TargetingModified releaseDosage forms whose drug releasecharacteristics of time course and/orlocation are chosen to accomplishtherapeutic or convenience objectivesnot offered by conventional dosageforms such as a solution or animmediate-release dosage form.Modified-release solid oral dosageforms include both delayed- andextended-release drug products.Delayed releaseRelease of a drug (or drugs) at a timeother than immediately following oraladministration.Extended releaseExtended-release products areformulated to make the drug availableover an extended period afteringestion. This allows a reduction indosing frequency compared to a drugpresented as a conventional dosageform (e.g. as a solution or animmediate-release dosage form).No definition for controlled releaseor targeted release is provided by theFDA or pharmacopoeias.KeyPoints&&&&Immediate-release deliverysystems give a fast onset ofaction.For a therapeutic action thedrug should be in solution,therefore disintegration of thedosage form and dissolution ofthe drug may have to occurfirst depending on the dosageform.Immediate-release systemsusually release the drug in asingle action following a firstorder kinetics profile.The time of action of the drug islimited to the time that theconcentration of the drug isabove the MEC.Immediate releaseMany dosage forms are designed to release thedrug immediately or at least as quickly aspossible after administration. This is useful if afast onset of action is required for therapeuticreasons. For example, a tablet containing apainkiller should disintegrate quickly in thegastrointestinal tract to allow a fast uptake intothe body.The onset of action is very fast for intravenousinjections and infusions and thepharmacological effect may be seen in a matter ofseconds after administration. The reasons for thisare twofold:1. The drug is already in solution, so strictlyspeaking the drug does not have to bereleased from the dosage form at all.2. The drug is directly administered into thebody, so no time is lost due to drugpermeation through the skin or mucosalmembranes, before the target organs can bereached.In oral solutions the drug is also already releasedand the solution will simply mix with thegastrointestinal fluids. However, powders andgranules need to dissolve first before the drug isreleased by dissolution. For tablets it is initiallynecessary that the tablet disintegrates (if it isformed from compressed granules this willinitially happen to the level of the granules, fromwhich further disintegration into powder particlesand finally drug dissolution occurs). For capsulesto release their drug content it is necessary forthe capsule shell material (for example, gelatin orhydroxypropylmethylcellulose (HPMC)) first todisintegrate. Thereafter the drug can eitherdissolve from the usually solid powders orgranules in the case of hard gelatin or HPMCcapsules or it can be dispersed from the usuallyliquid, lipophilic content of a soft gelatin capsule.These types of immediate-release dosage formshave an onset of action in the order of minutes tohours.Immediate-release dosage forms usuallyrelease (dissolve or disperse) the drug in a singleSample chapter from Pharmaceutics: Drug Delivery and Targeting
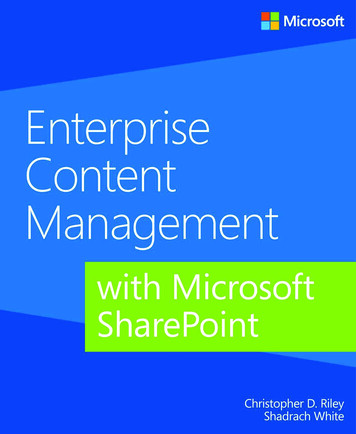
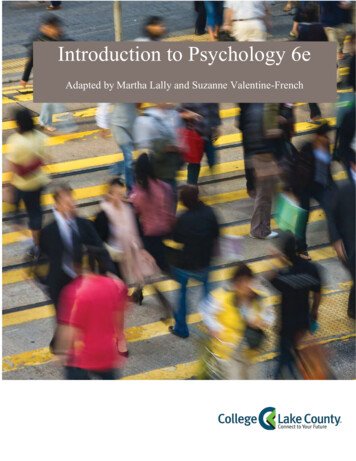
Controlling drug deliveryPlasma concentrationaction following a first-order kinetics profile.This means the drug is released initially veryquickly and then passes through the mucosalmembrane into the body, reaching the highestplasma level (termed Cmax) in a comparativelyshort time (termed tmax). Uptake through themucosal membranes may be due to passivediffusion or by receptor-mediated activetransport mechanisms (see section on modifiedrelease). Once taken up into the body the drug isdistributed throughout the body and eliminationof the drug by metabolism and excretion occurs.The elimination process also usually followsfirst-order kinetics. Therefore the plasma levelsmeasured over time after administration of animmediate-release dosage form (the plasmaconcentration time curve) basically are the sumof a first-order absorption and a first-orderelimination process. The resulting function isknown as the Bateman function. Figure 1.2shows an idealised plasma concentration versustime profile of an immediate-release oral dosageform.AUCtmaxTipsFirst-order kineticsThe rate of the process is proportionalto the concentration of one of thereactants, in our case the drug.Bateman functionThis function was initially used todescribe the concentration of aradioactive material B that stems froma first-order decay of anotherradioactive material A and that in itsown right further decays to anothermaterial C. If both decay processes(A ! B and B ! C) followfirst-order kinetics, exactly the samefunction results as for the plasmaconcentration time curve of a drugfrom an immediate-release oraldosage form. The A ! B decay isequivalent to the absorption processand the B ! C process is equivalentto the elimination process.Figure 1.2 Idealised plasmaconcentration versus timeprofile of an immediaterelease oral dosage form. Thehighest drug plasmaconcentration is termed Cmax.The time at which Cmax isreached is termed tmax. Thearea under the plasmaconcentration versus timeprofile is termed AUC andreflects the total amount ofdrug absorbed.Cmax9TimeAn important consideration for immediate-release dosage forms isthat the time of action of the drug is limited to the time that theconcentration of the drug is above the MEC. If the drug has a shortbiological half-life, this time interval may be short, requiring frequentSample chapter from Pharmaceutics: Drug Delivery and Targeting
10Pharmaceutics: Drug Delivery and Targetingdosing and potentially leading to low patient compliance and suboptimaltherapeutic outcome.The biological half-life of a drug is defined as the time required toreduce the plasma concentration by 50% by metabolism or excretion.Many studies show that a large proportion of patients do not take drugs asdirected (for example three times a day), especially if the disease is (atleast initially) not accompanied by strong symptoms, for example in thetreatment of high blood pressure or glaucoma. To reduce the frequency ofdrug administration it is often not possible simply to increase the dose ofan immediate-release dosage form as the peak plasma concentrations maybe too high and lead to unacceptable side-effects. Therefore the drugconcentration within the plasma should be above the MEC and below theMTC, i.e. within the therapeutic range (Figure 1.1).KeyPoints&&&&Modified-release systems aredesigned to influence therelease profile of a drug fromits delivery system.Oral delayed-release systemscan delay release until specificregions of the gastrointestinaltract are reached.Extended release of a drug canbe achieved using sustainedor controlled-release drugdelivery systems.Controlled-release systemsaim to control the plasmaconcentration of the drug afteradministration by variouspossible routes.TipImmediate-release oral deliverysystems can also have polymercoatings. In this case the polymer maybe used to mask an unpleasant tasteor odour, to facilitate swallowing of thedrug or to improve identification of themedicine. These coats dissolvequickly in the stomach and do notdelay the release of the drug.Modified releaseDosage forms can be designed to modify therelease of the drug over a given time or after thedosage form reaches the required location.Delayed releaseDelayed-release dosage forms can be defined assystems which are formulated to release theactive ingredient at a time other thanimmediately after administration. Delayedrelease from oral dosage forms can control wherethe drug is released, e.g. when the dosage formreaches the small intestine (enteric-coateddosage forms) or the colon (colon-specific dosageforms).Delayed-release systems can be used toprotect the drug from degradation in the low pHenvironment of the stomach or to protect thestomach from irritation by the drug. In thesecases drug release should be delayed until thedosage form has reached the small intestine.Often polymers are used to achieve this aim. Thedosage form (for example, a tablet or the granulesbefore tableting) can be coated with a suitablepolymer. The polymer dissolves as a function ofpH, so when the dosage forms travel from thelow-pH environment of the stomach to thehigher-pH environment of the small intestine,the polymer coat dissolves and the drug can bereleased. Once this occurs, the release is againimmediate and the resulting plasmaSample chapter from Pharmaceutics: Drug Delivery and Targeting
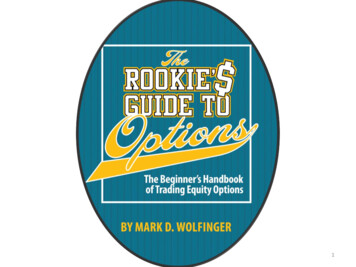
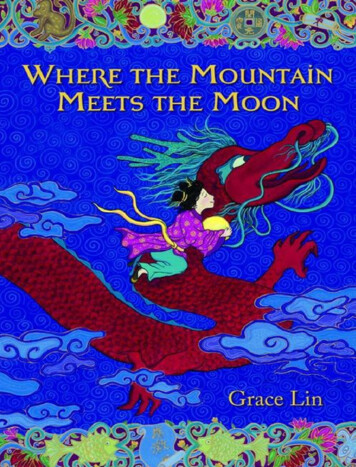
Controlling drug deliveryconcentration versus time curve is similar to the one for immediaterelease dosage forms.The development of colon-specific drugs and dosage forms may beadvantageous for the treatment of local and systemic diseases,including colorectal cancer and Crohn’s disease. Especially for peptideand protein drugs, this form of release may also be advantageous forsystemic administration given the more favourable pH conditions in thecolon compared to the stomach and the generally lower enzymaticactivity compared to the small intestine.Figure 1.3 shows an idealised plasma concentration versus timeprofile of a delayed-release oral dosage form. Tmax (but not Cmax) isstrongly dependent on the gastric emptying times which, as stated above,may be quite variable.Plasma concentrationFigure 1.3 Idealised plasma concentration versus time profile of a delayed-release oral dosageform compared to an immediate-release dosage form. TmaxIR is the time for maximum plasmaconcentration of the drug released from an immediate-release dosage form and TmaxDR is the timefor maximum plasma concentration of the drug released from a delayed-release dosage maxDRExtended releaseExtended-release systems allow for the drug to be released over prolongedtime periods. By extending the release profile of a drug, the frequency ofdosing can be reduced. For immediate-release dosage forms the timeinterval the plasma concentration is in the therapeutic range of the drugcan be quite short. Therefore frequent dosing, with its associatedcompliance problems, is required. This is especially an issue in chronicdiseases when patient
continuous. Controlling drug delivery 3 Sample chapter from Pharmaceutics: Drug Delivery and Targeting. used to form the liposomes will determine if a liposomal dispersion is a suspension (if the lipids are in a crystalline state) or an