Transcription
Using Trauma-Informed Practices to Enhance Safetyand Security in Women’s Correctional FacilitiesAlyssa Benedict, CORE AssociatesIntroductionOne of the most common experiences sharedby women in correctional facilities is a history oftrauma, which for many can be extensive.1 Researchfrom multiple disciplines has shown that the effectsof trauma can be significant and long lasting. Wenow know that trauma often plays a role in theonset of women’s criminal behavior, is often linkedto substance abuse and mental health challenges,and that trauma may explain some of the behaviorswomen offenders display while incarcerated(e.g. rule violations, violent episodes, “failure” intreatment, “manipulation”).Taking Universal PrecautionsExperts recommend that all systems (e.g., medical,mental health, corrections) be trauma-informed andthat professionals in these systems adopt “universalprecautions” when working with individuals. Universalprecautions means that we assume a trauma history ispresent with all individuals we interact with (and thatwe interact with them in a trauma-informed manner).In the wake of significant research on trauma andthe interventions required to address it, a number ofcorrectional agencies have made efforts to increasethe use of trauma-based services and curricula(e.g., psycho-educational groups). However, fewerefforts have focused on implementing “universalWhat is Traumaand What Causes It?“Trauma is trauma, no matterwhat caused it.” - Peter LevineTrauma has multiple causes. In addition tointerpersonal violence, trauma can resultfrom emotional neglect, sexual or physicalassault, accidents, war, illness, medicalintervention, the death of loved ones,natural disasters, and many other types ofevents.Trauma is created when an individualis exposed directly or indirectly to anoverwhelming event/experience thatinvolves a threat to one’s physical, emotionaland/or psychological safety. Overwhelmingevents can be physical or psychological.The experience of trauma may be suddenor dramatic, or the result of gradual andunrelenting violations. Sometimes, anindividual is not even aware that she hasbeen experiencing trauma until weeks,months, or even years have passed(Emerson & Hopper, 2011).precautions”2 or building a more integrated, multimodal trauma-informed culture in correctionalfacilities to both meet the goals of corrections andmaximize the success of trauma-based interventions.The literature on trauma offers correctionsprofessionals with common definitions, guidingThis project was supported by Grant No. 2010-DJ-BX-K080 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance is acomponent of the Office of Justice Programs, which also includes the Bureau of Justice Statistics, the National Institute of Justice, the Office ofJuvenile Justice and Delinquency Prevention, the SMART Office, and the Office for Victims of Crime. Points of view of opinions in this documentare those of the author and do not necessarily represent the official position or policies of the U.S. Department of Justice.1
principles, and examples of trauma-informedpractices that can be adopted and tailored for usein their facilities. This document provides a briefoverview of trauma and its effects on womenoffenders, and specifically defines trauma-informedpractices for women’s correctional facilities.3 It alsoprovides key actions that facility administrators,managers, and staff can take to better align theiroperational practices with the research on traumaand to create a more trauma-informed facilityculture.system is activated, allowing us to “rest and digest.”While the human body is designed to handle manystressful events, traumatic events like childhoodneglect and sexual assault can overwhelm thehuman stress response. Trauma research, includingbrain scan data, shows that many survivors areeasily triggered into or chronically “stuck” in thebody’s stress response.What Do We Know About theExperience of Trauma AmongWomen Inmates ?First, there is an extremely high prevalence oftrauma among women inmates: justice-involvedwomen report extraordinarily high rates oftraumatic experiences that exceed the ratesreported by women in the general population—including childhood sexual abuse, sexual assault,and intimate partner violence.4 This fact remainstrue for women in institutions, with some studiesnoting rates of trauma histories among womeninmates as high as 90%.5Second, the research on trauma shows that theeffects of traumatic experiences continue wellafter the event(s). Trauma survivors experiencepsychological and physiological repercussions thatare rooted in the brain’s response to trauma. Infact, experts assert that trauma is, by definition,neurobiological.6 Typically, when we experiencea threat, the brain and body work together toeffectively respond. The brain cues the sympatheticnervous system, which stimulates a host ofphysiological and hormonal events that are designedto keep us safe (i.e., the flight response): our heartrate and blood pressure increase; we become morealert in our senses; our muscles become tense; ourdigestive system shuts down; blood is diverted tothe limbs and other areas of the body where it ismost needed in that moment. These physiologicalchanges are designed to keep us safe in the face ofa threat. Once the stressor or threat is no longerpresent, the body’s parasympathetic nervous2Because they are stuck in a state of extreme stressand self-protection, it is difficult for survivors to bepresent in the here and now.7 Due to their historiesof often multiple traumatic experiences, manywomen inmates are in a constant state of fight orflight—a self-protective mechanism that is hardwired in all human beings. This state, and all thephysiological changes that accompany it, becomesthe norm and it is perpetually activated. This cancause significant psychological and physiologicalstress; trauma survivors are constantly, and oftenunconsciously, scanning their environment for athreat or interpreting all events and interactions aspotentially unsafe and threatening. They have greatdifficulty regaining a sense of safety and regulation(i.e., relaxation).8 Returning to a state of equilibriumin body and mind is challenging for all traumasurvivors; for women living in correctional facilities,it can be extraordinarily difficult.
What Does This Mean for Women’sInstitutions?Given the prevalence of trauma among womeninmates and the realities of its effects, somewomen’s correctional facilities9 have begun to createa more trauma-informed culture. In a traumainformed culture:1. Staff understand trauma’s pervasive effects onthe brain and body,2. Innovative programs are introduced to educatewomen on the effects of trauma and help themcope with its effects, and3. Operational practices are specifically structuredto help women manage difficult symptoms sothey can safely engage in institutional programsand services.Becoming trauma-informedas an institution means changing those operational practices thatcan cause further trauma to women.Trauma survivors often carry sensations of constantthreat (e.g., dry throat, increased heart rate) andwill do anything to make these sensations go away.10Drug use, self-harm, defiance, and other negativebehaviors exhibited by women inmates may bebetter understood as trauma survival behaviorsthat alleviate deep sensory distress, rather than ablatant disregard for institutional rules. Commoncorrectional routines and practices can worsen oralleviate the sensory distress that accompaniestrauma. For women inmates, attempts toneutralize, escape, or protect can take many forms:bullying another inmate, forming inmate families,withdrawing from certain activities, nurturing withfood, and countless other behaviors. In the absenceof alternatives and living in a climate of fear, thesebehaviors offer a sense of control and providepsychological and physiological relief.3For institutions, becoming trauma-informed meansmodifying operational practices that can causefurther trauma to women inmates. For instance: The conduct of strip searches by staff forcontraband may re-traumatize women who havebeen sexually abused in the past.11 Transitioning inmates from one place toanother in a facility appears to be an innocuousprocedure; yet, for women inmates who aretrauma survivors, transitions can be significanttriggers. Being supervised by male staff during sensitivetimes (i.e., showering, dressing/undressing) notonly creates basic human discomfort, but can beextremely traumatic for women who have beenabused by men.Trauma survivors need to have physical and sensoryexperiences that help them to “unlock their bodies,activate effective fight/flight responses, tolerate theirsensations, befriend their inner experiences, and cultivatenew action patterns.”- Emerson & Hopper, 2011Various events and routines that occur day-to-dayin women’s facilities can easily be perceived asthreatening (e.g., banging of doors, loud voices,unfamiliar persons, having to talk with someonewho is unfamiliar, strip searches, cell extractions,segregation). These events and routines are oftenexperienced as “triggers” and make it very difficultfor the nervous system to reset itself; therefore,women in institutions often live day-to-day inan unnecessarily heightened state of stress. Forexample, a woman inmate who has survivedchildhood sexual abuse is likely to have developedfinely tuned neurophysiological patterns to helpkeep her safe by allowing her to respond to theperception of any cues that were present duringher abuse. If she experiences one or more ofthese cues, she will experience the same cascadeof neurochemicals that were triggered duringthe actual event.12 This reaction is automatic,often unconscious and governed by the brain’sfear-response system. Many women inmates areintensely on guard; their primary (instinctual) brain
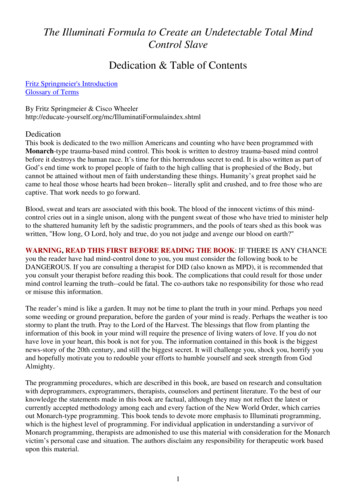
is constantly scanning for threat or opportunity;and they are frequently feeling and acting fromfear. Responding to the research on trauma andtaking specific steps toward becoming more traumainformed can help correctional professionalscreate safer and more secure facilities. Traumainformed environments facilitate psychological andphysiological regulation; inmates who feel safe intheir environment are less likely to be triggered intoself-protective responses that complicate facilityoperations.A trigger is an internal or externalexperience that is a reminder of one ormore traumatic events.When a trigger is present, an individual’smind and body respond as if the threat isactually present.What Are The Benefits of Creating aMore Trauma-Informed InstitutionalCulture?Research on the neurobiology of trauma has also ledto new understandings on the nature of recoveryand healing. Just as exposure to trauma affectsan individual’s neurobiological response system,trauma-informed interactions with others cancreate healing at the neurobiological level.13 Humanbeings literally regulate each other’s biologicalstates.14 In women’s facilities, how staff interactwith women inmates can either create morepsychological and physiological stability or causemore dysregulation and instability. Staff can literallyalleviate women inmates’ distress, increase theirability to meaningfully engage in services, and setthe stage for recovery from traumatic events just bychanging their interactions and operational practiceswith women. Facilities that have begun to take stepstoward creating a more trauma-informed culturereport: Improvements in inmates’ ability to fall and stayasleep at night4 Improved attendance and participation inprograms and services Decreases in disciplinary infractions Decreases in conflicts between inmatesFor example, under the leadership ofSuperintendent Lynn Bissonnette, theMassachusetts Correctional Institution atFramingham has begun to implement traumainformed strategies (such as training all staff ontrauma-informed approaches, implementing a peersupport program for the women, and opening anIntensive Treatment Unit for inmates on mentalhealth watch or crisis intervention) with promisingresults: Between 2011 and 2012, there was anotable decrease in inmate-on-staff and inmateon-inmate assaults, the use of segregation, suicideattempts, and the need for mental health watches(see chart on the following page).Creating A Trauma-informed Culturein Women’s Correctional InstitutionsPrinciples of Trauma-Informed PracticeThe broad principles of trauma-informed practiceoffered by Fallot and Harris15 have become thestandard and suggest that we offer justice-involvedwomen opportunities to experience safety, trust,choice, collaboration and empowerment. Althoughthese principles are frequently cited when definingtrauma-informed care, there has been lessdiscussion on how to implement them in facilitysettings. When these characteristics are presentin facilities, they are often confined to one-on-onecounseling, case management, or treatment groupprocesses. Broadening trauma-informed practices tothe larger institutional culture for women inmatesrequires that leadership and staff work togetherto put these principles into practice at the primaryinmate contact points as noted on page 6.While on the surface these principles may appearincompatible with the correctional practices that aredesigned to assure institutional safety and security,research and experience demonstrate that they are
Benefits of Implementing Trauma-Informed Approaches at MCI FraminghamFrequency of Incidents in 2011 and 201220112012FrequencyChange% ChangeInmate-on-staff assaults6525-40-62%Inmate-on-inmate assaults11251-61-54%Inmate-on-inmate fights12970-59-46%Segregation placements966748-218-23%Disciplinary reports58305470-360-6%Suicide attempts3012-18-60%One-on-one mental health watches14798-49-33%Petitions for psychiatric evaluation4437-7-16%Crisis contacts15361316-220-14%Self-injury incidents11499-15-13%TypeSource: Bissonnette, 2013.essential to addressing trauma effectively, and canactually help to enhance institutional safety andsecurity. Consider the following: Miller and Najavits16 point out that institutionalvalues such as running a highly structured andsafe environment, offering consistent limits,incentives, and boundaries, and administeringfair, swift, and certain consequences for5behaviors are the very features that provide “thetype of stability trauma survivors need to learnnew information and skills that promote traumarecovery.” Emerging data from MCI Framingham, the RhodeIsland Department of Corrections Women’sFacilities, and others suggest that implementingtrauma-informed practices in institutional
Trauma-informed Practice ntsettings can enhance efforts to achieve safety andsecurity (as measured by reductions in inmateinmate assaults, inmate-staff confrontations,disciplinary sanctions, and the use of force).17When basic correctional processes such as intakeand discipline do not reflect trauma-informedprinciples, they can be experienced as additionaltraumatic events by women inmates. This additionaltrauma can increase their already high level ofpsychological and physiological stress, and increasethe number and seriousness of coping and survivalbehaviors that complicate management andsupervision (e.g., arguing, fighting, self-harming,refusing staff direction). Importantly, traumainformed practice does not replace accountability;it is still important to hold women accountable fortheir behavior whenever necessary—the key is to doso while being trauma informed. What those whohave begun this work are finding, however, is thatactively creating a trauma-informed correctionalenvironment reduces unsafe inmate behaviors.When women inmates feel safe and secure intheir environment—and are given opportunitiesto exercise choices and work with staff towardpersonal goals—their behavior becomes morestable and their engagement in services improves.Opportunities for ImplementingTrauma-Informed Practices inCorrectional SettingsCorrections professionals can maintain safer andmore secure environments by integrating trauma-6Primary Inmate Contact PointsIntake/Admissions and ScreeningAssessment and ClassificationCase Planning and ManagementStaff-Inmate InteractionsSanctions and DisciplineProgramming and TreatmentMedical ServicesMental Health ServicesDischarge, Transition, and Reentryinformed principles throughout their institutions,helping inmates manage their trauma symptoms,and cultivating important skills for success withinand outside of facilities. Trauma-informed practicecannot be confined to clinical sessions or groups;all institutional staff have a role in creating apsychologically and physically safe institutionalenvironment. The table on the following pagesoffers specific examples of how several key contactpoints within a facility can be enhanced according tothe principles of trauma-informed practice.Eight Action Steps for Building ATrauma-Informed Facility CultureSome specific actions that correctional professionalscan take to become more trauma-informedare provided in the sections below. Action Step#1, “Make a Commitment to Trauma-InformedPractice,” provides an important foundation for theremaining steps. While the order in which ActionSteps are discussed suggests a possible sequence,they can be implemented in any order given aninstitution’s unique population profile, staffingpattern, fiscal and political realities, and otherimportant variables. Taken together, these steps canhelp build an integrated trauma-informed facilityculture.Creating a trauma-informed culture requires a multi-modalapproach where trauma-informed practice permeates alllevels of institutional practice.
Opportunities for Implementing Trauma-Informed Practicein Women’s FacilitiesContact PointTrauma-Informed Practices(Apply principles of safety, trust, choice, collaboration and empowerment)Intake/Admissions g andManagementStaff-InmateInteractions799 Let inmates choose where to sit in a defined, safe and secure intake/admission space99 Let inmates know what you will be asking, why and who will have access to theinformation99 Review the facility rules and expectations, emphasizing physical, emotional, and sexualsafety, and the policies that support all three99 Train intake staff to recognize and respond to trauma symptoms99 Train assessment and classification staff to use a trauma-informed approach whenconducting assessments and recognize trauma symptoms99 Let inmates know what you will be asking, why, and who will have access to theinformation99 Assess for past and recent trauma as well as current trauma symptoms/responses99 Utilize information about inmates’ past trauma in classification decisions99 Define case management goals with inmates; offer options and respect the choicesinmates make about goals and case management targets99 Work in a spirit of collaboration with the woman99 Ensure case management sessions have a clear agenda99 Actively define and discuss confidentiality with inmates, including its limitations99 Provide inmates with copies of their case plans and help her develop a plan for keepingthem safe from other inmates or staff99 Refer to the inmate’s strengths99 Utilize Motivational Interviewing skills99 Facilitate productive and safe interactions between inmates as part of unit meetings,recreation, and other activities99 Celebrate inmate strengths and accomplishments as part of routine interactions99 Use a tone of voice and pace of speaking that encourages stability and physiologicalregulation (i.e., relaxation)99 Use postures and body proximity that convey safety and support (versus control)99 Utilize Motivational Interviewing skills
Sanctions andDisciplineProgrammingand TreatmentMedicalServices899 Use trauma-informed de-escalation techniques (e.g., maintain an even and respectfultone, use inmates’ names, use short encouraging phrases)99 Where safety and security permits, introduce sensory boxes (boxes that contain comfortitems that can be used for de-escalation and relaxation such as squishy balls, mini beanbags, soft plastic balls)99 Use segregation and restraints as a last resort99 Talk about what happened with inmates after a restraint has occurred99 Develop group agreements with inmates for all group work, including expectationsaround emotional safety and confidentiality99 Define treatment options with inmates; do not force treatment of trauma or disclosureof trauma99 Assure that substance abuse programs recognize the impact of trauma on substancedependence99 Do not begin any type of trauma treatment while inmates are incarcerated if there is notsufficient time to work with issues that arise99 Maintain provider consistency so inmates can cultivate trust99 Ensure treatment plans define coping strategies inmates can develop to deal with thechallenges of life in and outside of the institution99 Implement programs that offer opportunities for inmates to connect with and bond withtheir children99 Screen low risk, low need inmates from interventions designed for high risk/high needinmates99 Ensure that inmates are aware of what medications they are on, why, potential sideeffects, etc.99 Encourage inmates to keep a journal where they can track their body’s response to themedications they are on and share observations, concerns, and ideas with providers99 Utilize same-sex practitioners where possible and offer chaperons during OB/GYYN visitswhen same sex practitioners cannot be provided99 Uphold privacy as part of all medical practices99 Ensure that all medical visits adopt a basic trauma-informed protocol (e.g., the goals ofthe visit are explained first, inmates are invited to ask questions or raise concerns beforebeginning and during any medical procedures, inmates have a voice in what procedurestake place and how they take place)99 Implement protocols that maximize early bonding opportunities between mothers andinfants99 Empower inmates with knowledge by offering classes and workshops on basic anatomyand physiology, the mind-body connection, etc.
Mental HealthServicesDischarge,Transition andReentry99 Complement utilization of psychotropic medications with interventions that give inmatesthe opportunity to develop brain-body regulation skills such as mindfulness-basedstress reduction (MBSR)18, yoga, biofeedback, and various somatically-based therapies/interventions99 Empower inmates with knowledge by offering classes and workshops on mental healthand wellness and that describe the links between trauma, substance abuse, and mentalhealth99 Adopt strength-based language (e.g., providers should talk with inmates about survivalbehaviors and patterns versus impaired function and maladaptive coping)99 Establish protocols that are designed to support inmates during times of grief and loss,including immediately following visits with loved ones, transitions, etc.99 Begin discharge planning as soon as possible after admission so that release does notbecome another traumatic event in inmates’ lives99 Address how inmates can deal with trauma symptoms upon release as part of thedischarge plan99 Facilitate inmate contact with individuals and organizations with whom she will beworking upon release99 Ensure that inmates have a written, specific, individualized Community Safety Plan(including the names and numbers of organizations they can call when needed); ideally,this plan is informed by the Personal Safety Plan that is initially developed at intake99 Conduct departure rituals that honor and encourage inmates as they move on to a newphase in their livesEverything we do and how we do it can be designedeither to literally cue safety and stability at thelevel of the nervous system or to create moredysregulation, disengagement and unsafe copingmechanisms that compromise institutional safetyand security. Institutional enhancement requires anintentional effort to translate research into practicein a way that is both practical and realistic.Action Step #1: Make a Commitmentto Trauma-Informed PracticeFirst, acknowledge that being trauma-informed isimportant. Consider the development of a PositionStatement on Trauma-Informed Practice. Engagestaff and inmates in the development of the PositionStatement:9 Conduct focus groups with staff and inmates togain their input (see sample questions in the textbox on the next page). Administer surveys to staff and inmates to gaintheir input. You need not start from scratch:there are some excellent surveys that can beused to gauge staff and inmate perspectives ontrauma-informed practice and their experienceswithin the facility.19 Solicit information about institutionalexperiences from staff, inmates, and providersindividually in informal settings (e.g., during staffmeetings, facility walk-throughs, during breaks). Assign a small work group to draft a PositionStatement based on the feedback received. Solicit further input (e.g., from an inmatecouncil, medical and mental health staff) where
necessary/desired and develop a final PositionStatement on Trauma-Informed Practice. Once developed, disseminate the PositionStatement throughout the facility and discusswith staff and inmates the steps they can take tomake the statement a reality as part of day-today practice.Questions to Ask Staff and Inmatesto Develop a Position Statementon Trauma-Informed Practice1.2.3.4.What operational practices make you feel safe?What operational practices make you feel unsafe?How would you describe the interactions betweenstaff and inmates?How would you describe the interactions betweeninmates and other inmates?Action Step #2: Support and Train Staffin their Efforts to be More TraumaInformedStaff are the backbone of any institution’s successfuloperation, yet many report feeling unpreparedfor the complexities of day-to-day work withwomen inmates and the various behaviors theyexhibit, including those that are linked to trauma.20Providing staff with the support and skills they needto do their jobs effectively is essential. Trainingand access to resources can help staff deal withthe inherent challenges associated with workingday-to-day with women inmates who are traumasurvivors.21 It is particularly critical to assist staff inbalancing their responsibilities to act in a traumainformed manner, while still holding womenaccountable for any negative behavior. Four types ofstaff support are particularly important to consider: Training: Staff training is one of the most widelycited actions that leadership can take to enhancefacility services and outcomes. Consider makingtraining on trauma-informed practices as wellas other skill-based training a core trainingrequirement for all staff.22 Training modules10Essential Training Elements on Trauma99 Explain the benefits of trauma-informedapproaches: reduced use of mental health units,reduced use of restraints, reduced numberof critical incidents, more effective behaviormanagement, increased job satisfaction, less staffburnout/turnover, etc.99 Present basic information on trauma: what traumais and how it affects the brain and body, traumarelated symptoms/behaviors, gender and culturallyspecific coping mechanisms, ways to facilitateinmate safety and stability.99 Demonstrate skills: show staff how to talk inmatesthrough pat downs and searches, and respond toinmates’ disclosures of trauma respectfully andeffectively.99 Include sufficient skill practice/rehearsal: userole plays, practice de-escalation techniques,practice how to identify and maintain professionalboundaries.99 Reinforce and build on strategies that staff haveused successfully in the past.Adapted from Miller & Najavits, 2012.focused on building concrete staff skills whenworking with women trauma survivors isespecially important. Coaching and Mentoring: Managers andsupervisors can play an important role insupporting and reinforcing staff in traumainformed practices on a daily basis. For example,are staff members given opportunities to practicenew skills and succeed? Are there opportunitiesfor managers and supervisors to observe staffinmate interactions and provide feedback,coaching, and mentoring? Professional and Personal Support: Facilityleadership can cultivate a trauma- freeenvironment for staff by maintaining regularcommunication, offering regular formalsupervisions, making expectations clear, andnot only communicating changes in institutionalpolicy and practice, but obtaining staff inputbeforehand. Staff members who feel safe and
supported are more likely to offer safetyand support to inmates. Conversely, staff cansupport managers by communicating strengthsand challenges, and making a commitment toinstitutional improvement. Attending to Secondary Trauma: Seeing intenseinmate behaviors and hearing traumatic storiescan take a toll on staff; secondary, or vicarioustrauma, is not uncommon for professionalsworking in a correctional environment. Forexample, when staff are repeatedly exposed tohorrific stories of trauma and/or the behaviorsthat inmates display as a result, they may feel theeffects of trauma as well. Employee AssistanceProtocols (EAPs) are intended to help employeesdeal with personal challenges that mightadversely impact their work performance, health,and well-being. EAPs generally include short-termcounseling and referral services for employeesand their families. Services can be added toEAPs that make staff more aware of the effectsof secondary trauma and offer coping skillsonsite or via referral. Importantly, supportingeach staff member’s ability to cope with thingslike secondary trauma and burnout should notoccur once there is a problem, but be offeredas an essential aspect of staff development.Onsite services (e.g., Mindfulness-based StressReduction (MBSR)23, relaxation skills training) andlinkages to local organizations let staff know thatself-care is important and that the institutionalleadership values staff and the hard work they doevery day.Action Step #3: Adopt
What Does This Mean for Women’s Institutions? Given the prevalence of trauma among women inmates and the realities of its effects, some women’s correctional facilit