Transcription
PEDIATRICS/ORIGINAL RESEARCHCool Running Water First Aid Decreases SkinGrafting Requirements in Pediatric Burns: ACohort Study of Two Thousand Four HundredNinety-five ChildrenBronwyn R. Griffin, Grad Dip Emerg Nursing, PhD*; Cody C. Frear, BA*; Franz Babl, MD; Ed Oakley, MBBS;Roy M. Kimble, DMed(res), MBChB*Corresponding Author. E-mail: bronwyn.griffin@qut.edu.au or cody.frear@uqconnect.edu.au, Twitter: @brongriffin or @CodyFrear.Study objective: First-aid guidelines recommend the administration of cool running water in the early management of thermalinjury. Our objective is to analyze the associations between first aid and skin-grafting requirements in children with burns.Methods: This cohort study used a prospectively collected registry of patients managed at a tertiary children’s hospital.Multivariate logistic regression models were used to evaluate the relationship between first aid and the requirement for skingrafting. Secondary outcomes included time to re-epithelialization, wound depth, hospital admission and length of stay, andoperating room interventions. Adequate first aid was defined as 20 minutes of cool running water within 3 hours of injury.Results: In our cohort of 2,495 children, 2,259 (90.6%) received first aid involving running water, but only 1,780 (71.3%) were giventhe adequate duration. A total of 236 children (9.5%) required grafting. The odds of grafting were decreased in the adequate firstaid group (odds ratio [OR] 0.6; 95% confidence interval [CI] 0.4 to 0.8). The provision of adequate running water was furtherassociated with reductions in full-thickness depth (OR 0.4; 95% CI 0.2 to 0.6), hospital admission (OR 0.7; 95% CI 0.3 to 0.9), andoperating room interventions (OR 0.7; 95% CI 0.5 to 0.9), but not hospital length of stay (hazard ratio¼0.9; 95% CI 0.7 to 1.2; P¼.48).Conclusion: Burn severity and clinical outcomes improved with the administration of cool running water. Adequate first aid mustbe prioritized by out-of-hospital and emergency medical services in the preliminary management of pediatric burns. [Ann EmergMed. 2020;75:75-85.]Please see page 76 for the Editor’s Capsule Summary of this article.Readers: click on the link to go directly to a survey in which you can provide feedback to Annals on this particular article.A podcast for this article is available at www.annemergmed.com.0196-0644/ -see front matterCopyright 2019 by the American College of Emergency 019.06.028INTRODUCTIONBackgroundCurrent first-aid guidelines in the United States,1United Kingdom,2 and Australia3 call for the irrigationof acute burns with cool running water. In contrastwith that for alternative treatments such as ice,4 aloe vera,5and toothpaste,6 a solid body of evidence has developedaround the favorable effects of water first aid. Early researchreported possible associations with decreased mortality,7infection, clinical appointments, pain,8 and scarring.9 Morerecently, a series of animal model studies observed thegreatest improvements in re-epithelialization, depth, andcosmetic outcomes with the application of cool runningwater for 20 minutes immediately postburn, althoughbenefits were still noted after a delay of up to 3 hours.4,10-12Volume 75, no. 1 : January 2020Despite this research, there is still debate surrounding theoptimal duration of first aid, with recommendationsranging from a full 20 minutes in Australia,3 the UnitedKingdom,2 and Europe13 to only approximately 5 minutesin the United States.1Relatively little research has explored the effect of coolrunning water on clinical outcomes in human populations,and the few existing studies lack consistency in theirfindings and definitions of appropriate first aid.14-17 By farthe most comprehensive human evidence to date wasprovided by a pair of recent Australian studies involvinglarge adult cohorts.18,19 Both identified several clinicalbenefits associated with the provision of cool running waterfirst aid, including decreased surgical requirements, time tore-epithelialization, burn depth, ICU admission, and lengthAnnals of Emergency Medicine 75
Cool Running Water First Aid for Pediatric BurnsEditor’s Capsule SummaryWhat is already known on this topicMany guidelines recommend irrigation with coolrunning water for 20 minutes’ duration after a burn.What question this study addressedIs there an association between 20 minutes of coolrunning water within 3 hours of injury and skingrafting requirements in children with burns?What this study adds to our knowledgeIn this cohort study, the odds of skin grafting weredecreased among children who had 20 minutes ofcold running water (odds ratio 0.6; 95% confidenceinterval 0.4 to 0.8).How this is relevant to clinical practiceAlthough this study establishes only association, inthe absence of better-evidence first-aid guidelines,physicians should promote 20 minutes of cool-waterirrigation for burns in children.of stay in the hospital. Together, they were the first studiesto convincingly demonstrate cool running water’seffectiveness as a first-aid intervention for adult burns.ImportanceAlthough children are at particularly high risk of burninjuries,20 there is a paucity of literature addressing therelationship between burn first aid and clinical outcomes inpediatric populations. Because of differences in volume,surface area,21 and skin thickness,22,23 it is unknownwhether benefits in adults apply to children.Goals of This InvestigationThe purpose of this study was to determine therelationship between cool running water first aid and burnwound healing in a large pediatric cohort. We tested thehypothesis that adequate first aid, 20 minutes of coolrunning water, would be associated with a decrease in theodds of grafting. We further examined its relationship withsecondary outcomes, including time to re-epithelialization,burn depth, hospital admission, hospital length of stay, andgeneral operating room requirements.MATERIALS AND METHODSStudy Design and SettingThis study was designed with a prospectively collecteddatabase that documents every pediatric burn patient (0 to76 Annals of Emergency MedicineGriffin et al16 years) attending the only dedicated children’s burncenter in the Australian state of Queensland. The databasecontains information on all inpatients and outpatientstreated at the center, capturing the entirety of their journeyof care until discharge from the service or referral to scarmanagement. Data from July 2013 to June 2016 wereextracted and analyzed.In line with recommendations by the European BurnsAssociation,13 British Burn Association,2 and Australianand New Zealand Burn Association,3 first aid wascharacterized as adequate if it involved greater than or equalto 20 minutes of cool running water delivered eithercumulatively or continuously within 3 hours of injury. Anyother form of first aid, including cool running water of lessthan 20 minutes’ duration or the use of alternatives (eg, stillwater, ice, aloe vera), was classified as inadequate. Friction,electrical, and chemical burns were excluded, along withcases in which the type or duration of first aid wasunknown.The study was approved by the Children’s HealthService District–Human Research Ethics Committee.Consent for inclusion in the database was obtained at datacollection. Patient information was deidentified whileundergoing statistical analysis, maintaining patient privacyand confidentiality.Selection of ParticipantsInvestigators conducted structured interviews with allfamilies who consented to data collection at their firstpresentation to the participating hospital’s burn outpatientdepartment or inpatient ward. Patients were referred to theburn service by the children’s hospital’s own emergencydepartment (ED), a local hospital ED, a generalpractitioner, or another source (eg, a pediatrician).Information collected during the structured interviewsincluded demographics and injury-related details such asmechanism of injury and first aid. All interventionsperformed in the first 3 hours postinjury were documented,encompassing treatment provided at the scene of the injury,in the care of paramedics, in the ED or other referral center,or all 3. Total first aid was divided into 6 categories: no firstaid; an alternative to cool running water; or durations ofcool running water lasting less than 5 minutes, 5 to 10minutes, 11 to 19 minutes, or greater than or equal to 20minutes.Because previous research demonstrated thatsocioeconomic disadvantage was associated with a reducedlikelihood of receiving first aid and poorer clinical outcomesamong children with burns,24,25 patient socioeconomicstatus was assessed to be included as a covariate in theVolume 75, no. 1 : January 2020
Griffin et alanalytic models. It was evaluated indirectly with postcodethrough the Socio-Economic Indexes for Areas developedby the Australian Bureau of Statistics.26 For the purposes ofthis research, socioeconomic status deciles were dividedinto 3 groups: disadvantaged (deciles 1 to 4), advantaged(deciles 5 to 8), and highly advantaged (deciles 9 and 10).Outcome MeasuresThe primary outcome of the study, skin grafting, servesas a strong indicator of burn severity, healing capacity, andpatient morbidity. Grafting is undertaken only whenclinicians conclude that a wound is incapable of healingspontaneously or without sufficient speed to preventsignificant scarring. Secondary outcomes included time tore-epithelialization among ungrafted burns, wound depth,hospital admission and length of stay, and requirements forany operating room interventions.Grafting procedures, operating room interventions,hospital admission, and hospital length of stay wererecorded through active tracking of patients and post hocreview of their medical charts. Time to re-epithelializationwas assessed by calculating the number of days between thedate of injury and the completion of acute treatment in theoutpatient department. Senior burns clinicians visuallyassessed and classified burn depth on initial review in theoutpatient department or inpatient ward according to theclassification system by Shakespeare.27 For burnscharacterized by a mixture of thicknesses, researchersrecorded the most severe depth. Total body surface areapercentage was estimated with the Lund and Browder28method, also on initial assessment.Primary Data AnalysisDescriptive statistics were carried out for all keyvariables, with 95% confidence intervals (CIs) reportedwhere relevant. Median and interquartile range werecalculated for continuous data. c2 Tests were performed toexamine the relationships between purely categoricvariables and the provision of first aid. Where variableswere continuous, Kruskal-Wallis and Mann-Whitney testswere used.Associations between cool running water first aid andeach outcome variable were evaluated by performing 3separate comparisons, based on different categorizations offirst-aid duration and type. The primary analysis involvedthe comparison of wounds given adequate first aidcomposed of greater than or equal to 20 minutes of coolrunning water to those managed inadequately with anyother form of first aid. Further comparisons wereconducted between cool running water-treated burns andVolume 75, no. 1 : January 2020Cool Running Water First Aid for Pediatric Burnsthose that received either no first aid or an alternative tocool running water, and the 6 durational categories of firstaid outlined previously.The relationship between adequate cool running waterand the studied clinical outcomes was evaluated first by therisk difference and 95% CI. Additionally, associations withgrafting, hospital admission, and operating roomintervention were assessed by binomial logistic regressionmodels. A multinomial logistic regression model was usedto identify any associations with depth. From these logisticregressions, odds ratios (ORs) for the outcome variables, aswell as 95% CI, were estimated. Hazard ratios (HRs) and95% CI of time to re-epithelialization and hospital lengthof stay were determined with Cox regression models. Toassess the relationship between first aid and healing inburns at greatest risk of scarring, subgroup analyses—alsoinvolving Cox regression models—were conducted toestimate HR and 95% CI of time to re-epithelialization inburns requiring greater than or equal to 10 days to reepithelialize. This threshold was selected in light of thestudy by Cubison et al29 of hypertrophic scar formation inchildren with scald injuries, which identified 10 to 14 daysas the shortest period of burn wound healing associatedwith scarring. In accordance with the practices andrecommendations of previous studies investigating first aidfor burns,18,19 all regression models were adjusted for age,sex, socioeconomic status, mechanism of injury, and totalbody surface area. Logistic regression was chosen over othermethods such as propensity score matching, given itsprecedence of use in burns first aid literature and evidencesuggesting it has less bias in cohorts with large numbers ofevents per confounder.30 P .05 was accepted as statisticallysignificant. All data analyses were conducted with SPSS(version 25; SPSS, Inc., Chicago, IL).RESULTSCharacteristics of Study SubjectsDuring the study period, 2,769 patients attended thepediatric burn center. Interviews were conducted with thefamilies of 2,691 children (Figure 1). The study excluded175 cases with a nonthermal burn and 21 cases withunknown first-aid type, duration, or both.Among the remaining 2,495 patients, the median agewas 2 years (interquartile range [IQR] 1.0 to 6.0 years)(Table 1). Male participants composed 59.1% (n¼1,462)of the cohort. Scalds were identified as the mechanism ofinjury in 49.1% of cases (n¼1,224). A majority of injuriesoccurred in the home (85.3%; n¼2,108), and themost commonly affected body site was the upper limbs(40.3%; n¼993).Annals of Emergency Medicine 77
Griffin et alCool Running Water First Aid for Pediatric BurnsTable 1. Patient and wound demographics.VariableMedian (IQR)NPatient age, y2 (1–6)2,494Total body surface area percentage affected1 (0.5–2.0)2,485%SexMale e4.8119Radiant rm2.151Recreation/sports3.894School or residential1.639Street0.614Other0.820Upper limb40.3993Multiple24.5604Lower limbMechanism of injuryFigure 1. Participant flow. CRW, Cool running water.Place of injuryHomeMost patients first presented to an ED during theirinitial care. Local hospital EDs were responsible for 56.2%(n¼1,402) of the referrals to the burn center, and another36.9% (n¼921) were made by the participating hospital’sown ED. The remaining patients were referred from ageneral practice (5.0%; n¼124) or another source (eg, apediatrician, self-referral) (1.9%; n¼48).There was a median delay of 3.0 days (IQR 2.0 to 4.0days) between injury and presentation to the burn center.At initial assessment by burn service clinicians, the mediantotal body surface area was 1.0% (IQR 0.5% to 2.0%),with a range of less than 1% to 84%. Injuries with a totalbody surface area of 5% or greater composed 10.3%(n¼255) of the sample. Most burns were classified assuperficial and partial thickness in depth (65.7%;n¼1,604).Body part injured22.3549Torso9.2228Head3.893Total body surface area percentage affected 589.72,2305–107.2179 103.176Wound depthMain ResultsFully 96.8% of all patients (95% CI 96.1% to 97.4%;n¼2,414) had received some form of first aid within 3hours of injury. Greater than 9 in 10 patients (90.6%; 95%CI 89.4% to 91.7%; n¼2,259) had their burns cooledwith running water, but far fewer, 71.3% (95% CI 69.6%to 73.1%; n¼1,780), were given the recommended 20minutes of cool running water. Of these patients, only 789(44.3%; 95% CI 42% to 47%) were administered thecomplete duration of adequate cooling at the scene of theinjury. Among the 152 children provided an alternative tocool running water, the most common treatments were stillwater (23.0%; n¼35), ice (21.1%; n¼32), and coldcompresses (16.4%; n¼25).Adequate first-aid provision was significantly associatedwith injury mechanism (c2¼109.4; P .001). The highestproportions of adequately treated patients were those withscalds (77.7%), followed by contact burns (67.7%), flame78 Annals of Emergency MedicineSuperficial3.278Superficial partial thickness65.71,604Deep dermal partial thickness27.16614.1100Full thicknessData were complete for mechanism, operating room interventions, and hospitaladmission. Categories in which data were missing included age (n¼1; 0.08%), totalbody surface area percentage affected (n¼10; 0.40%), sex (n¼21; 0.88%), place ofinjury (n¼25; 1.00%), body part injured (n¼28; 1.12%), and wound depth (n¼52;2.08%).injuries (59.7%), and radiant heat burns (8.3%). There wasno association with age (Z¼–0.911; P¼.36), sex(c2¼109.4; P¼.17), or total body surface area (Z¼–0.4;P¼.72).Table 2 describes the differences in clinical outcomesand burn severity with adequate and inadequate first aid.Skin grafting was undertaken in 9.5% of cases (95% CI8.3% to 10.6%; n¼236). The administration of adequateVolume 75, no. 1 : January 2020
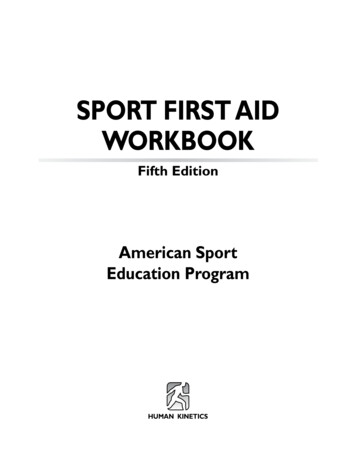
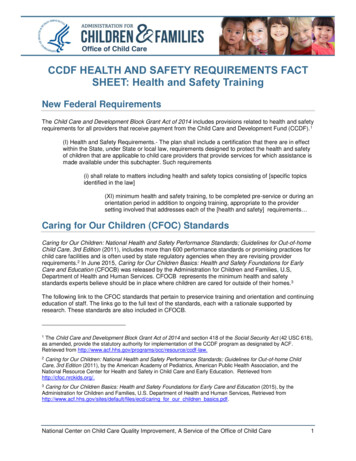
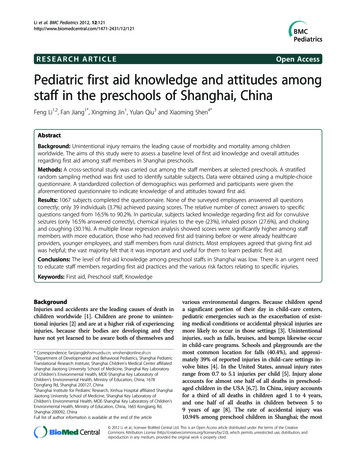
Griffin et alCool Running Water First Aid for Pediatric BurnsTable 2. Differences in clinical outcomes with adequate and inadequate first aid.OutcomeSkin graftingAdequate First Aid (n[1,780)Inadequate First Aid .6(1.3)–5.8(–4.5 to –7.0)95% CIFull-thickness depth472.7(0.4)537.6(1.0)–4.7(–3.7 to –6.1)Hospital admission23413.2(0.8)12918.0(1.4)–4.9(–3.7 to –6.15)Operating room intervention17810.0(0.7)10715.0(1.3)–5.0(–3.7 to –6.2)All burns10.0—†(7.0 to 14.0)10.0—(7.0 to 15.0)0.0(0.0 to –1.0)Burns requiring 10 days to re-epithelialize13.0—(10.0 to 18.0)14.0—(11.0 to 20.0)–1.0(–1.0 to –2.0)3.0—(1.0 to 10.0)3.0—(1.0 to 11.8)0.0(0.0 to –1.8)Time to re-epithelialization, median, daysHospital length of stay, median time, days*Unless otherwise stated.†Dashes indicate not applicable.cool running water first aid was associated with a decreasedneed for grafting; relative to all other forms of first aid,adequate cool running water yielded an OR of 0.6 (95% CI0.4 to 0.8; P .001) (Figure 2).The odds of receiving skin grafting were reduced by44.1% (OR¼0.6; 95% CI 0.4 to 0.9; P¼.007) in childrenprovided any amount of cooling with running water(Table E1, available online at http://www.annemergmed.com). A dose-response relationship was noted between theodds of grafting and duration of cool running water(Figure 3). Compared with children who received notreatment, those who were administered greater than orequal to 5 minutes of cool running water or an alternativehad significantly decreased odds of receiving grafting.Among burns that did not require grafting, median timeto re-epithelialization was 10 days (IQR 7 to 14 days). Thelikelihood of re-epithelialization was 29% greater amongcool running water-treated injuries (HR¼1.3; 95% CI 1.1to 1.5; P¼.003) (Table 3) per day postburn. However,administration of cool running water was not associatedwith a decrease in median time to re-epithelialization. Acomparison of adequately and inadequately treated burnsyielded no significant difference in re-epithelializationamong all wounds (HR¼1.1; 95% CI 1.0 to 1.2; P¼.06).For the 1,198 burns (59.2%) requiring 10 days or longer tore-epithelialize, however, wound closure was significantlyfaster after the application of adequate first aid (HR¼1.2;95% CI 1.0 to 1.3; P¼.04), with a reduction in mediantime to re-epithelialization of 1 day, from 14 to 13 days.A significant inverse relationship was observed betweenduration of first aid and odds of full-thickness depth.Relative to burns that failed to receive any first aid, thosecooled with running water for lengths of 5 minutes orgreater had significantly reduced odds of classification asfull thickness, with progressively greater odds reductions inVolume 75, no. 1 : January 2020the 5- to 10-minute (OR¼0.3; 95% CI 0.1 to 1.0; P¼.04),11- to 19-minute (OR¼0.3; 95% CI 0.1 to 0.9; P¼.03),and greater than or equal to 20-minute (OR¼0.2; 95% CI0.1 to 0.4; P .001) groups (Table E1, available online athttp://www.annemergmed.com). Compared withtreatments of no first aid or an alternative, the provision ofany cool running water was associated with an OR of 0.3(95% CI 0.2 to 0.6; P .001). The odds of patients whoreceived adequate first aid presenting with a full-thicknessburn were 62.6% lower than those of children given anyother form of first aid (OR¼0.4; 95% CI 0.2 to 0.6;P .001). Figure 4 illustrates the nonlinear relationshipbetween the probability of full-thickness depth and totalbody surface area, which suggests that the benefit ofadequate first aid might be greatest in larger burns between10% and 40% total body surface area. However, thetrend—which was also observed in the context of skingrafting—must be viewed cautiously because this rangerepresents only 3.7% of the cohort (n¼91).Overall, 14.5% of patients (95% CI 13.2% to 15.9%;n¼363) were admitted to the hospital at some point duringtheir management. The odds of admission decreased by35.8% with the provision of any cool running water(OR¼0.6; 95% CI 0.4 to 1.0; P¼.03) and by 31.0% withthe application of adequate first aid (OR¼0.7; 95% CI 0.3to 0.9; P¼.006).For those admitted as inpatients, median hospital length ofstay was 3 days (IQR 1 to 10 days). Cox regression analysesrevealed no significant associations with first aid. Length ofstay did not significantly change with the provision of anycool running water (HR¼0.7; 95% CI 0.5 to 1.0; P¼.07) oradequate first aid (HR¼0.9; 95% CI 0.7 to 1.2; P¼.48).Slightly more than 11% of patients (11.4%; 95% CI10.2% to 12.7%; n¼285) underwent treatment in anoperating room. The list of operating room interventionsAnnals of Emergency Medicine 79
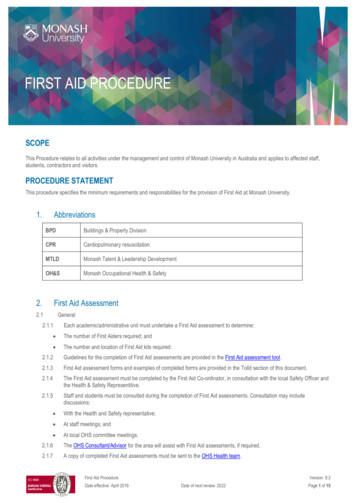
Cool Running Water First Aid for Pediatric BurnsGriffin et alFigure 2. Relationships between adequate first aid and each outcome measure. Error bars show 95% CIs.performed in this cohort included dressing changes undergeneral anesthetic, debridements, escharotomies, fullthickness skin grafts, scar revisions, split-thickness skingrafts, and steroid injections. Any amount of cooling withrunning water was associated with a 42.4% reduction inthe odds of intervention in an operating room (OR¼0.6;95% CI 0.4 to 0.9; P¼.008). Relative to that of childrengiven inadequate first aid, the OR of requiring an operatingroom intervention for recipients of adequate cool runningwater was 0.7 (95% CI 0.5 to 0.9; P¼.004).As with grafting, hospital admission and operating roomrequirements showed a dose-response relationship withfirst-aid duration. For both, the OR was significant for80 Annals of Emergency Medicinealternative treatment and all durations of cool runningwater greater than or equal to 5 minutes.The numbers of ICU admissions (n¼17) and deaths(n¼2) were too low to factor into the analysis.Table E2 (available online at http://www.annemergmed.com) documents the relationships between the covariatesand outcome variables.LIMITATIONSThe results must be interpreted in light of the followinglimitations. First, all cool running water treatments ofgreater than or equal to 20 minutes were categorized into asingle group. In their animal model, Bartlett et al10 foundVolume 75, no. 1 : January 2020
Griffin et alCool Running Water First Aid for Pediatric BurnsFigure 3. Dose-response relationships between first aid duration and each outcome measure. Error bars show 95% CIs.Table 3. Results of regression analyses evaluating the effect offirst aid on burn severity and clinical outcomes.OutcomeCrude OR/HRAdjusted OR/HR(95% CI)Skin graftingInadequate first aid1 (Reference)Adequate first aid0.540.59 (0.44–0.79)Full-thickness depthInadequate first aid1 (Reference)Adequate first aid0.320.37 (0.24–0.59)Hospital admissionInadequate first aid1 (Reference)Adequate first aid0.690.69 (0.33–0.90)Operating room interventionInadequate first aid1 (Reference)Adequate first aid0.630.66 (0.50–0.88)Time to re-epithelializationInadequate first aid1 (Reference)Adequate first aid1.071.10 (0.99–1.22)Hospital length of stayInadequate first aid1 (Reference)Adequate first aid1.140.92 (0.73–1.16)Results were controlled for age, sex, mechanism, socioeconomic status, and totalbody surface area percentage affected.Volume 75, no. 1 : January 2020that 30 minutes of cool running water yielded fewerbenefits than treatments of 20 minutes. Furthermore,Wood et al18 showed that first aid of greater than or equalto 40 minutes’ duration might actually be detrimental,possibly as a result of vasoconstriction and hypothermia.There are few documented cases in the literature ofhypothermia resulting from cool water treatment,31 but forsome patients, particularly young children with largerburns, application of cool running water for long durationscarries an obvious risk of thermoregulatory issues. A broadrange of total body surface areas was included in this study,although, consistent with the known epidemiology ofpediatric burns, the majority of the participants presentedwith wounds that were less than 5% total body surface area.The results therefore apply primarily to small- to mediumsized burns. Still, there was evidence of a clinical benefitwith adequate first aid in a substantial proportion of thelarger ( 5% total body surface area) injuries thatcomprised greater than one tenth of the cohort. Thefindings should not, however, be assumed to generalize tochemical, electrical, or friction burns because nonthermalmechanisms were excluded from the analysis.As a single-center study, this research has limitedexternal validity, and continued investigation is needed toconfirm its findings. Unlike past multicenter research,Annals of Emergency Medicine 81
Cool Running Water First Aid for Pediatric BurnsGriffin et alFigure 4. Associations between total body surface area and first aid for skin grafting, full-thickness depth, hospital admission, andoperating room intervention. Points represent mean probability for each given total body surface area value, as determined bylogistic regression models adjusting for age, sex, socioeconomic status, and mechanism of injury.however, this study did not have to estimate the duration ofa patient’s first aid; instead, detailed information aboutfirst-aid type and length was obtained directly fromparticipants and caregivers through structured interviews.These interviews carry an inherent risk of recall bias,especially in relation to elapsed time variables, which oftentend to be overestimated in retrospective reporting.Systematic overestimation of treatment exposure mightobscure the relationship between cool running waterduration and clinical outcomes and underestimate theintervention’s true effect. One possibly ameliorating factorwas the timing of the interviews, which were conducted amedian of only 3 days after the injury. Additionally, aninformal validation study of 100 randomly selected casesfrom the cohort revealed substantial agreement between theinterview data and contemporaneous ambulance reports,referral letters, and ED notes (Appendix E1, availableonline at http://www.annemergmed.com).Another limitation was the relatively low hospitaladmission rate, which might have biased the length-of-stayanalyses and contributed to their inconclusive findings; it ispossible that the sample of 363 inpatients was insufficientin size for a difference in length of stay to become apparent.82 Annals of Emergency MedicineThe analyses might have been further confounded byconcomitant injuries, infections, or social issues that mayhave delayed discharge.Finally, the noninterventional nature of the study precludesany definitive attribution of causality to first aid’s associationswith improved outcomes. Its findings, nevertheless, areconsistent with data from past human-subjects research.18,19DISCUSSIONThis cohort study of 2,495 children with thermal burnsfound that most of the clinical benefits of first aid previouslyreported in animal models4,10-12 and adult populations18,19were also present in the studied pediatric sample. The oddsof skin grafting were reduced by more than 40% in childrenprovided adequate first aid involving greater than or equal to20 minutes of cooling with running water.Among patients who did not require grafting, the speedof re-epithelialization was faster with the administration ofany cool running water. Adequate cooling, relative to allother forms of first aid, did not show a relationship withfaster re-epithelialization universally. However, amongburns in which the healing process was more protracted,spanning a period of 10 days or longer (ie, the wounds atVolume 75, no. 1 : January 2020
Griffin et algreatest risk of scarring), it was associated with significantlyimproved re-epithelialization speeds. Although small, thedecrease in median time to healing of 1 day with adequatefirst aid is far from inconsequential because recent researchdemonstrated that the odds of hypertrophic scarringincrease by a factor of 1.138 with each additional day takento achieve re-epithelialization.32By every metric besides hospital length of stay, burns thatwere cooled with running water fared significantly better thanthose that received no first aid or an alternative to cool runningwater. For emergency clinicians, these results highlight thesignificance of, at a minimum, initiating cooling in pediatricburn patients because any duration of cool running waterappears to be better than none. Even in scenarios in which thesize or distress of a child precludes extended periods of cooling,concerted efforts should be made to ensure the delivery of atleast some water first aid before any further care iscommenced. When possible, however, clinicians should aimfor longer durations because the data suggest that the extent offirst aid’s therapeutic benefit is contingent on the length oftime it is provided. The dose-response relationships betweencool running water duration and several outcome variablesclearly illustrate this point, none more so than its inversecorrelation with burn depth. Acro
likelihood of receiving first aid and poorer clinical outcomes among children with burns,24,25 patient socioeconomic status was assessed to be included as a covariate in the 76 Annals of Emergency Medicine Volume 75, no. 1 : January 2020 Cool Running Water