Transcription
You,YourChild&
A message from our SponsorThe future matters to our communities. Making contributions that have alasting, positive impact is the driving force behind TD Bank Financial Group’smany community giving programs.TD Bank Financial Group is pleased to provide financial support toThe Arthritis Society for the production of You, Your Child and Arthritis.Yo u , Yo u r C h i l d & A r t h r i t i sFinding useful information about children’s health issues can oftenbe difficult for families. As the sponsor of this new edition ofYou, Your Child and Arthritis, it was our goal to help provide families copingwith arthritis, access to current and reliable health information.Working together with the Arthritis Society, TD hopes to ensure abrighter future for all Canadian children.IntroductionThe mission of The Arthritis Society is to search for theunderlying causes, and subsequent cures for arthritis, and to promotethe best possible care and treatment for people with arthritis.The Arthritis Society provides education, support and solutions to peopleliving with arthritis, giving hope for a better life – today and tomorrow.The Arthritis Society is pleased to present the fourth edition ofYou, Your Child, and Arthritis. This publication providesfactual information, and should serve as a basis for you to ask questionsand gain further knowledge aboutjuvenile idiopathic arthritis andhow it may affect you and your family.4th EditionRevised by Shirley ML Tse, MD, FRCP(C)Assistant Professor of Pediatrics,University of TorontoPediatric RheumatologistThe Hospital for Sick Children(June 2005)You, Your Child and Arthritis was originally producedby the late Dr. Abraham Shore and Dr. James E. Boone.The 3rd Edition was revised by Dr. Ronald Laxer.We also thank Dr. Alex Levin and Dr. Nasrin Tehranifor their contributions to the section on eye problems and eye care.2www.arthritis.ca
ForewordIn 2004, a book entitled I am Brave: Children Living withArthritis was developed to give hope and inspiration tochildren living with arthritis. During its development,children from across Canada were asked to draw picturesand write stories about the emotional and physicalimpact of the disease on their day-to-day life.The fourth edition of You, Your Child & Arthritis presentedan opportunity to republish the compelling and creative artworkfirst showcased in I am Brave. The end result isa fun and informative book forchildren living with arthritis and those who care about them. On behalf ofThe Arthritis Society, I would like to thank the many artists who made such ameaningful contribution to this book.John E. FlemingPresident & CEO, The Arthritis SocietyArtistsBailey - page 10Brandon - page 15Callah - page 33Chesney - page 20, 21Ericka - page 17, 19, 20, 23Jaclyn - page 12Jennifer - page 27Laurence - page 10, 28Madeleine - page 14, 19, 31Melanie - page 11, 32Rebecca - page 18Tricia - page 15You,Your Child and Arthritis is a valuable resource for children andfamilies with newly diagnosed juvenile idiopathic arthritis (JIA) as well as a usefulreference for those who have had arthritis for years.This edition describes the newer terms which are now frequently used to classifythe types of chronic arthritis in children and provides updated information onmedications including the currently available biologic agents.Bianca Lang,MD FRCP(C)President,Canadian Pediatric Rheumatology AssociationYou,Your Child and Arthritis was created by The Arthritis Societyin conjunction with leading experts in pediatric rheumatology,young adults with JIA and parents of children with arthritis.www.arthritis.ca3
Table ofContentsAn OverviewWhat is Arthritis?What Causes Juvenile Idiopathic Arthritis?DiagnosisUnique Features of Juvenile Idiopathic Arthritis Growth Eye Problems UnpredictabilityYo u , Yo u r C h i l d & A r t h r i t i sPatterns and Types of Arthritis in Childhood456789 - 10991011 - 14 Oligoarticular-persistent JIA, Oligoarticular-extended JIA,Polyarticular-RF negative JIA, Polyarticular-RF positiveJIA, Systemic JIA, Enthesitis-Related-Arthritis, andPsoriatic ArthritisWhat Will Happen to Your Child?Treating Juvenile Idiopathic Arthritis Medications: Non-Steroidal Anti-Inflammatory Drugs,Aspirin, Steroids (Cortisone-Type Drugsincluding joint injections), Disease-ModifyingAnti-Rheumatic Drugs and Biologic Agents Newer Therapies Physiotherapy and Occupational Therapy Active Exercises General Physical Activities Splinting Rest Relief of Morning Stiffness Improvement Takes Time Eye Care SurgeryYour Family and Juvenile Idiopathic ArthritisIndependence and Learning to Cope With LifeYour Child and SchoolAdolescenceAims of TherapyA Word of EncouragementResearchAlternative TherapiesA Note to ParentsCommon Arthritis Termswww.arthritis.ca1516 - 26162021222323242424252627282830303132333334 - 36
Anoverview“Arthritis is not just adisease of old people.”Arthritis is not just a disease of old people. In fact, approximately 1 in 1,000 children under the age of16 suffers from arthritis, making the disorder more common than most chronic childhood disorders,including cystic fibrosis and diabetes. Previously, chronic childhood arthritis was referred to as juvenilerheumatoid arthritis (JRA) but arthritis in children is quite different from adult rheumatoid arthritis andis not always associated with the presenceof an arthritis associated autoantibody known as the rheumatoidfactor. As a result, many people now refer to chronic childhood arthritis as juvenile idiopathic arthritis orJIA. Idiopathic simply means“unknown” and is used when other known illnesses known to cause arthritisare ruled out such as infections, injuries, cancers, and other related rheumatic/autoimmune disorders(lupus, dermatomyositis, vasculitis). While research has not yet provided us with a cure for childhoodarthritis, there is effective therapy. Children who are followed closely, monitored carefully and adhere tothe recommended treatment provided by a multidisciplinaryteam do best overall and most are able toparticipate in normalactivities and have a bright future. Expanding research initiatives and the availabilityof more effective medications will allow us todo even better with this disease.Once your child has been diagnosed as having arthritis, theoverall treatment plan will be coordinatedby your child’s doctor, and will include medication and rehabilitation therapy. An exercise program,specially designed by your child’s doctor and therapists, is one of thecornerstones of treatment.Even if arthritis does cause jointdamage, the bones andcartilage of growing childrenhave amazing abilities to heal.Exercise helps prevent loss ofjoint movement and encourages normal growth.The medication prescribed by yourchild’s doctor acts to reduce jointswelling, pain and stiffness, preventjoint damage and makes the exerciseprogram easier for your child to do.The choice, nature and strengthof the medication will dependon the severity and type ofarthritis.www.arthritis.ca5
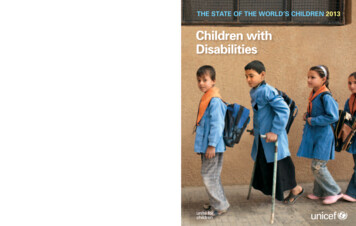
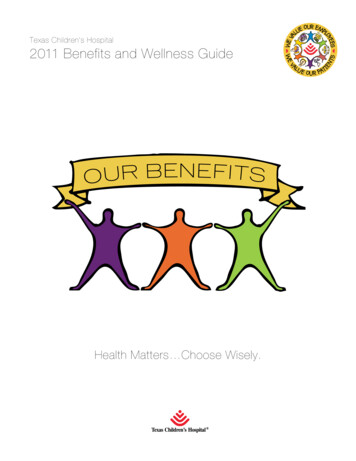
ArthritisBoneCartilageSynovial fluidYo u , Yo u r C h i l d & A r t h r i t i sSynovial liningNormaljointWhat isDamage tocartilageDamage tobonearthritis?Terms ending in “itis” refer to swelling or inflammation of a part of the body. “Tonsillitis,” forexample, refers to red, inflamed, painful tonsils. The term “arthritis” means swelling and inflammationof the joint lining. In JIA, this inflammation results in warm, stiff, swollen and often painful joints.It is important to know that not all joint pain is arthritis. Joint pain without inflammation, or arthralgia,is quite common and can occur in many conditions.A capsule encloses the joint space between two bones. The inner lining of this capsule, the synovium,produces a fluid that lubricates and nourishes the joint. The ends of the bones are covered with asmooth substance called cartilage, which allows the bone ends to glide smoothly across each other.In arthritis, imbalances in the immune system cause the synovium to become inflamed and thickened,producing extra fluid, which contains inflammatory cells. Inflammatory cells produce and releasesubstances that can cause the symptoms of joint inflammation (warmth, stiffness, swelling, pain)and, if left untreated, also lead to damage of the cartilage and underlying bone.6www.arthritis.ca
Whatcauses Juvenile Idiopathic Arthritis?No one knows. We do know that most subtypes of JIA do not run in families, and arthritis is almostnever passed from a parent to a child. Therefore, the chances of your child passing arthritis on tohis/her children would be extremely rare. JIA is not caused by any disease or infection that eitherparent may have had at any time, nor is it connected to any event during pregnancy. JIA is notcaused by eating the wrong foods, nor is there any proof that it can be improved by specific diets.Similarly, although many people feel that their arthritis is better in warm, dry climates, there is noscientific proof that JIA is caused or improved by any particular climate.The onset of JIA may follow a routine infection or injury, but such common events do not causechronic arthritis. It is currently believed that the body’s immune system may be responsible for theinflammation.The body’s immune system is a complex and finely tuned defence mechanism, whichfights infection by causing inflammation, as it does in tonsillitis.Tonsillitis is caused by an infection,and the sore, red, inflamed tonsils are signs that the body’s immune system is acting normally toeliminate this infection. In juvenile idiopathic arthritis, there is also inflammation of one or morejoints, but in contrast to tonsillitis, we do not know what causes this inflammation. In children witharthritis, the immune system seems to be overactive. It may respond inappropriately to infection ormistakenly identify something in the body for an infection, causing continuous inflammation.Although fever and rash may occur insome children with arthritis, juvenileidiopathic arthritis is definitely notcontagious.www.arthritis.ca7
DiagnosisYo u , Yo u r C h i l d & A r t h r i t i sChildren with arthritis do not always complain of pain.8As a result, it may be hard to tell if a child’s joints areinflamed. Sometimes the only initial clue to arthritis maybe that the child is stiff upon awakening in the morningor after a nap, and walks with a limp, or has some difficultyusing his or her arm or leg. Rarely, there may be no signsother than a swollen joint or some movement loss whenthe child is examined. Juvenile idiopathic arthritis can bedifficult to detect and may sometimes go unrecognizedby even the most experienced physician.Your child’s doctorwill look carefully for any signs of joint swelling or loss ofmobility, which indicate that the joints are inflamed.Juvenile idiopathic arthritis is defined as continuous inflammation of one or more jointslasting at least six weeks for which no other cause can be found in a child 16 years of age oryounger. Since arthritis may be a part of many different illnesses and there is no test that candefinitely diagnose juvenile idiopathic arthritis, tests to exclude other causes of joint pain andswelling must be done. Therefore your child will likely require X-rays and blood tests. Laboratorytests may also help in classifying your child’s type of arthritis and determining if your child is at riskof more severe disease. This may include testing for the autoantibodies such as rheumatoid factor(RF) and anti-nuclear antibody (ANA). In addition, once the diagnosis of JIA is confirmed, tests willneed to be repeated from time to time to monitor the illness and the effects of medication.The uncertainty and doubt of the first several weeks following discovery of the arthritis can resultin an emotionally difficult time for you, your child and your family. It is important for you to realizethat it may take time for your child’s doctor to be absolutely certain of the diagnosis of juvenileidiopathic arthritis. You must also understand that it may take up to several weeks or sometimeseven months for the medicines and exercises the doctor prescribes to have a noticeable effect.www.arthritis.ca
Unique Featuresof Juvenile Idiopathic ArthritisGrowthOne of the unique issues in JIA is the effect of inflammation on the growing child. There may belocal changes in the growth of individual joints that have been affected by arthritis. Inflammation canlead to accelerated growth. For example, knee inflammation may cause the leg to grow slightly fasterthan the non-inflamed side. The growth usually returns to normal once the arthritis has improved.Occasionally, if the inflammation is not well controlled, a slowing of growth may occur. For example,ongoing jaw inflammation may result in a small chin. Some-times, if the arthritis is severe and requiresmedications such as steroids, a generalized slowing of growth may occur.The growth will usuallyreturn to normal once the arthritis is controlled and the steroids are tapered or stopped. The healthcare team will pay careful attention to all aspects of your child's growth.Eye ProblemsSometimes a child with JIA may suffer from inflammation insidethe eye. This eye disorder goes by many names such as: uveitis,iritis, iridocyclitis, anterior uveitis, and nongranulomatous iritis.This inflammation often occurs without symptoms or visible signsso that you and your child may not be aware of its presence.Therefore, it is important for the child’s eyes to be checkedregularly, even if they are not red or painful. In the early stages,this inflammation can only be detected by a special examination(slit lamp examination), which must be done by an ophthalmologist(a physician specially trained in eye care and treatment) or anoptometrist (a non physician who has special training in performingeye examinations).often“Inflammationoccurs without symptomsor visible signs”www.arthritis.ca9
Yo u , Yo u r C h i l d & A r t h r i t i sIf your child develops uveitis, then yourchild shouldbe under the care of an ophthalmologist to receiveappropriate treatment. Your child’s doctor will makesure that regular eye examinations are arranged tofollow your child. Undetected, or inadequately treateduveitis can lead to cataract (a cloudiness in the lens of theeye), glaucoma (high pressure inside the eye), and/or band keratopathy (calcium deposition onthe surface of the eyeball) all of which can lead to vision loss or even blindness. Sometimes scartissue forms at the edge of the pupil (called posterior synechae) causing the pupil to be irregularin shape rather than the normal circle. Although this does not affect vision, it is a sign that there isor has been active uveitis. It is desirable to identify ongoing inflammation before synechae occur.For more information about the complications of uveitis, visit the website of the PediatricGlaucoma and Cataract Family Association (www.pgcfa.org).The uveitis is not related to the degreeof inflammation in the joints. Eye disease is, in fact, most common in children with only one or afew joints involved; it may even start before arthritis is diagnosed. Although uveitis can occur inany form of JIA it is most common in ANA positive, rheumatoid factor negative, young girls witholigoarticular JIA and older boys with polyarticular JIA. It can start in one or both eyes. If after6-12 months the uveitis affects only one eye, it is unusual for the uveitis to then affect the othereye, but ongoing regular visits to an eye doctor are essential. Some children have only oneepisode of uveitis that easily responds to treatment. Others may have recurrent uveitis thatresponds to treatment each time with periods of no inflammation in between bouts. A minorityof children (approximately 10% of those with uveitis) will have chronic ongoing uveitis that mayrequire months or years of treatment. These latter children are the ones most at risk for other eyecomplications and vision reduction.UnpredictabilityArthritis in children sometimes may last for as little as several months to a year and then disappearforever. Most children, however, have an up-and-down course for many years, depending on whattype of arthritis they have. Flares (also known as flare-ups or exacerbations) are those times whenthe arthritis seems to be getting worse. Some children may continue to have arthritis that extendsinto adulthood.Remissions are times when the arthritis appears to have goneaway. Sometimes, a mild infection, such as the ‘flu,’ maycause a flare. Usually, the reason for the flare is notidentified. It may be upsetting for parents to seesuch changes when it seemed the disease haddisappeared or had improved. Nevertheless, parentsshould not give up hope and should remain optimistic.Fortunately for most children, these flares tend tobecome less severe and occur less often with time.10www.arthritis.caMy arthritishas thiscolourand shape.
Patterns and Typesof Arthritis in ChildhoodThere is great variation in both the symptoms and nature of childhood arthritis. Therefore, once adoctor has diagnosed or questioned arthritis in your child, referral to a specialist, such as a pediatricrheumatologist (a physician specially trained in diagnosis, evaluation and treatment of disorders ofjoints, muscles and bones in children), will usually be required. A specific diagnosis is important andnecessary so that a specific treatment program can be designed for each individual child.There are 7 major subtypes of JIA: Oligoarticular – persistent JIA Oligoarticular – extended JIA Polyarticular – RF negative JIA Polyarticular – RF positive JIA Systemic JIA Enthesitis – related arthritis (ERA) Psoriatic arthritisThe subtype of JIA assigned for your child’s arthritis is largely based on information at the start of thedisease (physical examination findings, laboratory and imaging tests) but also on what happens withyour child’s disease course over the next 6-12 months. It is important for you to realize that it may taketime for your child’s doctor to be absolutely certain of the subtype of JIA and sometimes if your child’sdisease course changes, a different but more appropriate subtype will be assigned for your child’s JIA.However, the initial management of your child’s arthritis will not be hindered or delayed by not having aconfirmed subtype of JIA available. Knowledge of the subtype of JIA will ultimately help toprovide information to you, your child and health care providers about the expecteddisease course and to design a treatment plan specially customized to manage yourchild’s arthritis. The common features for each of these types of arthritis aresummarized on the following pages.On a bad day, my arthritis hurts.www.arthritis.ca11
Oligoarticular – Persistent JuvenileIdiopathic ArthritisYo u , Yo u r C h i l d & A r t h r i t i sThis is the name given to the most commonand generally mildest form of juvenile idiopathicarthritis. Oligoarticular (and sometimes calledpauciarticular) means involvement of few joints(4 or fewer joints). Children are classified as having oligoarticular – persistent JIA if beyond 6months after the initial start of arthritis, there isinvolvement of no more than 4 different jointsthroughout the course. Girls are affected muchmore commonly than boys. It usually starts inchildren four years of age or younger.The mostcommonly affected joints are the knee, ankle,wrist and elbow.There is little or no disturbanceof general health or growth.The course ofoligoarticular-persistent JIA may involve flaresand remissions, but with appropriate treatment,there is rarely permanent damage to the joints. Infact, many affected children will be in permanentremission within a few years after the onset of thedisease.Up to 20% of children with oligoarticularpersistent JIA will eventually develop uveitis.Therefore, all children with oligoarticular JIAshould have a regular, routine slit-lampexamination of their eyes at least three or fourtimes a year for the first few years after diagnosis.In children who develop eye inflammation, theblood test for antinuclear antibody (ANA) isalmost always positive. The ANA blood testtherefore helps to identify those children whowill require frequent eye checks.Oligoarticular – Extended JuvenileIdiopathic ArthritisAs described above, oligoarticular meansinvolvement of few joints (4 or fewer joints).However children are classified as having12www.arthritis.caoligoarticular – extended JIA if there isinvolvement of 4 or fewer joints within the first6 months after the initial start of arthritis, butbeyond 6 months of the disease course, thechild goes on to develop arthritis in new locationsresulting in 5 or more joints being affected indifferent locations anytime throughout thedisease course (remember that not all joints needto be active at the same time but importance isplaced on the number of different locations ofjoints affected). Large and small joints may beaffected. The course of oligoarticular-extendedJIA may involve flares and remissions, but withappropriate treatment, permanent damage tothe joints can usually be prevented. Associatedeye disease can also be present and childrenshould also have a regular, routine slit-lampexamination of their eyes at least three or fourtimes a year for the first few years afterdiagnosis. As mentioned above, inchildren who develop eye inflammation,the blood test for antinuclear antibody(ANA) is almost alwayspositive. The ANA bloodtest therefore helps toidentify those children whowill require frequenteye checks.Polyarticular – RheumatoidFactor Negative JuvenileIdiopathic ArthritisChildren with polyarticular-RF negative JIAhave many joints (five or more) involved withinthe first 6 months of disease but without apositive blood test for rheumatoid factor (RF).This type of juvenile idiopathic arthritis canbegin at any age, and usually, the arthritisstarts in several joints at the same time.
It is more common in girls than in boys.Occasionally it will begin in only one or twojoints, then spread to other joints. Of special note,two joints that may become involved in this typeof JIA are the temporomandibular joint (TMJ)and the cervical spine (neck). TMJ arthritis canlead to limited jaw opening and affect chewingas well as cause abnormal growth of the jawleading to a small chin. Your child’s doctor willcheck if these two joints are affected (physicalexamination and X-rays when indicated) andinform you and your child of any furthermanagement and precautions if necessary.The duration of polyarticular JIA varies from sixmonths to many years. In general, the arthritisruns a course that lasts several years. Interferencewith growth is less of a problem in polyarticularJIA than it is in systemic JIA, and inflammationof internal organs is rare.Polyarticular – Rheumatoid FactorPositive Juvenile Idiopathic ArthritisChildren with polyarticular-RF positive JIA havemany joints (five or more) involved within the first6 months of disease associated with a positiveblood test for rheumatoid factor (RF). This type ofjuvenile idiopathic arthritis can begin at any age,however, onset frequently occurs with older girls.Usually, the arthritis starts in several joints at thesame time.The onset of polyarticular-RF positiveJIA in teenagers may closely resemble adultrheumatoid arthritis (RA). It is more common inolder girls than in boys. Occasionally it will beginin only one or two joints, then spread to otherjoints. It can affect both the small (especially hands and fingers) and largejoints (knees, hips, ankles) usually on both sides of the body.Some children may also haveadditional findings such as alow-grade fever, rheumatoidnodules (bumps under the skin), anemia (lowred blood cell count or fall in hemoglobin level),significant fatigue, poor appetite and generalunwellness. This type of JIA has a greatertendency to cause severe joint damage thanother types of arthritis. Thus, stronger medicationsare recommended at an early stage for childrenwith polyarticular-RFpositive JIA.Systemic Juvenile IdiopathicArthritisThis form of JIA affects the body generallywith fever and can affect the child's internalorgans as well as joints and skin. Systemic JIAcan begin at any age and affects boys and girlsequally. It usually involves many different jointsand some joints may have severe disease.Children with systemic JIA have spiking(rapidly rising and falling) fever, which usuallyoccurs once (or sometimes twice) a day, and arash that frequently comes and goes with thefever. The rash usually appears as pale red spotson the child’s chest, upper arms, thighs and otherparts of the body. In addition, they often haveswollen lymph glands, and enlargement of theliver and spleen. They appear listless and unwellduring the fever (most often in the late afternoonor evening), only to brighten up by the next dayas their temperature returns to normal. Whenfever in systemic JIA persists for several weeks,the child will be weak, lose weight and maybecome pale from anemia (a fall in the level ofhemoglobin in the blood). Flares that last a longtime may also interfere with growth, althoughthe growth usually improves as thechild’s condition improves.Inflammation of internalorgans may cause stomachpain or affect the heart orlungs but will not causepermanent damage.even severe“forms of arthritissometimes go intoremission within afew years”www.arthritis.ca13
Yo u , Yo u r C h i l d & A r t h r i t i s14In the early stages of systemic JIA, there issometimes no sign of joint inflammation.Thismay make it a very difficult disease to diagnosebecause there are many other illnesses that alsocause a fever and rash in children. Therefore,many tests are done.The arthritis usuallyappears within the first six months after thestart of the fever, and usually persists, even whenthe fever settles.The arthritis may be mild orsevere, and may involve just a few, or manyjoints. However, even severe forms of arthritissometimes go into remission within a few years.If the arthritis does not go into remission, it willfollow a pattern of “ups and downs”that isdifferent for each child. In most cases, the patternwill gradually become less severe. Occasionally,as with all forms of JIA, flares may occur after thedisease has been inactive for a long time.Medications used to treat children withsystemic JIA will include drugs that control notonly the arthritis but also the systemic part ofthe illness, such as the fever and anemia. Uveitisis uncommon in systemic JIA but childrenshould still have their eyes examined annually.Enthesitis – Related – ArthritisChildren with enthesitis-related-arthritis(ERA) demonstrate inflammationboth in their joints (arthritis) andentheses (enthesitis). Entheses arespots where tendons attachor insert into bones. Thistype of JIA generally affectschildren over the age of 10,and is the only type of JIA that ismore common in boys. It usuallyinvolves just a few joints in thelower limbs and commonly affectsthe hips. Joint inflammation inERA often persists into adulthood.This form of arthritis may sometimeswww.arthritis.caprogress to involvement of the spine or sacroiliacjoints and lead to pain and stiffness of the back.Entheses in the lower limbs are usually affected,especially around the knees, ankles and bottomof the feet, and therefore children may oftencomplain of knee, heel or foot pain particularlywith activity. ERA is one of the few types ofarthritis that may be hereditary or run in families.It may also occur with inflammation of the eyes,or bowel, either in the patient or in other familymembers. Many children with ERA carry aprotein called HLA B-27 on their cells.Testingfor this protein in the laboratory may help inthe diagnosis in some cases.Psoriatic ArthritisPsoriasis is a skin disease that is accompaniedby arthritis in many cases. Psoriasis appears asa scaly red rash usually on the scalp, behindthe ears, on the eyelids, elbows, knees, buttocksor in the belly button. Some children may alsohave changes on their fingernails (pitting orridging). When arthritis and psoriasis occurtogether, the disease is called psoriatic JIA.Thistype of arthritis can occur at any age affectingboth boys and girls. It often affects only one or afew joints but may also involve the hips or back(like in enthesitis-related-arthritis), or the fingersand toes. In some children, the swelling in thefingers or toes may be soextensive that the digit appearslike a sausage. This is due toinflammation and swelling in thetendon of a finger or toe and isreferred to as dactylitis. In about halfof children with psoriaticarthritis, the arthritisstarts before any sign ofskin disease. For this reason, afamily history of psoriasis willhelp your child’s doctor to diagnosethis type of arthritis.
What willHappen to your Child?Although the long-term outlook for most children with arthritis is usually good, it is impossible topredict exactly what will happen to your child. It is true that the longer the disease remains active, thegreater the risk of joint damage. Once your child has established a pattern of disease, your health careteam will be able to give you a general idea of the future.To achieve the best possible outcome, you and your child will need to work very closely with thearthritis treatment team. This may include your child’s doctor, a nurse, a physiotherapist, an occupationaltherapist, a social worker, psychologist, dietician, an orthopedic surgeon, an ophthalmologist (oroptometrist if your child does not have active uveitis or related eye problems needing treatment), adentist and your child’s teachers. The specific members of the team involved in the care of your child willbe determined by the nature of the arthritis and his or her special needs. The most important membersof the team are you and your child. With help and guidance of the team, your child can deal with evensevere arthritis.The attitude and emotional response of a child and his or her family are extremely important indetermining
www.arthritis.ca 3 Foreword In 2004, a book entitled I am Brave: Children Living with Arthritis was developed to give hope and inspiration to children living with arthritis.During its development, children from across Canada were asked to draw pictures and write stories about the emotional a