Transcription
http://ebook2book.ir/
USMLE STEP 2 CK: PEDIATRICSLecture Noteshttp://ebook2book.ir/
2019http://ebook2book.ir/
Table of ContentsUSMLE Step 2 CK Lecture Notes 2019: PediatricsCoverTitle PageCopyrightEditorsFeedback PageChapter 1: The NewbornApgar ScoreBirth InjuriesPhysical Examination: Normal FindingsNewborn ScreeningFetal Growth and MaturitySpecific DisordersInfectionsSubstance Abuse and Neonatal WithdrawalChapter 2: Genetics/DysmorphologyAbnormalities of ChromosomesEarly Overgrowth with Associated DefectsUnusual Brain and/or Neuromuscular Findings with Associated DefectsFacial Features as the Major DefectOsteochondrodysplasiasConnective Tissue DisordersEnvironmental AgentsMiscellaneous SequencesMiscellaneous AssociationsChapter 3: Growth and NutritionChildhood GrowthDisorders of GrowthFeedingBreast FeedingSolidsChapter 4: DevelopmentOverviewPrimitive Reflexes and Developmental MilestonesChapter 5: Behavioral/Psychological DisordersEating DisordersElimination DisordersSleep DisordersChapter 6: ImmunizationsActive ImmunizationsActive Immunization after Disease ExposureSpecific Vaccines (Routine Vaccinations)http://ebook2book.ir/
Chapter 7: Child Abuse and NeglectIntroductionPhysical AbuseSexual AbuseChapter 8: Respiratory DiseaseAcute Inflammatory Upper Airway ObstructionCongenital Anomalies of the LarynxAirway Foreign BodyInflammatory Disorders of the Small AirwaysPneumoniaCystic Fibrosis (CF)Sudden Infant Death Syndrome (SIDS)Chapter 9: Allergy and AsthmaAllergiesAsthmaChapter 10: Immune-Mediated DiseaseEvaluation of Suspected Immune DeficiencySpecific DefectsOther Immune DeficienciesChapter 11: Disorders of the EyeAbnormalities of the Eye StructuresEye InjuriesPeriorbital versus Orbital CellulitisChapter 12: Disorders of the Ear, Nose, and Throat .EarsNose and ThroatChapter 13: CardiologyCardiac Evaluation and Congenital Heart LesionsPediatric Heart Sounds and Innocent MurmursLeft to Right ShuntsStenotic LesionsRight to Left Shunts (Cyanotic Lesions)Mixed LesionsRegurgitant LesionsOther Cardiac PathologyHypertensionChapter 14: Gastrointestinal DiseaseOral ionChapter 15: Renal and Urologic DisordersUrinary Tract Infection (UTI)Vesicoureteral Reflux (VUR)Obstructive UropathyDiseases Presenting Primarily withhttp://ebook2book.ir/Hematuria
Polycystic Kidney DiseaseDiseases Presenting with ProteinuriaMale Genitourinary DisordersChapter 16: Endocrine DisordersPituitary DisordersThyroid DisordersParathyroid DisordersAdrenal DisordersDiabetes MellitusChapter 17: Orthopedic DisordersDisorders of the HipIntoeingDisorders of the KneeDisorders of the SpineDisorders of the Upper LimbOsteomyelitis and Septic ArthritisOsteogenesis ImperfectaBone TumorsChapter 18: Rheumatic and Vasculitic DisordersJuvenile Idiopathic Arthritis (JIA)Systemic Lupus Erythematosus (SLE)Neonatal LupusKawasaki DiseaseHenoch-Schönlein Purpura (HSP)Chapter 19: HematologyAnemias of Inadequate ProductionCongenital AnemiasAcquired AnemiasMegaloblastic AnemiasHemolytic AnemiasHemoglobin DisordersThalassemiasHemorrhagic DisordersPlatelet DisordersChapter 20: OncologyLeukemia and LymphomaBrain TumorsOther MalignanciesChapter 21: NeurologyCentral Nervous System (CNS) AnomaliesSeizuresNeurocutaneous SyndromesEncephalopathiesNeurodegenerative DisordersNeuromuscular DiseaseChapter 22: Infectious Diseasehttp://ebook2book.ir/Meningitis
PertussisMycobacteriaLyme DiseaseRocky Mountain Spotted FeverMycotic InfectionsViral InfectionsOther Viral DiseasesHelminthic DiseasesChapter 23: AdolescenceMortality/Morbidity, Sexuality, and STIsAcnehttp://ebook2book.ir/
http://ebook2book.ir/
USMLE is a joint program of the Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME),neither of which sponsors or endorses this product.This publication is designed to provide accurate information in regard to the subject matter covered as of its publication date, with theunderstanding that knowledge and best practice constantly evolve. The publisher is not engaged in rendering medical, legal, accounting, orother professional service. If medical or legal advice or other expert assistance is required, the services of a competent professional should besought. This publication is not intended for use in clinical practice or the delivery of medical care. To the fullest extent of the law, neither thePublisher nor the Editors assume any liability for any injury and/or damage to persons or property arising out of or related to any use of thematerial contained in this book. 2018 by Kaplan, Inc.Published by Kaplan Medical, a division of Kaplan, Inc.750 Third AvenueNew York, NY 10017All rights reserved under International and Pan-American Copyright Conventions. By payment of the required fees, you have been granted thenon-exclusive, non-transferable right to access and read the text of this eBook on screen. No part of this text may be reproduced, transmitted,downloaded, decompiled, reverse engineered, or stored in or introduced into any information storage and retrieval system, in any form or byany means, whether electronic or mechanical, now known or hereinafter invented, without the express written permission of the publisher.ISBN-13: 978-1-5062-3629-2http://ebook2book.ir/
EDITORSWilliam G. Cvetnic, MD, MBAFellow of the American Academy of PediatricsBoard Certified in Pediatrics and Neonatal-Perinatal MedicineJacksonville, FloridaEduardo Pino, MDAssociate Professor, Department of PediatricsMarshall University School of MedicineMedical Director, Hoops Family Children's HospitalCabell Huntington HospitalHuntington, West Virginiahttp://ebook2book.ir/
We want to hear what you think. What do you like or not like about the Notes? Please email us atmedfeedback@kaplan.com.http://ebook2book.ir/
THE NEWBORNhttp://ebook2book.ir/
LEARNING OBJECTIVESCalculate an Apgar scoreUse knowledge of birth injuries to predict symptomologyDemonstrate understanding of newborn screening, fetal growth/maturity, and neonatal infectionshttp://ebook2book.ir/
APGAR SCOREA newborn infant at birth is noted to have acrocyanosis, heart rate 140/min, and grimaces tostimulation. She is active and has a lusty cry. What is her Apgar score?Evaluation0 Points1 Point2 PointsHeart rate0 100/min 100/minRespirationNoneIrregular, shallow, gaspsCryingColorBluePale, blue extremitiesPinkToneNoneWeak, passiveActiveReflex irritabilityNoneFacial grimaceActive withdrawalTable 1-1.Apgar Scoring SystemApgar scores are routinely assessed at 1 and 5 minutes, and every 5 minutes thereafter as long asresuscitation is continuing.The 1-minute score gives an idea of what was going on during labor and delivery.The 5-minute score gives an idea of response to therapy (resuscitation).In general, the Apgar score is not predictive of outcome; however, infants with score 0 3 at 5 minutescompared to infants with score 7 10 have a worse neurologic outcome.http://ebook2book.ir/
NEWBORN CAREVitamin K IMProphylactic eye erythromycinUmbilical cord careHearing testNewborn screening testshttp://ebook2book.ir/
BIRTH INJURIESOn physical exam, a 12-hour-old newborn is noted to have nontender swelling of the head that doesnot cross the suture line. What is the most likely diagnosis?InjurySpecificsSkull fracturesIn utero from pressure against bones orLinear: no symptoms and no treatment neededforceps; linear: most commonDepressed: elevate to prevent cortical injuryBrachial palsyOutcomeErb-Duchenne: C5–C6; cannot abductMost with full recovery (months); depends on whether nerve wasshoulder; externally rotate and supinateinjured or lacerated; Rx: proper positioning and partialforearm; Klumpke: C7–C8 T1; paralyzedimmobilization; massage and range of motion exercises; if nohand Horner syndromerecovery in 3–6 mo, then neuroplastyClavicularEspecially with shoulder dystocia in vertexPalpable callus within a week; Rx: with immobilization of arm andfractureposition and arm extension in breechshoulderFacial nerve palsyEntire side of face with forehead; forcepsImprovement over weeks (as long as fibers were not torn); needdelivery or in utero pressure over facialeye care; neuroplasty if no improvement (torn fibers)nerveCaputDiffuse edematous swelling of soft tissues ofsuccedaneumscalp; crosses suture linesCephalohematomaSubperiosteal hemorrhage: does not crossMay have underlying linear fracture; resolve in 2 wk to 3 mo; maysuture linescalcify; jaundiceTable 1-2.Disappears in first few days; may lead to molding for weeksCommon Injuries During Deliverieshttp://ebook2book.ir/
PHYSICAL EXAMINATION: NORMALFINDINGSA newborn infant has a blue-gray pigmented lesion on the sacral area. It is clearly demarcated anddoes not fade into the surrounding skin. What is the most likely diagnosis?A newborn has a flat, salmon-colored lesion on the glabella, which becomes darker red when hecries. What is the best course of INCutis marmorataLacy, reticulated vascular pattern over most of body when baby is cooled; improves over first month; abnormal ifpersistsSalmon patchPale, pink vascular macules; found in nuchal area, glabella, eyelids; usually disappears(nevus simplex)Mongolian spotsBlue to slate-gray macules; seen on presacral, back, posterior thighs; in nonwhite infants; arrested melanocytes;usually fade over first few years; differential: child abuseErythemaFirm, yellow-white papules/pustules with erythematous base; peaks on second day of life; contain eosinophils; benigntoxicum,neonatorumHemangiomaSuperficial: bright red, protuberant, sharply demarcated; most often appear in first 2 months; most on face, scalp,back, anterior chest; rapid expansion, then stationary, then involution (most by 5–9 years of age); Rx: beta blockers,embolization; deeper: bluish hue, firm, cystic, less likely to regress; Rx: (steroids, pulsed laser) only if large andinterfering with functionHEADPreauricularLook for hearing loss and genitourinary anomalies.tags/pitsColoboma of irisCleft at “six o’clock” position; most with other eye abnormalities; CHARGE associationAniridiaHypoplasia of iris; defect may go through to retina; association with Wilms tumorEXTREMITIESPolydactyly 5 number of fingers or toes. No treatment needed if good blood supply.Table 1-3.http://ebook2book.ir/Physical Examination—Common Findings
NEWBORN SCREENINGA 1-month-old fair-haired, fair-skinned baby presents with projectile vomiting of 4 days’ duration.Physical exam reveals a baby with eczema and a musty odor. Which screening test would most likelybe abnormal?Every newborn is screened before discharge or day 4 of life. It is more reliable if done after 48 hours oforal feedings (substrates for metabolic diseases).The total diseases screened are determined by the individual state. Some examples:PhenylketonuriaTyrosinemia21-hydroxylase deficiencyGalactosemiaHb SSHb CHypothyroidismCystic fibrosisPhenylketonuria (PKU)Classic GalactosemiaPhenylalanine hydroxylase; accumulation ofGal-1-P uridylyltransferase deficiency; accumulation of gal-1-P withPHE in body fluids and CNSinjury to kidney, liver, and brainMental retardation, vomiting, growthJaundice (often direct), hepatomegaly, vomiting, hypoglycemia,retardation, purposeless movements, athetosis,cataracts, seizures, poor feeding, poor weight gain, mentalseizuresretardationFair hair, fair skin, blue eyes, toothPredisposition to E. coli sepsis; developmental delay, speechabnormalities, microcephalydisorders, learning disabilitiesOtherNormal at birth; gradual MR over first fewMay begin prenatally—transplacental galactose from mothercommentsmonthsTreatmentLow PHE diet for lifeDefectPresentationAssociationsNo lactose—reverses growth failure, kidney and liver abnormalitiesand cataracts, but not neurodevelopmental problemsDefinition of abbreviations: CNS, central nervous system; G-1-P, galactose-1-phosphate; M R, mental retardation; PHE, phenylalanine.*Items in bold have a greater likelihood of appearing on the exam.Table 1-4.http://ebook2book.ir/Two Newborn Screening Diseases*
FETAL GROWTH AND MATURITYTypeReasonMain EtiologiesComplicationsSymmetricEarly, in utero insult that affectsGenetic syndromes, chromosomal abnormalities,Etiology dependent;growth of most organscongenital infections, teratogens, toxinsdelivery of oxygen andnutrients to vital organsusually normalAsymmetricRelatively late onset after fetalUteroplacental insufficiency secondary to maternalNeurologic (asphyxia) if(headorgan development; abnormaldiseases (malnutrition, cardiac, renal, anemia) and/orsignificant decreasedsparing)delivery of nutritional substancesplacental dysfunction (hypertension, autoimmunedelivery of oxygen toand oxygen to the fetusdisease, abruption)brainTable 1-5.PretermIntrauterine Growth Restriction (IUGR)Large for Gestational AgePost-term(LGA)—Fetal MacrosomiaPremature—liveborn infants delivered prior to 37Birth weight 4,500Infants born after 42 weeks’ gestationweeks as measured from the first day of the lastgrams at termfrom last menstrual periodmenstrual periodPredisposing factors:When delivery is delayed 3 weeksLow birth weight—birthweight 2,500 grams. Thisobesity, diabetespast term, significant increase inmay be due to prematurity, IUGR, or bothHigher incidence of birthmortality.injuries and congenitalCharacteristicsanomalies—Increased birth weight—Absence of lanugo—Decreased/absent vernix—Desquamating, pale, loose skin—Abundant hair, long nails—If placental insufficiency, may bemeconium stainingGestational Age and Size at Birthhttp://ebook2book.ir/
SPECIFIC DISORDERSENDOCRINE DISORDERSInfants of diabetic mothersYou are called to see a 9.5-pound newborn infant who is jittery. Physical exam reveals a largeplethoric infant who is tremulous. A murmur is heard. Blood sugar is low.Maternal hyperglycemia (types I and II DM) fetal hyperinsulinemiaInsulin is the major fetal growth hormone increase in size of all organs except the brainMajor metabolic effect is at birth with sudden placental separation hypoglycemiaInfants may be large for gestational age and plethoric (ruddy).Other metabolic findings: hypoglycemia and hypomagnesemia (felt to be a result of delayed actionof parathyroid hormone)Common findingsBirth trauma (macrosomia)Tachypnea (transient tachypnea, respiratory distress syndrome, cardiac failure, hypoglycemia)Cardiomegaly—asymmetric septal hypertrophy (insulin effect, reversible)Polycythemia (and hyperviscosity) hyperbilirubinemia jaundiceRenal vein thrombosis (flank mass, hematuria, and thrombocytopenia) from polycythemiaIncreased incidence of congenital anomaliesCardiac—especially VSD, ASD, transpositionSmall left colon syndrome (transient delay in development of left side of colon; presents withabdominal distention)Caudal regression syndrome: spectrum of structural neurologic defects of the caudal region ofspinal cord which may result in neurologic impairment (hypo, aplasia of pelvis & LE)Prognosis—Infants of diabetic mothers are more predisposed to diabetes and LGA infants are atincreased risk of childhood obesity.TreatmentMonitor carefully and advocate good glucose control during pregnancy. Follow glucose carefullyin infant after delivery.Early, frequent feeds: oral, NG if episodes of hypoglycemia continueIntravenous dextrose infusion if above does not result in euglycemiahttp://ebook2book.ir/
Clinical RecallWhich of the following is commonly seen in infants of diabetic mothers?A)MicrosomiaB)C)D)Small heart sizePolycythemiaRenal artery thrombosisE)Slow respiratory rateAnswer: Chttp://ebook2book.ir/
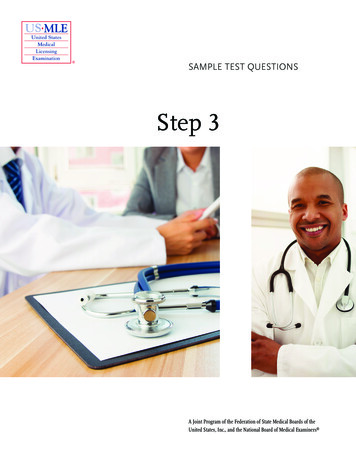
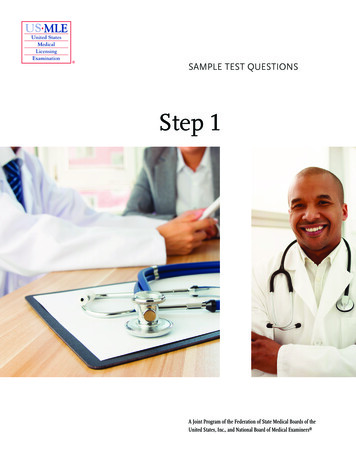
RESPIRATORY DISORDERSFigure 1-1. Respiratory DistressRespiratory distress syndrome (RDS)Shortly after birth, a 33-week gestation infant develops tachypnea, nasal flaring, and grunting andrequires intubation. Chest radiograph shows a hazy, ground-glass appearance of the lungs.Deficiency of mature surfactant (surfactant matures biochemically over gestation; therefore, theincidence of surfactant deficiency diminishes toward term.)Inability to maintain alveolar volume at end expiration decreased FRC (functional residualcapacity) and atelectasisPrimary initial pulmonary hallmark is hypoxemia. Then, hypercarbia and respiratory acidosis ensue.DiagnosisBest initial diagnostic test—chest radiographFindings: ground-glass appearance, atelectasis, air bronchogramsMost accurate diagnostic test—L/S ratio (part of complete lung profile; lecithin-tosphingomyelin ratio)Done on amniotic fluid prior to birthBest initial treatment—oxygenMost effective treatment—intubation and exogenous surfactant administrationPrimary preventionAvoid prematurity (tocolytics)Antenatal betamethasonehttp://ebook2book.ir/
Transient tachypnea of the newborn (TTN)Slow absorption of fetal lung fluid decreased pulmonary compliance and tidal volume withincreased dead spaceTachypnea after birthGenerally minimal oxygen requirementCommon in term infant delivered by Cesarean section or rapid second stage of laborChest x-ray (best test)—air-trapping, fluid in fissures, perihilar streakingRapid improvement generally within hours to a few daysMeconium aspirationMeconium passed as a result of hypoxia and fetal distress; may be aspirated in utero or with the firstpostnatal breath airway obstruction and pneumonitis failure and pulmonary hypertensionChest x-ray (best test)—patchy infiltrates, increased AP diameter, flattening of diaphragmOther complications—air leak (pneumothorax, pneumomediastinum)Prevention—endotracheal intubation and airway suction of depressed infants with thickmeconiumTreatment—positive pressure ventilation and other complex NICU therapiesDiaphragmatic herniaFailure of the diaphragm to close abdominal contents enter into chest, causing pulmonaryhypoplasia.Born with respiratory distress and scaphoid abdomenBowel sounds may be heard in chestDiagnosis—prenatal ultrasound; postnatal x-ray (best test) reveals bowel in chestBest initial treatment—immediate intubation in delivery room for known or suspected CDH, followedby surgical correction when stable (usually days)http://ebook2book.ir/
GASTROINTESTINAL AND HEPATOBILIARYDISORDERSSee also GI chapter on this topic.Umbilical herniaFailure of the umbilical ring closure, weakness of abdominal musclesMost are small and resolve in 1-2 years without any treatmentSurgery if getting larger after 1-2 years, symptoms (strangulation, incarceration), and/or persistent afterage 4OmphaloceleFailure of intestines to return to abdominal cavity with gut through umbilicusCovered in a sac (protection)Associated with other major malformations and possible genetic disorders (trisomy)Large defects need a staged reduction (use of a surgical Silo), otherwise respiratory failure andischemiaGastroschisisDefect in abdominal wall lateral to umbilicus (vascular accident)Any part of the GI tract may protrudeNot covered by a sacMajor problem with the intestines: atresia, stenosis, ischemia, short gutSurgery based on condition of gut; if no ischemia, large lesions need a staged reduction as withomphaloceleNecrotizing enterocolitis (NEC)Transmural intestinal necrosisGreatest risk factor is prematurity; rare in term infantsSymptoms usually related to introduction of feeds: bloody stools, apnea, lethargy, and abdominaldistention once perforation has occurredhttp://ebook2book.ir/
Pneumatosis intestinalis on plain abdominal film is pathognomonic (air in bowel wall)Treatment: cessation of feeds, gut decompression, systemic antibiotics, and supportive care; surgicalresection of necrotic bowel may be necessaryImperforate anusFailure to pass stool after birthNo anal opening visibleTreatment is surgical correction.May be part of VACTERL association.JaundiceA 2-day-old infant is noticed to be jaundiced. He is nursing and stooling well. Indirect bilirubin is11.2 mg/dL; direct is 0.4 mg/dL. Physical exam is unremarkable except for visible jaundice.PathophysiologyIncreased production of bilirubin from breakdown of fetal red blood cells plus immaturity ofhepatic conjugation of bilirubin and elimination in first week of lifeRapidly increasing unconjugated (indirect reacting) bilirubin can cross the blood-brain barrierand lead to kernicterus (unconjugated bilirubin in the basal ganglia and brain stem nuclei).Hypotonia, seizures, opisthotonos, delayed motor skills, choreoathetosis, and sensorineuralhearing loss are features of kernicterus.Physiologic JaundicePathologic JaundiceAppears on second to third day of life (term)May appear in first 24 hours of lifeDisappears by fifth day of life (term)—7thVariablePeaks at second to third day of lifeVariablePeak bilirubin 13 mg/dL (term)UnlimitedRate of bilirubin rise 5 mg/dL/dUsually 5 mg/dL/dTable 1-6.Physiologic Jaundice Versus Pathologic Jaundicehttp://ebook2book.ir/
NOTEWork up for pathologic hyperbilirubinemia when:It appears on the first day of lifeBilirubin rises 5 mg/dL/dayBilirubin 13 mg/dL in term infantDirect bilirubin 2 mg/dL at any timeThe causes of hyperbilirubinemia with respect to bilirubin metabolism are as follows:RBC metabolismIncreased number of RBCsv.Normal newborn (normal Hct 42 65)Physiologic jaundicePolycythemia (Hct 65).ii.Increased RBC production: Chronic hypoxia, IUGR, post-mature; IODM, BeckwithWiedemann syndrome (insulin effect); maternal Graves’ disease (transplacental antibodies);trisomies (unknowm mechanism)Extra RBCs entering the circulation: delayed cord clamping, twin-twin transfusionTreatment: partial exchange transfusion with normal saline (dilutional)Increased hemolysisImmune-mediated (labs: high unconjugated bilirubin, may be anemia, increased reticulocytecount, positive direct Coombs test)Rh negative mother/Rh positive baby: classic hemolytic disease of the newborn(erythroblastosis fetalis).ii.ii.ABO incompatibility (almost all are type O mother and either type A or B baby): mostcommon reason for hemolysis in the newbornMinor blood group incompatibility (Kell is very antigenic; Kell negative mother),uncommonNon-immune mediated: same as above but Coombs is negative; need to see blood smearSmear shows characteristic-looking RBCs: membrane defect (most are eitherspherocytosis or elliptocytosis)Smear shows normal-looking RBCs: enzyme defect (most are G6PD deficiency thenpyruvate kinase deficiency)Extravascular: excessive bruising,cephalohematomahttp://ebook2book.ir/
Bilirubin is then bound to albumin and carried in the blood; bilirubin may be uncoupled from albuminin the blood stream to yield free bilirubin, e.g. neonatal sepsis, certain drugs (ceftriaxone), hypoxia,acidosis.Bilirubin is transported to the hepatocytes: within the hepatocytes is the conversion of unconjugated(laboratory indirect-acting) fat-soluble bilirubin to conjugated (glucuronide) water-soluble bilirubin(laboratory direct-acting) by the action of hepatic glucuronyl transferase (GT).Decreased enzymatic activity of GTNormal newborn first week of lifePrimary liver disease of systemic disease affecting the liver (sepsis, TORCH, metabolicdiseases)No GT activity: Crigler-Najjar syndrome (type I)Transport through the intrahepatic biliary system to the porta hepatis for excretion into the duodenum;abnormalities of transport and excretion cause a conjugated (direct) hyperbilirubinemia ( 2 mg/dLdirect-acting bilirubin in the blood in the newborn).Biliary atresia (progressive obliterative cholangiopathy): obstruction at birth due to fibrosis andatresia of the extrahepatic ducts (and so no gall bladder); then variable severity and speed ofinflammation and fibrosis of the intrahepatic system which ultimately leads to cirrhosisMost present in first 2 weeks of life with jaundice (conjugated hyperbilirubinemia), poorfeeding, vomiting, lethargy, hepatosplenomegaly, persistent acholic stools and dark urineBest initial test: U/S (triangular fibrotic cord at porta hepatis; no evidence of normal ductalanatomy; no gallbladderMost accurate test (next step): percutaneous liver biopsy (is pathognomonic for this process)Best initial treatment (palliative): hepatic portojejunostomy (Kasai procedure)Best long-term management: liver transplantLiver disease (primary or secondary to systemic disease): cholestasis (sepsis, perinatalinfections, metabolic disease, neonatal hepatitis, severe hypothyroidism and othersIntestinal transport and excretion: most bilirubin is eliminated in the stool with final productssynthesized with help of colonic bacteria; some bilirubin is eliminated in the urine, some isreprocessed in the liver due to enterohepatic circulation (along with bile acids); intestinal betaglucuronidase hydrolyzes glucuronide-bilirubin bonds to yield some unconjugated bilirubin, which isabsorbed into the portal circulation and transported back to the liver to be acted upon by hepaticglucuronyl transferaseIncreased enterohepatic circulationIntestinal obstructionDecreased colonic bacteria (first week of life, prolonged antibiotics, severe diarrhea)http://ebook2book.ir/
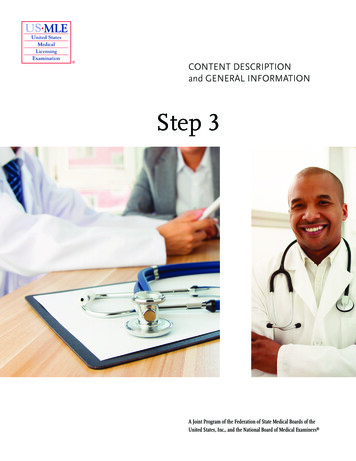
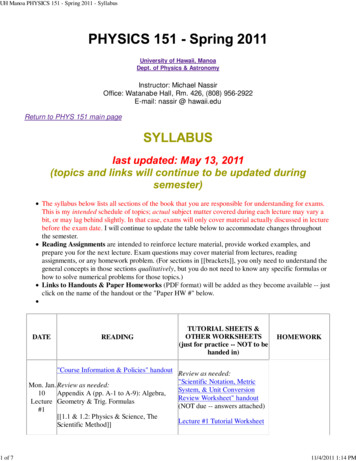
Clinical RecallWhich of the following is not a cause of hyperbilirubinemia?A)Increased red blood cell productionB)C)D)ABO incompatibilityBiliary atresiaIncreased activity of hepatic glucuronyl transferaseE)Decreased enterohepatic circulationAnswer: DBreast feeding jaundice vs. breast milk jaundice (see text box)Figure 1-2. Jaundice Workuphttp://ebook2book.ir/
BREAST-FEEDING JAUNDICE VERSUS BREAST-MILK JAUNDICEBreast-feeding jaundice means a baby is not nursing well and so not getting many calories. This is common in first-time breast-feedingmothers. The infant may become dehydrated; however, it is lack of calories that causes the jaundice. Treatment is to obtain a lactationconsultation and rehydrate the baby. The jaundice occurs in the first days of life.Breast-milk jaundice occurs due to a glucoronidase present in some breast milk. Infants become jaundiced in week 2 of life. Treatmentis phototherapy if needed. Although the bilirubin may rise again, it will not rise to the previous level. The baby may then be safely breastfed. The jaundice will be gone by 2–3 months.Treatment of hyperbilirubinemiaPhototherapyComplications: loose stools, erythematous macular rash, overheating leading to dehydration, andbronze baby syndrome (occurs with direct hyperbilirubinemia; dark, grayish-browndiscoloration of the skin [photo-induced change in porphyrins, which are present in cholestaticjaundice])Double volume exchange transfusion—if bilirubin continues to rise despite intensivephototherapy and/or kernicterus is a concernEtiologyReason forHyperbilirubinemiaincreasedHgb,Other Cs Hgbbruising/cephalohematoma BilirubinIndirectPhototherapyNormal toslightly lowHgb/HctNormal to slightincrease inreticulocytesImmune hemolysisAnti-Rh, anti-A,IndirectLow Hgb/HctRh negativePhototherapy Rhanti-B, anti-(anemia)mother andpossibleABOminor bloodIncreasedRh positiveexchangeMinor blood groupsgroup AbsreticulocytesbabytransfusionType Omother andtype A or BbabyDirectCoombshttp://ebook2book.ir/positive
DecreasedRBCsPolycythemiaHigh Hct, HgbIndirect high bilirubinHighIncreased RBCs(Hct 65)/normalPhototherapy partial exchangetransfusionNon-immune hemolysisAbnormal RBCIndirect splenicLowIf noPhototherapy (anemia)/increasedmembranetransfusiondefect ,removalG6PD, PKactivityCharacteristicRBCs ifmembranedefectDecreasedRBCsDisplacement of boundFree bilirubin inbilirubin from albumincirculationFamilial nonhemolyticAbsence jar syndrome)transferasetransfusionIndirectNormalTreat underlyingproblemIndirectNormalGT activityPhototherapy (type I) vs. smallamount ofinducible GT(type II)Extrahepatic obstructionBilirubin cannot—biliary atresialeave the biliaryDirectNormalUltrasound, liverPortojejunostomy,biopsythen later liversystemCholestasis (TORCH,Abnormalsepsis, metabolic,endocrine)Bowel obstructionBreast feeding jaundicetransplantWith H and P,Treat underlyinghepatic functionother select labsproblem decreasesuggestive tion irectNormalhttp://ebook2book.ir/Phototherapy hydration teach
recirculationBreast milk jaundiceIncreasedbreast feedingIndirectNormalPhototherapy enterohepaticcontinued breastrecirculationfeedingTable 1-7.Hyperbilirubinemia and Jaundicehttp://ebook2book.ir/
INFECTIONSNEONATAL SEPSISA 3-week-old infant presents with irritability, poor feeding, temperature of 38.9 C (102 F), andgrunting. Physical examination reveals a bulging fontanel, delayed capillary refill, and grunting.Signs and symptoms are very nonspecific.Risk factorsPrematurityChorioamnionitisIntrapartum feverProlonged rupture of membranesMost common organisms: group B Streptococcus, E. coli, and Listeria monocytogenes.http://ebook2book.ir/
NOTEIn recent years studies have proven that in the first year of life, lumbar puncture reveals almost no cases of meningitis. Therefore,lumbar puncture should be reserved only for neonates with severe signs.Diagnosis—sepsis workup: CBC, differential and platelets, blood culture, urine analysis and culture,chest x-ray; lumbar puncture only for neonates with severe signs (lethargy, hypothermia, hypotonia,poor perfusion, apnea, abnormal neurological findings, or clinical deterioration from birth)TreatmentIf no evidence of meningitis: ampicillin and aminoglycoside until 48–72-hour cultures arenegativeIf meningitis or diagnosis is possible: ampicillin and third-generation cephalosporin (notceftriaxone)http://ebook2book.ir/
TRANSPLACENTAL INTRAUTERINE INFECTIONS(TORCH)TORCH infections are typically acquired in first or second trimester. Most infants have IUGR.http://ebook2book.ir/
NOTEToxoplasmosisOther (syphilis, varicella, HIV, and parvovirus B19)RubellaCytomegalovirus (CMV)HerpesToxoplasmosisToxoplasmosis is a maternal
USMLE is a joint program of the Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME), neither of which sponsors or endorses this product. This publication is designed to provide accurate information in regard to the su