Transcription
FIRST AID Q&A FOR THEUSMLESTEP 2 CKSecond EditionSENIOR EDITORSEDITORSTAO LE, MD, MHSHERMAN SINGH BAGGA, MDAssistant Clinical ProfessorChief, Section of Allergy and Clinical ImmunologyDepartment of MedicineUniversity of LouisvilleResidentDepartment of UrologyUniversity of California, San Francisco Medical CenterKRISTEN VIERREGGER, MDResidentDepartment of DermatologyMayo ClinicResidentDepartment of PathologyUniversity of California, Irvine Medical CenterTHOMAS L.H. HOCKER, MDCHRISTOPHER R. KINSELLA, JR., MDResearch FellowUniversity of Pittsburgh Medical CenterMATTHEW O'ROURKE, MDResidentMorgan Stanley Children's Hospital of New York–PresbyterianColumbia University Medical CenterJOHN RHYNER, MDResidentDepartment of Internal MedicineUniversity of Michigan Medical CenterSADE CLARKE UDOETUK, MDResidentDepartment of PsychiatryBaylor College of MedicineNew York / Chicago / San Francisco / Lisbon / London / Madrid / Mexico CityMilan / New Delhi / San Juan / Seoul / Singapore / Sydney / Toronto
Copyright 2010, 2008 by Tao Le. All rights reserved. Except as permitted under the United States Copyright Act of 1976, no part of this publication may be reproduced or distributed in any form or by any means, or stored in a database or retrieval system, without the prior written permission of the publisher.ISBN: 978-0-07-162930-0MHID: 0-07-162930-0The material in this eBook also appears in the print version of this title: ISBN: 978-0-07-162571-5, MHID: 0-07-162571-2.All trademarks are trademarks of their respective owners. Rather than put a trademark symbol after every occurrence of a trademarked name, we use names in aneditorial fashion only, and to the benefit of the trademark owner, with no intention of infringement of the trademark. Where such designations appear in this book, theyhave been printed with initial caps.McGraw-Hill eBooks are available at special quantity discounts to use as premiums and sales promotions, or for use in corporate training programs. To contact arepresentative please e-mail us at bulksales@mcgraw-hill.com.Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authorsand the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with thestandards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher norany other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate orcomplete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers areencouraged to confirm the information contained herein with other sources. For example and in particular, readers are advised to check the product information sheetincluded in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been madein the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently useddrugs.TERMS OF USEThis is a copyrighted work and The McGraw-Hill Companies, Inc. (“McGraw-Hill”) and its licensors reserve all rights in and to the work. Use of this work is subject tothese terms. Except as permitted under the Copyright Act of 1976 and the right to store and retrieve one copy of the work, you may not decompile, disassemble, reverseengineer, reproduce, modify, create derivative works based upon, transmit, distribute, disseminate, sell, publish or sublicense the work or any part of it without McGrawHill’s prior consent. You may use the work for your own noncommercial and personal use; any other use of the work is strictly prohibited. Your right to use the work maybe terminated if you fail to comply with these terms.THE WORK IS PROVIDED “AS IS.” McGRAW-HILL AND ITS LICENSORS MAKE NO GUARANTEES OR WARRANTIES AS TO THE ACCURACY, ADEQUACY OR COMPLETENESS OF OR RESULTS TO BE OBTAINED FROM USING THE WORK, INCLUDING ANY INFORMATION THAT CAN BE ACCESSEDTHROUGH THE WORK VIA HYPERLINK OR OTHERWISE, AND EXPRESSLY DISCLAIM ANY WARRANTY, EXPRESS OR IMPLIED, INCLUDING BUTNOT LIMITED TO IMPLIED WARRANTIES OF MERCHANTABILITY OR FITNESS FOR A PARTICULAR PURPOSE. McGraw-Hill and its licensors do notwarrant or guarantee that the functions contained in the work will meet your requirements or that its operation will be uninterrupted or error free. Neither McGraw-Hillnor its licensors shall be liable to you or anyone else for any inaccuracy, error or omission, regardless of cause, in the work or for any damages resulting therefrom.McGraw-Hill has no responsibility for the content of any information accessed through the work. Under no circumstances shall McGraw-Hill and/or its licensors be liablefor any indirect, incidental, special, punitive, consequential or similar damages that result from the use of or inability to use the work, even if any of them has been advisedof the possibility of such damages. This limitation of liability shall apply to any claim or cause whatsoever whether such claim or cause arises in contract, tort orotherwise.
D E D I C AT I O NTo the contributors to this and future editions, who took time to share theirknowledge, insight, and humor for the benefit of residents and clinicians.andTo our families, friends, and loved ones, who supported us in the task ofassembling this guide.
This page intentionally left blank
CONTENTSAuthorsviiFaculty ReviewersixPrefacexiAcknowledgmentsxiiiHow to ContributexvS EC T IO N IO R G A N SYST E M S1Chapter 1CardiovascularChapter 2Dermatology47Chapter 3Endocrinology57Chapter 4Epidemiology and Preventive Medicine91Chapter 5Ethics and Legal Issues117Chapter 6Gastrointestinal127Chapter 7Hematology/Oncology167Chapter 8Infectious Disease211Chapter 9Musculoskeletal261Chapter 10Neurology285Chapter 11Obstetrics321Chapter 12Gynecology351Chapter 13Psychiatry375Chapter 14Pulmonary409Chapter 15Renal/Genitourinary441S EC T IO N I IF U LL-LE N G T H E X A M I NAT I O N S3471Test Block 1473Test Block 2507Test Block 3539v
Test Block 4573Test Block 5607Test Block 6641Test Block 7675Test Block 8709About the Authors743vi
AUTHORSCYNTHIA ADAMS, MDLAURA MEINTSResidentBoston Combined Residency Program in PediatricsChildren's Hospital BostonVanderbilt University School of MedicineClass of 2009CLARISSA BARNES, MDResidentDepartment of Internal MedicineJohns Hopkins University School of MedicineRACHEL BORTNICK, MPHILMedical Scientist Training ProgramHarvard Medical SchoolCHRISTOPHER CHAPMAN, MDResidentDepartment of Internal MedicineUniversity of Chicago Medical CenterLIA CLATTENBURG, MD, MPHResidentDepartment of Internal MedicineUnion Memorial HospitalBaltimore, Md.GILLIAN DIERCKSColumbia University College of Physicians and SurgeonsClass of 2009VAHID ENTEZARI, MDPostdoctoral Research FellowOrthopedic Biomechanics LaboratoryBeth Israel Deaconess Medical CenterJOHNATHAN ETHRIDGEJohns Hopkins University School of MedicineClass of 2009ROBERT MICHELETTI, MDResidentDepartments of Internal Medicine and DermatologyHospital of the University of PennsylvaniaDANIEL L. MILLERJohns Hopkins University School of MedicineClass of 2009Johns Hopkins Bloomberg School of Public HealthClass of 2009DEEPIKA NEMANIUniversity of Pennsylvania School of MedicineClass of 2009TIMOTHY NIESSENJohns Hopkins University School of MedicineClass of 2009Johns Hopkins Bloomberg School of Public HealthClass of 2009HOWARD O'ROURKE, MDResidentDepartment of Diagnostic RadiologyUniversity of Pittsburgh Medical CenterNISHANT PATELJohns Hopkins University School of MedicineClass of 2009ROHITH PIYARATNA, MDERICA Y. FANResidentDepartment of AnesthesiologyStanford University Medical CenterSt. Louis University School of MedicineClass of 2009ANTHONY PRINCE, MDCARL ERIK FISHERResidentDepartment of OtolaryngologyMount Sinai Medical CenterColumbia University College of Physicians and SurgeonsClass of 2009SATTAR GOJRATY, MDFIORELLA SAPONARA, MDResidentDepartment of Internal MedicineHospital of the University of PennsylvaniaResidentTransitional ProgramMaimonides Medical CenterNew York CityNILAY KAVATHIA, MDASHA JAYENDRAKUMAR SHAH, MDResidentDepartment of Internal MedicineThomas Jefferson University HospitalInternDepartment of Internal MedicineEmory University School of Medicinevii
MONICA E. SHUKLABRANT W. ULLERY, MDVanderbilt University School of MedicineClass of 2009ResidentDepartment of SurgeryHospital of the University of PennsylvaniaMEGHAN SISEColumbia University College of Physicians and SurgeonsClass of 2009D'MITRI SOFIANOS, MDResidentDepartment of Orthopedic SurgeryUniversity of Utah Medical CenterANNA E. TEETERDuke University School of MedicineClass of 2009JOSHUA D. UDOETUK, MDKELLY VRANAS, MDResidentDepartment of Internal MedicineHospital of the University of PennsylvaniaDAVID WEIColumbia University College of Physicians and SurgeonsClass of 2009ZACHARY ZAVODNIDuke University School of MedicineClass of 2009Transitional InternUniversity of Texas-Houston Medical SchoolASSOCIATE AUTHORSMARINA FRIMER, MDSUNIL SHETHResidentDepartment of Obstetrics and Gynecology and Women's HealthAlbert Einstein College of MedicineHarvard Medical SchoolClass of 2009MARK J. MANN, MDResidentDepartment of UrologyState University of New York Upstate Medical UniversitySyracuse, N.Y.PARIN J. PATEL, MDResidentDepartment of Internal MedicineHospital of the University of PennsylvaniaviiiviiiLEANNE STANLEYDuke University School of MedicineClass of 2009TIAN ZHANGHarvard Medical SchoolClass of 2009
FACULTY REVIEWERSJONATHAN W. BRESS, MDKERILYN MORGAN, MDNephrologistPhiladelphia Hypertension & Nephrology ConsultantsRACHEL CHONG, MDAssociate Program DirectorDepartment of Internal MedicineBanner Good Samaritan Medical CenterPhoenix, Ariz.EndocrinologistLakeridge Health CorporationRINI BANERJEE RATAN, MDPETER DANYI, MD, MPH, MBAAssistant Clinical ProfessorDepartment of Obstetrics and GynecologyColumbia University College of Physicians & SurgeonsInstructor, Hospitalist ProgramDivision of General Internal MedicineJohns Hopkins University School of MedicineROBIN GIRDHAR, MDVice Chairperson and Director of Quality AssuranceDivision of CardiologyShadyside HospitalUniversity of Pittsburgh School of MedicineANDREW J. LENNEMAN, MDClinical FellowCardiovascular Medicine DivisionVanderbilt University School of MedicineESTER C. LITTLE, MDAssociate DirectorBanner Liver Disease CenterClinical Assistant Professor of MedicineUniversity of Arizona College of MedicineMARCUS A. MCFERREN, MD, PHDDepartment of DermatologyYale-New Haven HospitalELIZABETH SASTRE, MDAssistant ProfessorVanderbilt University Medical CenterAttending PhysicianMedical Service, Primary CareTennessee Valley Healthcare Veteran’s Administration HospitalJERRY D. SMILACK, MDEmeritus Associate Professor of MedicineMayo College of MedicineRetired ConsultantDepartment of Internal MedicineMayo ClinicMYRA J. WICK, MD, PHDDepartment of Medical GeneticsMayo ClinicAPRIL ZHU, MDThe Permanente Medical GroupSanta Clara, Calif.ix
This page intentionally left blank
PREFACEWith First Aid Q&A for the USMLE Step 2 CK, we continue our commitment to providing students with the most useful and up-to-date preparationguides for the USMLE Step 2 CK. This addition to the First Aid series represents an outstanding effort by a talented group of authors and includes the following:䡲䡲䡲䡲䡲䡲1,000 high-yield USMLE-style questions based on the top-ratedUSMLERx Qmax Step 2 CK Test Bank (www.usmlerx.com)Concise yet complete explanations to correct and incorrect answersOrganized as a perfect complement to First Aid for the USMLE Step 2 CKEight full-length test blocks simulate the actual exam experienceHigh-yield images, diagrams, and tables complement the questions andanswersTimely updates and corrections at www.firstaidteam.comWe invite you to share your thoughts and ideas to help us improve First AidQ&A for the USMLE Step 2 CK. See How to Contribute, p. xv.LouisvilleIrvineTao LeKristen Vierreggerxi
This page intentionally left blank
ACKNOWLEDGMENTSThis has been a collaborative project from the start. We gratefully acknowledge the thoughtful comments and advice of the medical students, residents,international medical graduates, and faculty who have supported the authorsin the development of First Aid Q&A for the USMLE Step 2 CK.Additional thanks to Neil Busis and Hey Chong for their review of the manuscript.For support and encouragement throughout the process, we are grateful toThao Pham, Selina Franklin, Louise Petersen, Jonathan Kirsch, and VikasBhushan. Thanks to our publisher, McGraw-Hill, for the valuable assistanceof their staff. For enthusiasm, support, and commitment to this challengingproject, thanks to our editor, Catherine Johnson. For outstanding editorialwork, we thank Steve Freedkin, Isabel Nogueira, and Emma D. Underdown.A special thanks to Rainbow Graphics for remarkable production work.For contributions, corrections, and surveys we thank Juan F. Alvarez, M.R.Brenz, Ericka Li Fuentes, Katherine Kline, Solomon Onyenkachukwu, Matthew Swenson, and Jennifer Turley.LouisvilleIrvineTao LeKristen Vierreggerxiii
This page intentionally left blank
HOW TO CONTRIBUTETo continue to produce a high-yield review source for the USMLE Step 2 CK exam, we invite you tosubmit any suggestions or corrections. We also offer paid internships in medical education and publishing ranging from three months to one year (see below). Please send us your suggestions for䡲䡲䡲Corrections or enhancements to existing questions and explanationsNew high-yield questionsLow-yield questions to removeFor each entry incorporated into the next edition, you will receive a 10 gift certificate, as well as personal acknowledgment in the next edition. Diagrams, tables, partial entries, updates, corrections, andstudy hints are also appreciated, and significant contributions will be compensated at the discretion ofthe authors.The preferred way to submit entries, suggestions, or corrections is via our blog at:www.firstaidteam.comOtherwise, please send entries, neatly written or typed or on disk (Microsoft Word), to:First Aid Q&A for the USMLE Step 2 CK , Second Edition914 North Dixie Avenue, Suite 100Elizabethtown, KY 42701All entries become property of the authors and are subject to editing and reviewing. Please verify all dataand spellings carefully. In the event that similar or duplicate entries are received, only the first entry received will be used. Include a reference to a standard textbook to facilitate verification of the fact. Pleasefollow the style, punctuation, and format of this edition if possible.I N T E R N S H I P O P P O RT U N I T I E SThe First Aid Team is pleased to offer part-time and full-time paid internships in medical education andpublishing to motivated medical students and physicians. Internships may range from three months (e.g., asummer) up to a full year. Participants will have an opportunity to author, edit, and earn academic credit ona wide variety of projects, including the popular First Aid and USMLERx series. Writing/editing experience, familiarity with Microsoft Word, and Internet access are desired. For more information, submit a résumé or a short description of your experience along with a cover letter to firstaidteam@yahoo.com.xv
This page intentionally left blank
SECTION IOrgan Systems䉴 Cardiovascular䉴 Dermatology䉴 Endocrinology䉴 Epidemiology andPreventive Medicine䉴 Ethics and Legal Issues䉴 Gastrointestinal䉴 Hematology/Oncology䉴 Infectious Disease䉴 Musculoskeletal䉴 Neurology䉴 Obstetrics䉴 Gynecology䉴 Psychiatry䉴 Pulmonary䉴 Renal/Genitourinary1
This page intentionally left blank
CHAPTER 1Cardiovascular3
HIGH-YIELD SYSTEMSCardiovascular4Section I: Organ Systems QuestionsQ U E ST I O N S1. A 66-year-old retired carpenter presents withchronic shortness of breath upon exertion. Hehas smoked one pack of cigarettes per day forthe past 5 years and drinks alcohol regularly.Physical examination reveals a displaced pointof maximal impulse and hepatosplenomegaly.His medications include pantoprazole for gastroesophageal reflux and sertraline for depression. Echocardiogram reveals an ejection fraction of 30% and dilated left and right ventricles.Laboratory tests show:Na : 129 mEq/LK : 5.2 mEq/LCl : 101 mEq/LBlood urea nitrogen: 45 mg/dLCreatinine: 1.3 mg/dLGlucose: 134 mg/dLAspartate aminotransferase: 220 U/LAlanine aminotransferase: 140 U/LAlkaline phosphatase: 280 U/LWhich of the following is the most likely causeof his cardiac findings?(A) Borrelia burgdorferi(B) Cigarette smoking(C) Coxsackie B virus(D) Ethanol(E) Pantoprazole toxicity(F) Trypanosoma cruzi2. A 52-year-old man presents to his primary carephysician’s office for routine care. He has hypertension, hypercholesterolemia, and type 2diabetes mellitus, and has smoked one pack ofcigarettes per day for the past 30 years. Medications include hydrochlorothiazide, atorvastatin,and glipizide. There is a family history of myocardial infarction in the maternal grandfatherat age 60. The patient has undergone screening for colon and prostate cancer. Physical examination reveals a pleasant, obese man who is175 cm (5′ 9″) tall and weighs 108 kg (238 lb).His blood pressure is 155/81 mm Hg, heart rateis 78/min, respiratory rate is 14/min, and temperature is 36.8 C (98.3 F). What one actionwould most reduce the patient’s stroke risk?(A) Blood glucose reduction(B) Blood pressure reduction(C) Serum cholesterol reduction(D) Smoking cessation(E) Weight loss3. A 36-year-old man presents to the clinic withcomplaints of a genital sore. The patient is asexually active heterosexual involved withthree partners and practices unprotected intercourse. Fours days ago he noted a painless soreon his penis. He is afebrile, with a heart rate of80/min and blood pressure of 120/77 mm Hg.Physical examination reveals a solitary ulcerated lesion located on the lateral aspect of hispenis. The lesion is nontender and associatedwith bilateral inguinal lymphadenopathy. Physical examination is otherwise normal. If leftuntreated, this man is at increased risk forwhich of the following?(A) Ascending aortic aneurysm(B) Coronary artery aneurysm(C) Endocarditis(D) Mitral valve stenosis(E) Rupture of ventricular free wall4. An 81-year-old man is hospitalized for acuteonset of shortness of breath and lower extremity edema. Although he lives by himself, it isvery difficult for him to move around his apartment without experiencing fatigue. He has notseen his physician in years but was told in thepast that he had high blood pressure. On physical examination his jugular venous pulse is palpated 9 cm above his sternal notch, inspiratorycrackles are heard at his lung bases, and thereis 3 lower extremity edema. Which of the following will confirm the most likely diagnosis?(A) Cardiac angiography(B) Echocardiography(C) Electrocardiogram(D) Endomyocardial biopsy(E) Pulmonary function tests(F) X-ray of the chest
55. A 42-year-old man presents to the clinic forroutine evaluation. His medical history is significant for gallstones. The patient deniessmoking and drinks alcohol occasionally. Hismother had a heart attack at the age of 63years. His blood pressure is 134/77 mm Hg.The patient is overweight with well-healed laparoscopic cholecystectomy scars. Fasting laboratory tests show:What is the most appropriate next step in management?(A) A trial of lifestyle modification alone (diet,exercise, and weight loss)(B) A trial of lifestyle modification combinedwith statin and niacin therapy(C) A trial of lifestyle modification combinedwith statin therapy(D) Niacin therapy(E) Statin therapy6. Two and a half weeks after coronary artery bypass grafting, a 63-year-old man returns to theemergency department acutely short of breath.The patient states that he began having chestpain and shortness of breath approximately 1hour earlier. He has a history of hypertension,diabetes, and two myocardial infarctions. Onexamination he is hypoxic with an oxygen saturation of 86% on room air. Other vital signsand results of a physical examination are normal. ECG shows no interval change from hismost recent ECG. CT of the chest is shown inthe image. What is the most likely etiology ofthis patient’s shortness of breath?Reproduced, with permission, from PEIR Digital Library(http://peir.net).(A) Aortic dissection(B) Exacerbation of chronic obstructive pulmonary disease(C) Myocardial infarction(D) Pleural effusion(E) Pulmonary embolus7. A 72-year-old man with coronary artery diseaseand hypertension is hospitalized after sufferinga myocardial infarction 5 days ago. He suddenly complains of severe chest pain. Hisblood pressure is 90/60 mm Hg and heart rateis 65/min. Auscultation reveals no murmurs orrubs. An ECG reveals sinus rhythm with anacute ST-segment elevation in the anteroseptalarea. Urgent bedside echocardiography showedanteroseptal, lateral, and apical akinesis, mildleft ventricular systolic dysfunction, and severepericardial effusion. Within 20 minutes he isunconscious with undetectable pulses andblood pressure. What is the most likely causeof the patient’s sudden decompensation?(A) Free wall rupture(B) Left ventricular thrombus(C) Mitral regurgitation(D) Pericarditis(E) Ventricular septal ruptureCardiovascularAspartate aminotransferase: 37 U/LAlanine aminotransferase: 28 U/LAlkaline phosphatase: 88 U/LTotal cholesterol: 268 mg/dLLDL cholesterol: 183 mg/dLHDL cholesterol: 46 mg/dLTriglycerides: 166 mg/dLHIGH-YIELD SYSTEMSChapter 1: Cardiovascular Questions
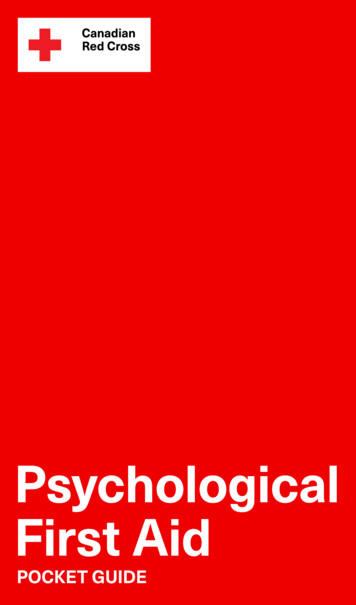
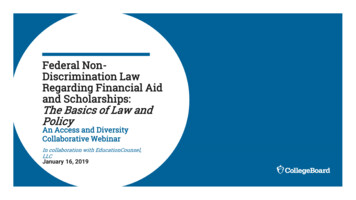
HIGH-YIELD SYSTEMSCardiovascular6Section I: Organ Systems Questions8. A 56-year-old woman was recently started onmedication for high blood pressure. At her nextoffice visit her hypertension is under good control, but she now complains of “feeling strange”since she started the medication. On furtherquestioning, she reports feeling chest tightnessseveral times over the past 2 weeks, and hasalso noticed pain in her elbows and knees. Herblood pressure is 124/78 mm Hg (146/82 mmHg on last visit), heart rate is 102/min, and respiratory rate is 14/min. Her examination is notable for several erythematous plaques on themalar distribution of the face, arms, and uppertorso. What medication was she most likelystarted on during her last visit?(A) Captopril(B) Furosemide(C) Hydralazine(D) Metoprolol(E) Verapamil9. A 19-year-old woman was attacked while coming home from a party and is brought to theemergency department. She recalls beingpunched in the side of the head and stabbed inthe left flank. Her speech is slow and she complains of a bad headache. Her pulse is 110/min, blood pressure is 90/50 mm Hg, and respiratory rate is 25/min. On examination shehas a stab wound at the left costal margin inthe midaxillary line. Two large-bore intravenous lines are inserted, and after infusion of2 L of lactated Ringer’s solution her bloodpressure rises to 95/55 mm Hg. What is themost appropriate next step in management?(A) Abdominal ultrasound(B) Diagnostic peritoneal lavage(C) Exploratory laparotomy(D) Noncontrast CT of the head(E) Peritoneal laparoscopy10. A 48-year-old man presents to the emergencydepartment complaining of crushing substernal chest pain. He is diaphoretic, anxious, anddyspneic. His pulse is 110/min, blood pressureis 175/112 mm Hg, respiratory rate is 30/min,and oxygen saturation is 94%. Aspirin, oxygen,sublingual nitroglycerin, and morphine aregiven, but they do not relieve his pain. ECGshows ST-segment elevation in leads V2 to V4.The duration of symptoms is now approximately 30 minutes. What is the most appropriate treatment for this patient at this time?(A) Calcium channel blocker(B) Intravenous angiotensin-converting enzyme inhibitor(C) Intravenous β-blocker(D) Magnesium sulfate(E) Tissue plasminogen activator11. A 70-year-old woman presents to the emergency department complaining of dizziness.She is disoriented to the date and her locationand it is difficult to gather an accurate history.Her pulse is 48/min, blood pressure is 84/60mm Hg, and respiratory rate is 12/min. Onexamination her extremities are cool andclammy. Her capillary refill time is 5 seconds.What is the most appropriate therapy?(A) Adenosine(B) Amiodarone(C) Atropine(D) Isoproterenol(E) Metoprolol12. A 77-year-old man, complaining of abdominalpain, anorexia, and nausea and vomiting overthe past 24 hours, presents to the clinic withhis son. The son reveals that his father has alsocomplained of blurred vision. The patient’s vital signs are stable and his abdomen is soft, buthe appears to be somewhat confused. He iscurrently taking metoprolol, digoxin, and hydrochlorothiazide for ischemic congestiveheart failure. His son says that sometimes hisfather confuses his medications. The patientalso has renal insufficiency with a baseline serum creatinine of 2.6 mg/dL. The ECG revealsa widened QRS complex and a new first-degreeheart block. Which of the following is the mostlikely cause of this patient’s symptoms?(A) Digoxin toxicity(B) Gastroenteritis(C) Hypocalcemia(D) Hypovolemia secondary to thiazide diuretic overuse(E) Myocardial infarction
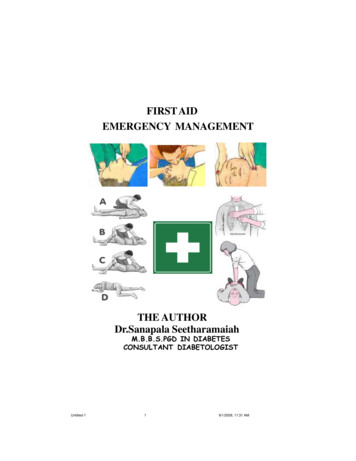
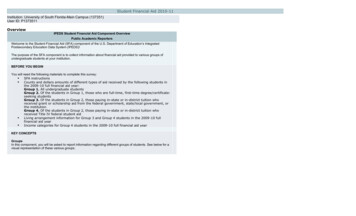
(A) Borrelia burgdorferi infection(B) Deletion mutation in dystrophin(C) Frameshift mutation in dystrophin(D) Trinucleotide repeat expansion(E) X-linked emerin deficiency14. A college sophomore is found by his roommateto be poorly responsive and brought to theemergency department. After resuscitation, theman complains of a severe headache and photophobia that is accompanied by dizziness,nausea, vomiting, and neck pain. Physical examination is noteworthy for positive Kernig’sand Brudzinski’s signs as well as petechiae onthe trunk and mucocutaneous bleeding. Laboratory studies show:WBC count: 17,000/mm³Hemoglobin: 11 g/dLPlatelet count: 70,000/mm³Bleeding time: 10 minProthrombin time: 17 secActivated partial thromboplastin time: 47 secThrombin time: 18 secA peripheral blood smear is shown in the image. Which of the following is the most likelydiagnosis?Reproduced, with permission, from Lichtman MA, Beutler E,Kipps TJ, Seligsohn U, Kaushansky K, Prchal JT. Williams’Hematology, 7th edition. New York: McGraw-Hill, 2006: PlateIII-2.(A) Disseminated intravascular coagulation(B) Factor V Leiden(C) Immune thrombocytopenic purpura(D) Protein C deficiency(E) Thrombotic thrombocytopenic purpura15. A 60-year-old man with coronary artery disease,peptic ulcer disease, and gout presents to theemergency department with a 24-hour historyof abdominal pain. The pain, which is most intense in the upper abdomen, was sudden inonset and has become progressively more severe. Free air in the abdomen is detected onx-ray films. The patient is in an agitated state.His extremities are cool and capillary refilltime is 3 seconds. His blood pressure is 80/40mm Hg and heart rate is 130/min. The neckveins are flat and the lungs are clear to auscultation. His hemoglobin is 13.8 g/dL. A urinarycatheter is inserted and 10 mL of urine isdrained. What is the most appropriate treatment for this patient at this time?(A) Broad-spectrum antibiotics for presumedsepsis(B) Infusion of isotonic fluid(C) Infusion of norepinephrine(D) Inotropic support with dopamine, vasopressin, or dobutamine(E) Transfuse with 1 unit packed RBCsCardiovascular13. A 35-year-old woman presents to the clinic because of visual problems. She states that shehas always had difficulty looking up, and overthe past few years her overall vision has become blurry. Review of symptoms is notablefor several recent episodes of “near fainting.”She takes no medication and has no othermedical history, and has not seen a physicianfor 7 years. Because she was adopted as a child,she does not know her family history, but herson has required special tutoring at school. Thepatient also remarks that her son seems to havebeen dropping objects lately. Physical examination reveals bilateral ptosis. Her extraocularmovements are intact and the pupils are equal,round, and reactive. Her corrected visual acuity is 20/100 in the right eye and 20/120 in theleft eye. The view of the fundus is obscured.On ambulation she raises her knees and makesa slapping sound on the floor as she walks.ECG indicates heart block. What is the pathogenesis of this patient’s disorder?7HIGH-YIELD SYSTEMSChapter 1: Cardiovascular Questions
HIGH-YIELD SYSTEMSCardiovascular8Section I: Organ Systems Questions16. A 29-year-old woman presents to the emergency department with a 3-week history of being awakened by a dull, prolonged chest painthat occurs 3–4 times a week. She is a smokerbut has never suffered a myocardial infarction(MI) or had chest pain before and has no family history of early MI. Results of a 12-leadECG are normal. Her first set of cardiac enzyme measurements (creatine kinase, creatinekinase-MB fraction, troponin I) are negative. Ifcoronary angiography were taken at the time ofher chest pain, which of the following findingsis most like?(A) Coronary artery spasm(B) Greater than 80% stenosis in at least twocoronary arteries(C) No abnormal findings(D) Plaque rupture and thrombosis17. A 42-year-old man presents to the emergencydepartment with a complaint of increasingshortness of breath when walking to get hisnewspaper, difficulty breathing while lying flat,and a 4.5-kg (10-lb) weight gain over the pastmonth. He is afebrile, his pulse is 75/min, andhis blood pressure is 98/50 mm Hg. On examination he smells of alcohol and has 2 pittingedema in the lower extremities and a thirdheart sound. X-ray of the chest reveals cardiomegaly. What additional findings must be present to confirm this man’s underlying diagnosis?(A) Hepatojugular reflux and pulmonary congestion
guides for the USMLE Step 2 CK. This addition to the First Aid series repre-sents an outstanding effort by a talented group of authors and includes the fol-lowing: 1,000 high-yield USMLE-style questions based on the top-rated USMLERx Qmax Step 2 CK Test Bank (www.usmlerx.com) Concise yet complete explanations to correct and incorrect answers