Transcription
Au et al. BMC International Health and Human 19) 19:22RESEARCH ARTICLEOpen AccessA model explaining refugee experiences ofthe Australian healthcare system: asystematic review of refugee perceptionsMichael Au1* , Athire Debbie Anandakumar1, Robyn Preston1,2, Robin A. Ray1 and Meg Davis3AbstractBackground: Refugees have significant unmet health needs. Delivering services to refugees continues to beproblematic in the Australian healthcare system. A systematic review and thematic synthesis of the literatureexploring refugee perceptions of the Australian healthcare system was performed.Methods: Titles and abstracts of 1610 articles published between 2006 and 2019 were screened, and 147 articleswere read in full text. Depending on the type of study, articles were appraised using the Modified Critical AppraisalTool (developed by authors), the Mixed Methods Appraisal Tool, or the JBI Appraisal Checklist for SystematicReviews. Using QSR NVivo 11, articles were coded into descriptive themes and synthesised into analytical themes.An explanatory model was used to synthesise these findings. Confidence in the review findings were assessed withGRADE-CERQual approach.Results: The final synthesis included 35 articles consisting of one systematic review, 7 mixed methods studies, and27 qualitative studies. Only one study was from a regional or rural area. A model incorporating aspects ofengagement, access, trust, and privacy can be used to explain the experiences of refugees in using the Australianhealthcare system. Refugees struggled to engage with health services due to their unfamiliarity with the healthsystem. Information sharing is needed but this is not always delivered effectively, resulting in disempowerment andloss of autonomy. In response, refugees resorted to familiar means, such as family members and their pre-existingcultural knowledge. At times, this perpetuated their unfamiliarity with the broader health system. Access barrierswere also encountered. Trust and privacy are pervasive issues that influenced access and engagement.Conclusions: Refugees face significant barriers in accessing and engaging with healthcare services and oftenresorted to familiar means to overcome what is unfamiliar. This has implications across all areas of service provision.Health administrators and educators need to consider improving the cultural competency of staff and students.Policymakers need to consider engaging communities and upscale the availability and accessibility of professionallanguage and cultural supports. Research is needed on how these measures can be effectively delivered. There islimited research in remote areas and further evidence is needed in these settings.Keywords: Refugees, Perception, Access, Engagement, Qualitative, Health services, Trust, Power, Health information,Autonomy, Cultural competency, Public health* Correspondence: michael.au@my.jcu.edu.au1College of Medicine and Dentistry, James Cook University, Townsville,Queensland, AustraliaFull list of author information is available at the end of the article The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication o/1.0/) applies to the data made available in this article, unless otherwise stated.
(2019) 19:22Page 2 of 23BackgroundRefugees in Australia are consistently recognised as anunderserved population with higher rates of mentalhealth and infectious diseases [1–3]. This is compounded by pre-arrival and post-arrival factors includingpoor care in their country of origin, trauma, prolongeddetention, and barriers to appropriate care on arrival [4].Seeking refugee status in Australia is tightly controlled.In the year 2016–2017, 21,968 visas were granted underthe Refugee and Humanitarian Assistance Programmeincluding 8208 places for displaced Syrian and Iraqirefugees. Those who arrive in Australia without a visaare subject to mandatory detention [5]. The evidence indicates a clear detrimental effect of indefinite detention,especially on mental health, and the morbidity is transferred into settlement [6–9]. Given these health issues,most States or Territories have their own policies withdifferent targets and objectives towards improvingrefugee health [10–12]. However, to date, there is still nocoordinated national policy.Once in the community, refugees have access to Medicare Benefit Schedule item numbers that allows a general practitioner to complete a refugee health assessmentwithin the first 12 months [13]. Refugees are also linkedwith resettlement agencies that provide some assistancein navigating the health system for six to 18 monthsupon arrival [14]. These services shape refugees’ initialexperiences with the healthcare system.Current literature exploring some of the challengesand facilitators faced by health professionals in delivering primary healthcare for refugees and asylum seekersin high-income countries can be conceptualised intothree broad themes: the healthcare encounter, workingwithin the healthcare system, and asylum and resettlement [15]. However, research is needed to understandthe experiences of refugees as an integral part of aframework to provide effective solutions to address thesebarriers. Furthermore, studies that collectively grouphigh-income countries together do not adequatelyaddress the unique geographical profile, health systemcharacteristics and social profile of Australia. These allplay a role in health, particularly, rural and remoteness.This is of significance as there have been efforts madeby the Australian Government to resettle refugees inregional areas [16].From the best available knowledge, no other systematic review has examined refugee perceptions of usingAustralian healthcare services. A scoping review of refugee perceptions in their host country only included twoAustralian studies with other international data [17]. Asimilar review examined refugee experiences of generalpractice in their countries of resettlement. However, thearticle was restricted to general practice [18]. Otherprimary research have considered refugee experiences ofhealthcare services but this is often limited to one particular service or setting [19, 20]. Examining the experiences of Australian refugees may be beneficial in aninternational context for nations that resettle refugees inregional and remote areas as well as those countries thatoffer universal primary healthcare. Considering thecurrent state of the literature, the aim of this study wasto explore the perceptions of refugees in using Australian healthcare services. Articles published from 2006 to2019 were selected to capture the current refugee demographics that occurred post-Iraq and Afghanistanconflicts. It also reflects Australia’s most recent refugeeintake after the end of the Pacific Solution policy in2007.Au et al. BMC International Health and Human RightsMethodsProtocol and registrationThis review adopted a thematic synthesis approach andadhered to ENTREQ and PRISMA guidelines [21–23].The review was registered with PROSPERO (registrationnumber: CRD42018088364).Eligibility criteriaTime frame: Studies published between the years 2006 to2019 were included to capture Australia’s most recentrefugee demographics after the Iraq and Afghanistanconflicts.Population: Refugees in Australia. Asylum seekers,immigrants, migrants, and displaced persons wereexcluded. Studies that had refugees as part of aheterogenous population were included if it clearlystated that some participants were refugees.Language: English language only.Intervention: Articles had to relate to refugee interaction with a specific health service or health intervention. Health seeking behaviours or service utilisationwere insufficient to judge perceptions of using a healthservice and therefore excluded.Outcomes: Data related to the perception of refugeesusing health services. Studies that included the perceptions of refugees and health service providers were considered but only data relating to refugees were reviewed.Types of articles: Qualitative, quantitative, mixedmethods, systematic reviews, and grey literature were included. Letters, commentaries and case studies wereexcluded. For systematic reviews, only the findings fromstudies relating to refugees were considered.Information sourcesStudies were identified through electronic databases including Scopus, CINHAL, PubMed, MEDLINE, Cochrane,and Informit. Hand searching was also used to select studies. Geographical limits to Australia were applied to all the
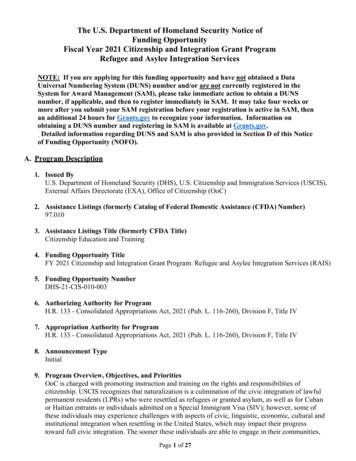
(2019) 19:22Page 3 of 23databases where available. The last search was ran on the2nd of April 2019.Duplicates were first removed, and articles publishedoutside 2006 to 2019 were excluded. Two researchers(MA and AA) independently screened the articles, firstby title, then abstract. Full text articles were screened.One author had to be contacted to retrieve full text. Ateach stage of the process, eligibility was negotiated byconsensus. When consensus was not met, a thirdresearcher (RP) was involved to decide its selection.Qualitative Research, Critical Appraisal Skills ProgrammeQualitative Appraisal Checklists, and McMaster University Critical Review Form, in order to capture the breadthand depth of assessment made by different tools (Additional file 1) [27]. The tool assessed for theoretical congruity, fundamentals, credibility, dependability, reporting,and utility. Reporting was assessed using Standards forReporting Qualitative Research. The MCAT was notassigned a scoring system and a judgment was applied toeach component.The Mixed Methods Appraisal Tool (MMAT) wasused for quantitative and mixed methods studies. Thequalitative component of mixed methods studies wereadditionally appraised with the MCAT. Systematicreviews were appraised with the JBI Appraisal Checklistfor Systematic Reviews. Consistency across tools wasmaintained as judgments were applied on componentsrather than assigning scores or grades. Two researchers(MA and AA) independently appraised the articles andconsensus was met on all the articles.Data collection process, data items, and analysisAssessment of confidence in the review findingsTwo researchers (MA and AA) were involved in the dataextraction process using QSR NVivo 11 software. Coding was regularly reviewed by authors to improve intercoder reliability. Disagreements were resolved throughconsensus. For studies that had a heterogenous population involving participants other than just refugees, onlythe data that was related to refugees was coded. Whereit was not clear to assessors if certain data related torefugees, data was included for analysis, but this affectedits appraisal performance and the confidence in thereview findings.Both first order and second order constructs wereincluded in the extraction process to capture the author’s interpretation [24, 25]. Line-by-line coding relating to refugee perceptions developed thedescriptive themes [21]. All authors interpreted thedescriptive themes to develop the analytical themesthat went beyond the primary studies. An interpretative approach was taken on the collective data whilstensuring the author’s original interpretation was captured in individual studies [26].Two researchers (MA and AA) also independentlyextracted the study characteristics including the aim,methodologies used, study setting, number of refugeeparticipants, gender of participants, country of origin,and services explored.The Confidence in the Evidence from Reviews of Qualitative research (GRADE-CERQual) method was used toassess the confidence of review findings despite thereview included quantitative, mixed methods and othersystematic reviews. Fidelity to the GRADE-CERQual approach was maintained by adhering to definitions andusing the four categories of grading. However, theauthors acknowledge potential for this to distort thefindings, which GRADE-CERQual assessment cannotassess. However, given the small number of these articles, the degree of alteration is minimal. Two researchers(MA and AA) performed this assessment under thesupervision of other authors. Disagreements wereresolved through consensus.Au et al. BMC International Health and Human RightsSearchThe search strategy is presented in Additional file 2.Maintaining close adherence to the search terms formultiple databases was ensured. As there is some variability in the definition of refugees, asylum seekers, migrants, and immigrants, all these terms were included inthe search strategy to avoid any missed articles.Study selectionAppraisal of articlesGiven the lack of consensus over a standardised qualitative appraisal tool, a Modified Critical Appraisal Tool(MCAT) was developed using components of JoannaBriggs Institute (JBI) Critical Appraisal Checklist forResultsStudy selectionA total of 35 studies were included comprising of onesystematic review, seven mixed methods studies, and 27qualitative studies (see Fig. 1).The initial search strategy generated 3349 articles withan additional seven articles identified from the referencelists of included articles. A total of 147 articles were readin full text excluding a further 112 articles.Study characteristicsStudy characteristics and results of individual studies aredetailed in Table 1.Methods and study designStudies selected in this review were published between2006 and 2019. Twenty-two studies used semi-structured
(2019) 19:22Page 4 of 23or in-depth interviews [19, 20, 29, 30, 34, 35, 37–39, 42–46, 50, 52, 54, 55, 57–60]. Focus groups with refugeeswere used in 12 studies [28, 31, 33, 38, 41, 43, 44, 47–50,53] and only 11 studies used a combination of methods tocollect data [30, 32, 36–38, 43, 44, 46, 50, 52, 53]. Surveysor questionnaires were used in seven studies [32, 36, 37,40, 51–53]. Chart audits were used in four studies [32, 36,46, 53]. One study used field observations as part of theirmethodology [30]. One study was a systematic review [56].35, 38, 40, 45, 52]. One study had a mix of refugees andother marginalised groups [60]. Furthermore, some studies appear to have published different findings from thesame data set [19, 55, 58, 59].Au et al. BMC International Health and Human RightsFig. 1 Adapted PRISMA 2009 Flow DiagramCountry of originRefugees came from over 39 countries or regions. Themost investigated country of origin was Afghanistan;others were the African continent, countries from theMiddle East, Vietnam, Sri Lanka, and South-East Asia.Study settingsMajority of studies were carried out in Australian capitalcities. Half of all the primary studies were performed inMelbourne [18–20, 29, 35–38, 40, 47–50, 52, 55, 57, 59].Three studies did not specify the study setting [42, 46,53]. Only one study was performed in a rural or regionalarea [54].Health services exploredParticipantsRisk of bias within studiesThe perceptions of approximately 1855 refugees werecaptured. Five studies had a mix of refugees and migrants and did not identify those with refugee status [33,The results of the qualitative appraisal are summarisedin Table 2. Quantitative, mixed methods, and systematicreview appraisals are summarised in Table 3. SevenA diverse range of services were captured. Maternity services were the most frequently investigated [29, 32, 35,39, 42, 47–50, 53, 57–59]. Six studies investigated all services [20, 33, 37, 40, 44, 60] which was followed by mental health [19, 38, 55, 56] and primary care [30, 43, 54].
y et al.2017[28]Carolan et al.2010[29]Cheng et al. 2015[30]Clark et al. 2014[31]Correa-Velezet al. 2012[32]Henderson et al.2011[33]Kay et al. ital,QueenslandSouthAustraliaPharmacyAll servicesMaternityservicesUsing healthservices andmedicineswhile livingin AustraliaCity ofPrimary careGreaterDandenongand City ofCasey, landStudy setting3861816Semi-structuredFocus groups342aSudan (1)Sudan, Afghanistan,Pacific Islands andMyanmarSudan (14)Burundi (5)Ethiopia (2)Congo (1)Somalia (1)Sudan, Burundi, Congo(15)Burma (10)Afghanistan (5)Bhutan (8)Afghanistan (6)Ethiopia (1)Sudan (12)Eritrea (2)Somalia (2)Kenya (1)Somalia (5)Congo (5)South Sudan (2)Uganda (1)Burundi (1)Liberia (1)Eritrea (1)NumberCountry of Origin orof Refugees BackgroundChart audit and surveys 23(separate surveys withhospital staff)Focus groupsSemi-structuredinterviews and fieldobservationIn-depth interviewsFocus groupsStudy MethodsFive barriers were identifiedUnfamiliarity with healthservices, difficulties accessingcare were experienced byCALD communities. CALDcommunities valued traditionalmedical practices and wantedhealth practitioners to respectthis. Language barriers andinterpreter issues prominent.Participants stated the need forinterpreters, education programsfor pregnant women, andcontinuity of care.Patients found that languagebarriers were the main barrierto accessing primary health care.Interpreters wereused inconsistently, and patientsnoted poor literacy.Barriers to healthcare for newlyarrived refugees include languageand cultural responsiveness,appointments, difficultieswith transport to the practice,long wait times and the costof care.Five themes that Africanrefugee women givingbirth encounter: pregnancyis not special; resettlementis a priority; childbearing isa normal process; comingto value continuouspregnancy care; and culturalsensitivity is important.When describing theirexperiences in accessingpharmacy services, refugeesnoted four overarchingthemes: health systemdifferences, navigatingthe Australian healthsystem, communicationbarriers and health careseeking behaviour.Main Findings(2019) 19:22Barriers and facilitators ofAccess and use of healthservices by four CALDcommunities in Logan,Queensland.Developing a model ofrefugee maternity healthcarefor from consultations withstakeholders, chart audit andsurveys with health serviceproviders and refugees.Barriers to accessing primaryhealth care services andexploration of medicine-relatedissues as experienced byrefugee women in SouthAustralia.Factors influencing Afghanrefugees’ access at a singlegeneral practice in south-eastMelbourne in 2013.Experiences of African-bornpregnant women receivingantenatal care in Melbourne.African refugees’ experiencesof barriers in accessingpharmacy services in Brisbane.AimTable 1 Table of Results. Number of refugees marked witha indicate that it is a mixed populationAu et al. BMC International Health and Human RightsPage 5 of 23
puttonget al. 2006[35]McBride et al.2016[36]McBride et al.2017[37]McCann et al.2016[38]Murray et al. 2010[39] QualitativeStudyDesignStudyBirth experiences of Africanrefugee women in Brisbane.Help-seeking barriers andfacilitators of mental healthand substance use servicesin recently arrived young SubSaharan African migrants inMelbourne.Experiences of refugeesin using Monash HealthRefugee Healthand Wellbeing services.Evaluation of the RefugeeHealth Nurse Liaison roleat Dandenong h-EastRegion toriaQueenslandquality use of medicinesfor from primary healthcareproviders and refugee healthleaders in Brisbane.Experience of caesarean birthamong Cambodian, Lao andVietnamese women.Study settingAimSemi-structuredinterviews (18) andsurveys (159)Semi-structuredsurveys (60) andchart audits (journalswere only used withservice providers)In-depth interviewsinterviewsStudy ental health In-depth interviewsand(28) and focussubstancegroups (41)use servicesAll servicesRefugeeHealth edTable 1 Table of Results. Number of refugees marked witha indicate that it is a mixed population (Continued)Sudan (5)Liberia (1)Ethiopia (2)Somalia (2)Sub-SaharanAfrica69a10Afghanistan (77)Sri Lanka (43)Iran (11)Myanmar (16)Iraq (3)Pakistan (14)Bangladesh (7)Other (6)Afghanistan(30)Sri Lanka (12)Iran (6)Burma (2)Iraq (2)Sudan (1)Pakistan (3)Other (2)Laos (30)Vietnam (30)Cambodia (31)1776091aMyanmar (1)Liberia (1)NumberCountry of Origin orof Refugees BackgroundRefugee birthing experiences faced some uniquechallenges such as languagebarriers, the refugee experience,female genital mutilation, andhealthcare staff with little culturalParticipants noted four helpseeking barriers that preventedthem from seeking help formental health and alcoholand drug use: stigma of mentalillness, lack of mental healthliteracy in parents and youngpeople, perceived lack ofcultural competency of formalhelp sources, and financialcosts deterring access.Refugees were highly satisfiedwith the service emphasisingthe importance of a trustingrelationship with staff, accessto bicultural support workers,onsite interpreting andintegrated care.Patients noted that RefugeeHealth NurseLiaisons were helpful ininterpreting and providinghelpful information.Women’s experiences incaesarean birth have threemain themes: trust in medicalknowledge,expectations andcommunication with anunderstanding of their caregivers’preferences.between HCWs and refugeehealth leaders: communicationand language constraints,cultural issues, limited healthliteracy, financial cost, andhealth system concerns.Main FindingsAu et al. BMC International Health and Human Rights(2019) 19:22Page 6 of 23
tativeQualitativeQualitativeQualitativeStudyNeale et al. 2007[40]Nicol et al. 2014[41]Niner et al. 2013[42]O’Callaghan et al.2007[43]Omeri, A et al.2006[44]Owens et al.2016[45]Phillips 2013[46]Fairfield, NewSouth WalesNot specifiedWesternAustraliaMelbourne,VictoriaStudy settingNot dinterpretingCommunitybasedmaternityservicesAll servicesPrimary careMaternityservicesChild dentalhealthservicesAll servicesServiceExploredChart audit (265) andinterviews ews and focusgroupsSemi-structuredinterviews (20) andfocus groups (20)InterviewsFocus groups(interviews were onlywith y MethodsAfghanistan, Bosnia,Burma, Iran, Iraq, SierraLeone, SudanIndonesia (1)Pakistan (1)Vietnam (1)Iran (1)Sudan (1)Myanmar (6)Thailand (1)12a273Afghanistan(38)Vietnam (40)Myanmar (15)Burma (16)Iraq, Kuwait (9)Sudan (5)Afghanistan (3)Burundi (2)Congo (2)Rwanda (1)Nigeria (1)Somalia (67)Eritrea (29)Ethiopia (24)Sudan (6)38401539126aNumberCountry of Origin orof Refugees BackgroundRemote interpreters donot provide the samecare and attention asan on-site interpreter.Women noted lack of socialsupport during pregnancy,language difficulties, andcultural differences. Theywere happy with thecompleteness of carethroughout pregnancy.Four main themes emerge fromAfghan refugee experiences ofaccessing healthcare: emotionalresponses to trauma and migration,culture specific health maintenancestrategies, cultural views onmental health, barriers impedingaccessibility and cultural factorsinfluencing outcomes.Women’s health literacy influencemedication use and their rationale.Refugees have concerns abouthealth professionals not favouringtraditional medicine use.Many patients used self-reliancewhen emotionally distressed.They were unsettled by themedicalisation of birthing andreaction to health service variedfrom gratitude to feelings ofdiscrimination.Many participants felt overwhelmeddue to misinformation and lowhealth literacy. Themes involvedincluded parents’ pastexperience, resettlement issues,and enablers and barriers toaccessing dental services.Difficulties with language, includingthe availability of interpreters, wereidentified as the main barriers toaccessing appropriate healthservices. Half reported difficultieswith accessing services.competence.Main Findings(2019) 19:22Readily accessible remotetelephone interpreting in theresettlement experience ofrefugees.Refugee and migrant women’sperceptions of using antenatalhealthcare services in Perth.Beliefs, practices and experiences New Southof Afghan people in accessingWales (mosthealthcare in New South Wales. likely Sydney)Experiences of older Vietnamesewomen in using medications inFairfield, NSW.Experiences of pregnancy andbirth before and afterresettlement for Karen womenin Australia.Refugee experience, access andunderstanding relating to earlyoral health.Health service use and barriersof recently arrived immigrantsfrom the Horn of Africa inMelbourne.AimTable 1 Table of Results. Number of refugees marked witha indicate that it is a mixed population (Continued)Au et al. BMC International Health and Human RightsPage 7 of 23
Experiences of Karen womenin group pregnancy care inMelbourne.The experiences of Afghanwomen and men of refugeebackground having a babyin Melbourne, Australia.Understanding health systemnavigation and the role oftechnology for young peoplebelonging to one or moremarginalised groups.QualitativeQualitativeQualitativeRiggs et al. 2017[49]Riggs, Yelland, Szwarc Qualitativeet al. 2016[48]QualitativeRiggs et al. 2016 [59]Robards et al. 2019[60]Russo et al. 2015[50]City ofGreaterNew SouthWalesGreaterDandenongand Casey inMelbourneMelbourne,VictoriaSouth-Eastregion ofMelbourneWyndhamand Hume inMelbourne,VictoriaStudy settingMaternal andchild healthAll servicesMaternal andchild healthservicesMaternityservicesMaternaldental healthservicesMaternal andchild healthservicesservicesServiceExploredFocus groups (28)and in-depth interSemi-structuredinterviewsInterviews (focusgroups were onlywith serviceproviders)Focus groupsFocus groups(interviews were onlywith serviceproviders)Focus groups(interviews were onlywith serviceproviders)Study Methods38Afghanistan(38)Afghanistan(30)309aKaren (19)Afghanistan (14)Sri-Lanka (13)Karen, Iraqi, AssyrianChaldean, Lebanese,South Sudanese,Bhutanese192787NumberCountry of Origin orof Refugees BackgroundThe majority of patients reportedpositive experiences with HCWsMarginalised young peopleare ambivalent about theirhealthcare journey. Forrefugees, confidentialityconcerns, discrimination andconfusion over the complexityof the health system werecommonly encountered themes.Afghan men found their role asa father changed in Australiabut were generally pleasedwith the changes. Menappreciated when healthprofessionals took an interestin them and would prefer ifHCWs were responsive to issuessurrounding settlement in anew country.Women felt empowered andreassured when learning aboutpregnancy, sharing stories anddeveloping trusting relationshipsin a group setting. Communicationand privacy were issuesencountered in the hospital.Afghan men provided transport,translation and their role in caringfor their wives challenged traditionalpreconceptions. Afghan men wouldlike health professionals to enquireabout their health concerns.Barriers for patients includedaccess to transport, lack ofconfidence in speaking English.Continuity of care was appreciatedand preferred. 4 identified themesincluded facilitating access tomaternal and child health services,promoting continued engagementwith the MCH service, languagechallenges, and what is workingwell and could be done better.Longer conversations,more interruptions, canoccur with remoteinterpreters.Main Findings(2019) 19:22Emotional and socialwellbeing of new mothersExperiences of barriers,knowledge and surroundingbeliefs of maternal oral healthfrom refugees and serviceproviders.To explore the utilisation andexperience of maternal andchild health services inMelbourne for parents ofrefugee backgroundfrom the perspective ofusers and providers.QualitativeRiggs et al. 2012[47]AimStudyDesignStudyTable 1 Table of Results. Number of refugees marked witha indicate that it is a mixed population (Continued)Au et al. BMC International Health and Human RightsPage 8 of 23
dmethodsStudySamuel et al.2017[20]Sheikh et al. 2011[51]Sievert et al. 2018[52]Stapleton et al.2013[53]Women from refugeebackground’s experiences ofantenatal healthcare at anAustralian tertiary publichospital.To characterise and identifyhealth literacy of chronichepatitis B and barriersaccessing healthcare inat-risk migrant populations.Identifying issues affectingnewly arrived refugees inaccessing an emergencydepartment.Narratives of health-seekingbehaviours of Sri-Lankan Tamilrefugees in Melbourne.All servicesNot specifiedMonashHealth liverand refugeeclinics inMelbournesuburbsMaternityservicesLiver andrefugeeclinicsLiverpoolEmergencyHospital, New departmentSouth WalesMelbourne,VictoriaDandenongservicesand City ofCasey, Victoriafrom Afghanistanliving in Melbourne.ServiceExploredStudy settingAimFocus groups (18),surveys (42) andchart audit (190)Surveys (14) andsemi-structured interviews terviewsviews (10)Study MethodsTable 1 Table of Results. Number of refugees marked witha indicate that it is a mixed population (Continued)Africa, MiddleEast and othercountriesAfghanistan(11)Myanmar (8)South Sudan(14)33a250Africa (106)Middle East (49)Sri Lankan (12)15512NumberCountry of Origin orof Refugees BackgroundPatients noted differencesbetween theirtraditional birthing practicesand Western practices.Continuity of care throughoutantenatal period providedsecurity and support tonegotiate an unfamiliarsetting.Refugees and asylumseekers living withchronic hepatitis B havecompeting social pressureswhich impact their prioritisat
(MCAT) was developed using components of Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Qualitative Research, Critical Appraisal Skills Programme Qualitative Appraisal Checklists, and McMaster Univer-sity Critical Review Form, in order to capture the breadth and depth of assessment made by different tools (Add-itional file 1)[27].