Transcription
HIVTHE AMERICAN ACADEMY OF HIV MEDICINE www.aahivm .org AUGUST 2016Patient Care, Practice Management & Professional Development Information for HIV CARE ProvidersSpecialistSPECIALISSUEFirstLookAT THEHRSAHIV WorkforceStudyWorkforceSupply & Demand2Ryan WhiteProvider Network10PARTNER Study24EmergingSyphilis Epidemic27
CONTENTSHIVSpecialistTHE AMERICAN ACADEMY OF HIV MEDICINEPatient Care, Practice Management & ProfessionalDevelopment Information for HIV Care ProvidersAugust 2016 Volume 8, No.3 www.aahivm.orgCHAIR/BOARD OF DIRECTORSZelalem Temesgen, MD, AAHIVSEXECUTIVE DIRECTORJames Friedman, MHADIRECTOR OF MARKETING& COMMUNICATIONSAmber McCrackenEDITORRobert GattyG-Net Strategic Communicationsbob@gattyedits.comPUBLICATION DESIGNAND ART DIRECTIONBonoTom Studio, Inc.703-276-0612, info@bonotom.comADVERTISINGJane Dees RichardsonAAHIVM Advertising Salesc/o Ad Marketing Group, Inc.703-243-9046 ext. 102, Fax: 856-219-8957jrichardson@admarketinggroup.comF E AT U R E S2 The HIV Clinician Workforce 18 Ending the Epidemicin the United StatesSupply and Demand Projectionsfrom 2010 to 2015Boyd Gilman, Ph.D., Ellen Bouchery, M.S.,Paul Hogan, M.S., Sebastian Negrusa, Ph.D.,Sylvia Trent-Adams, Ph.D., andLaura Cheever, M.D.10 Characteristics of the RyanWhite HIV/AIDS ProgramProvider NetworkImplications for Access to Careunder the Affordable Care ActEllen Bouchery, M.S., Boyd Gilman, Ph.D.,Sylvia Trent-Adams, Ph.D., andLaura Cheever, M.D.The New York State PlanBill Valenti, MD22 The Brave New Worldof Life And DisabilityInsurance for theHIV Positive PopulationLarry M. Halpern andJason M. Halpern18 Ending the HIV EpidemicThe New York State PlanBy Bill Valenti, MDA Special ReportBy James M. Friedman, MHA,Executive Director, AAHIVM24 BEST PRACTICESPARTNER StudyBy William R. Short, MD, MPH, AAHIVS1705 DeSales St., NW, Suite 700Washington, D.C. 20036202-659-0699 202-659-0976info@aahivm.org www.aahivm.orgEDITORIAL ADVISORY GROUPCHAIRJeffrey T. Kirchner, DO, FAAFP, AAHIVSMedical DirectorPenn Medicine/LGHP Comprehensive CareLancaster General Hospital, Lancaster, PAJoseph S. Cervia, MD, MBA, FACP,FAAP, FIDSA, AAHIVSClinical Professor of Medicine and Pediatrics,Hofstra North Shore-LIJ School of Medicine;Regional Medical Director, HealthCarePartners, IPA & MSO,Garden City, NYD. Trew Deckard, PA-C, MHS, AAHIVS,Steven M. Pounders, MD, PADallas-Fort Worth, TXTeresa Mack, MDSt. Lukes—Roosevelt HospitalNew York, NYRichard C. Prokesch, MD, FACP,FIDSA, AAHIVSInfectious Diseases Associates,Riverdale, GAJeffrey T. Schouten, MD, AAHIVE,Attorney at LawD E PA R T M E N T S1 LETTER FROM THE DIRECTORPUBLISHERThe American Academy of HIV MedicineDirector HIV/AIDS Network Coordination(HANC) Project, Fred Hutchinson CancerResearch Center, Seattle, WA27 AT THE FOREFRONTEmerging Syphilis EpidemicAmong MSM Living with HIVBy Demetre Daskalakis, MD, MPHSami Shafiq, PharmD, CPH, AAHIVELead HIV/AIDS Clinical PharmacistWalgreens PharmacyMiami, FLWilliam R. Short, MD, MPH, AAHIVSSidney Kimmel Medical CollegeThomas Jefferson UniversityPhiladelphia, PACarl Stein, MHS, PAC, AAHIVSOwen Medical GroupSan Francisco, CASharon Valenti, NP, AAHIVSSt. John Hospital and Medical CenterGrosse Point Woods, MI
LETTER FROM THEDIRE CTO RBY JAMES M. FRIEDMAN, MHAEXECUTIVE DIRECTOR, AAHIVMA Special ReportThe Academy is both pleased and honored that the HIV/AIDS Bureau (HAB) of theHealth Resources and Services Administration (HRSA) has selected HIV Specialistto publish the two major articles reporting on their HIV Workforce Study. Becauseof the importance of the study, we are publishing a special edition of the magazineto correspond with the National Ryan White Conference on HIV Care & Treatment, ameeting that reiterates the continued need for a strong, well-funded Ryan White Program.There is a long history to the HIV Workforce and pray, a vaccine and a cure will finally eliminateStudy. Shortly after HAB selected the contractor, the need for most HIV practitioners. But until then,they held a meeting with outside individuals and we need to produce a workforce that is passionate,organizations who had an ongoing interest in educated and dedicated to providing the best careadvancing the HIV workforce. Atpossible for HIV patients.that meeting, which I attended, weAAHIVM has been working inthese areas for some time. For severalagreed to work with HRSA to provide guidance, support and accessyears, we have offered free dues formedical school students in hopes ofto HIV care providers as needed.While the study provides ansupporting their desire to go intoextensive look at the future of theHIV care. Our webinar programHIV workforce, the main takeawaydeveloped with Medscape providesis there is and will continue to be athe basics of HIV care to primaryshortage of practitioners that cancare practitioners. Our Fundamentalsadequately treat HIV. We find ourof HIV Medicine will be publishedselves within a perfect storm andthrough Oxford University PressJames M. Friedmanno shelter in sight. More and morethis summer and will have a broaderpatients know their status and can access insurance reach than in the past. In addition our HIV-Age.for the first time thanks to the Affordable Care org blog provides the HIV practitioner supportAct. Concurrently, the workforce is aging and with respect to the care of older HIV patients.many of our providers are retiring without a newI urge you to read these articles carefullyand give us your thoughts on their conclusionsgeneration to take their place.There is good news on the prevention and and especially additional ideas for solutions. Itreatment fronts, however. Widespread utilization would like to express my thanks to AAHIVMof PrEP and PEP will help with prevention. The Communications Director Amber McCracken forcoming of long-term treatment regimens, such as overseeing this special issue and, again, a sincereinjectables and single-dose therapy, will improve thank you to HAB for the opportunity to reportadherence and outcomes. And one day, we hope on this important study.HIVwww.aahivm.orgWhile thestudy providesan extensivelook at thefuture of theHIV workforce,the maintakeawayis there isand willcontinue to bea shortage ofpractitionersthat canadequatelytreat HIV.HIVSpecialistAUGUST 20161
2AUGUST 2016HIVSpecialistwww.aahivm.orgSHUTTERSTOCKThe HIVClinician Workforcein the United States
IN THE UNITED STATES, APPROXIMATELY 1.1 MILLION ADULTS AND ADOLESCENTS ARE LIVING WITHHIV, and each year another estimated 50,000 become infected.1 Because of advances in HIVcare, people are living longer with the disease than they previously did.1 Moreover, at the endof 2008, an estimated 20% of the people living with HIV were undiagnosed.1 Only 77% ofHIV-diagnosed people are linked to care within four months after diagnosis, and only about 51%of those with an HIV diagnosis are engaged in long-term care.1 Should universal routine HIVtesting for people ages 13 through 64 be adopted, as is recommended by the Centers for DiseaseControl and Prevention (CDC), and improvements in linkages with and engagement in care beachieved, the demand for HIV care will increase rapidly and create significant new challenges forthe health care system.2 The 2010 Patient Protection and Affordable Care Act should also resultin increased access to care for people with HIV who have not previously seen a provider. Underthe law, people who are living with HIV but not diagnosed or who are at increased risk for HIVwill be more likely to be screened for HIV infection and, among those newly diagnosed, to receiveservices that strengthen their ability to adhere to treatment.Evidence suggests that the supply of HIV clinicians mightnot be keeping pace with the growth in the demand for HIVhealth care services. In a 2008 survey, the American Academyof HIV Medicine (AAHIVM) found that one third of itsmembers plan to retire within the next 10 years.3 Anotherstudy found that nearly 70% of all practices funded for earlyintervention services under the Ryan White HIV/AIDSProgram have a difficult or very difficult time recruitingprimary care providers.4 A recent qualitative assessment ofthe HIV workforce conducted by the federal governmentconcluded that “the Nation faces severe workforce capacitychallenges to effectively treat people living with HIV/AIDS(PLWHA). The demand for HIV and primary health careservices, in particular, continues to increase as treatingPLWHA becomes more complicated and new cases arise.Exacerbating workforce demands are the many experiencedSupply and Demand Projectionsfrom 2010 to 2015Boyd Gilman, Ph.D.Paul Hogan, M.S.(corresponding author)The Lewin GroupMathematica Policy Research Sebastian Negrusa, Ph.D.Ellen Bouchery, M.S.The Lewin GroupMathematica Policy ResearchSylvia Trent-Adams, Ph.D.Office of the Surgeon GeneralU.S. Department of Healthand Human ServicesLaura Cheever, M.D.Health Resources andServices AdministrationU.S. Department of Healthand Human ServicesDISCLAIMER: The views expressed in this article are those ofthe authors. No official endorsement by the U.S. Department ofHealth and Human Services is intended or should be inferred.3
health professionals retiring from practice while young providers choosemedical fields outside of HIV and primary health care.”5 Reflecting thisview, the two medical societies for HIV care and treatment in the UnitedStates—AAHIVM and the HIV Medicine Association—released a jointstatement: “With the growing number of people living with HIV, a failureto promptly address HIV medical workforce issues could lead to thecollapse of the HIV care system—risking lives and the public health ofcommunities across the country.”6In September 2010, amid growing concern about the potential shortageof HIV clinicians, the Health Resources and Services Administration withinthe U.S. Department of Health and Human Services (HHS) sponsored thefirst national study to quantify the number of clinicians providing HIVmedical care in the United States and to forecast the magnitude of the HIVclinician shortage or surplus.7 HHS initiated the study to assess whetherthere were sufficient providers available to address the goals of the NationalHIV/AIDS Strategy, launched by the White House Office of National AIDSPolicy in 2010 to reduce new HIV infections, increase access to care andimprove health outcomes for people with HIV, and reduce disparities inaccess to care among individuals living with HIV.8 The results from thatnational HIV clinician workforce study are summarized in this article.The health profession workforce issues addressed in this study areunique and require special attention for several reasons. First, HIV is a4AUGUST 2016HIVSpecialistwww.aahivm.orgcommunicable disease and, unlike most chronic conditions, failure todeal with shortages in care will have long term adverse consequencesfor public health in this country. Second, the expansion of health carecoverage under the Affordable Care Act has the potential to bring a largeproportion of the population currently living with HIV but not yet diagnosed, or those diagnosed but not yet linked to care, into the health caresystem. In 2012, over 62% of individuals diagnosed with HIV receivedmedical and support services funded by the Ryan White HIV/AIDSProgram9 and 78% of these clients had income below 200% of the federalpoverty level, making them potentially eligible for subsidized coverageunder the Affordable Care Act.10 Efforts must be made now to prepare forthe opportunity that health reform brings to identify and engage in carethose who are currently not receiving optimal treatment or not effectivelymanaging their HIV disease. Finally, unlike other chronic conditions,HIV care in this country has historically been managed by cliniciansfrom multiple health care professions and medical specialties, many ofwhom spend only a part of their clinical time treating patients with HIV.The diversity of the HIV workforce means that the administrative recordsof medical specialty societies cannot be used to identify HIV clinicians.Instead, we used medical and prescription drug claims to create the firstnational census of providers who manage HIV care in the United Statestoday and conducted a survey to characterize their HIV practice behavior.ISTOCKTHE HIV CLINICIAN WORKFORCE IN THE UNITED STATES
METHODS AND DATADefining and Characterizingthe HIV Clinician WorkforceGiven the lack of an established credentialing requirementfor physicians and nonphysician clinicians providing HIVservices, we identified (in consultation with a technicalexpert panel of HIV clinicians and practice administrators)potential HIV clinicians based on the services they providedas reported in a national pharmacy and medical claimsdatabase obtained from SDI Health containing claims fromall payers (including managed care plans), billing providers,and geographic regions. We pulled the data in October 2011and identified HIV clinicians based on claims from 2010.We identified 572,952 patients with at least one HIV-relatedclaim, representing two thirds of all diagnosed cases, andan even higher proportion of those in care. Clinicians withHIV-related visits or prescription claims for 10 or morepatients who were physicians, nurse practitioners, andphysician assistants in internal or family medicine, generalpractice, and infectious disease were deemed potential HIVclinicians. We excluded clinicians who treated fewer than10 patients with HIV because these clinicians are less likelyto manage HIV care on an ongoing basis. Based on theseparameters, we identified 9,145 potential high-volume HIVclinicians in the claims database.To obtain more information about the HIV care providedby these clinicians and to develop supply-side inputs thatreflect the behavior of HIV clinicians, in 2012 we surveyed anationally representative probability sample of 5,000 of thesepotential HIV clinicians. Only 55.1% of the original samplewas eligible for the survey. Most of those deemed ineligibleindicated that they did not provide HIV treatment to 10 ormore patients diagnosed with HIV. Among those eligiblefor the survey, 42.9% responded. The number of completedeligibles enabled us to estimate national supply-side inputparameters for selected age, gender, and health professiongroups with statistical precision. We weighted the analysesto adjust for survey sampling and for differential nonresponse patterns.11Calculating the Demandfor HIV-Related Medical CareWe defined demand as the total number of HIV-relatedmedical visits provided under market conditions in 2008.We calculated the total number of visits provided based on(1) the number of individuals diagnosed and living withHIV/AIDS as identified in CDC and state and local surveillance data and (2) the number of HIV-related medicalvisits per diagnosed person. We calculated visit rates perdiagnosed person in the base year as the ratio betweenthe total number of HIV-related visits used and the totalnumber of diagnosed persons in each age and gender group.We identified HIV-related visits and inpatient stays fromvarious sources, including two National Center for HealthStatistics (NCHS) provider surveys and the Health CareCost and Utilization Project’s National Inpatient Sample(HCUP-NIS).12 We excluded visits related to HIV testingand counseling because our analysis focused on clinicianswho manage HIV care longitudinally. We included visits forwhich HIV was a secondary diagnosis because the presenceof HIV as a secondary diagnosis can complicate treatment,implying that optimal treatment of the primary diagnosismight require the knowledge of an HIV specialist.Forecasting the Supply and Demandof HIV CliniciansWe projected the supply and demand of HIV cliniciansfrom 2011 to 2015 using a Markov model. We calculatedthe number of HIV clinicians in each year as the number ofHIV clinicians in the prior year plus entrants into the HIVworkforce and minus losses from retirement and mortality.We estimated entry into and retirement from the HIV clinician workforce from survey responses. To estimate the totalnumber of visits supplied by the workforce, we multipliedthe supply of HIV clinicians in each year by survey-basedestimates of the average number of hours worked per year,the proportion of time spent in HIV care, and the numberof visits provided per hour. We assumed these parametersremained constant for each age, gender, and health professioncategory throughout the projection period.The projections reflect a real and growing shortage ofHIV clinicians as current providers reach retirement age andthe number of people living with HIV continues to grow.We calculated the number of individuals diagnosed withHIV in each projection year as the number of individualsdiagnosed with HIV in the prior year plus newly diagnosedcases minus mortality, based on CDC and state and localsurveillance data. We assumed utilization rates per diagnosedperson by age, gender, and race remained constant throughoutthe projection period. We multiplied the average utilizationrates per diagnosed person by the forecasted number ofdiagnosed cases in each age and gender category to obtainthe total number of HIV visits demanded in each forecastedyear. We converted forecasted visits supplied and demandedto full-time equivalent (FTE) clinician values based on theaverage number of HIV-related visits supplied per full-timeclinician in the base year.RESULTSTable 1 shows the distribution of the estimated 4,937 HIVclinicians practicing in 2010 identified in this study. Ofthese, an estimated 54.5% were primary care physicians,37.2% were infectious disease specialists, and 8.3% werenurse practitioners or physician assistants. An estimated65.8% of the HIV clinicians were male and 16.5% wereage 65 and older. The majority of the HIV clinicians werewhite non-Hispanic (68.0%), and the largest share (39.7%)www.aahivm.orgHIVSpecialistAUGUST 20165
THE HIV CLINICIAN WORKFORCE IN THE UNITED STATESpracticed in the South. Overall, 13.2% of the HIV physicianswere trained outside of the United States.Table 2 provides an estimate of the number of HIV-relatedmedical visits supplied in 2010. Primary care physicians reported spending on average 1,872 hours per year in patientcare, with 30.4% of their clinical care time spent treatingpatients with HIV. Infectious disease specialists reportedspending a similar amount of time in patient care (1,871hours per year) but devoted nearly 30% more of their timeto treating patients with HIV (39.3%) than did primary carephysicians. Nonphysician clinicians reported spending moretime in clinical care (1,993 hours) and a higher share of theirtime treating patients with HIV (66.9%) than their physicianTable 1. Number and Percentage of High-Volume HIV Clinicians,by Clinician Type, Demographic Group, and RegionNumberof HIVCliniciansPercentageof HIVClinicians4,937100.0Primary care physicians2,69154.5Infectious disease 34.2Younger than 45 years1,57031.845 to 64 years2,55251.781516.5White, non-Hispanic3,36268.0Black, non-Hispanic4108.3Hispanic3607.3Other/multiple race, 7Midwest74615.0West84417.1United States4,28586.8International65213.2Number of CliniciansClinician TypeNurse practitioners and physician assistantsGenderAge Group65 years and olderRace/EthnicityCensus RegionCountry of Highest Clinical DegreeSource: HIV Clinician Workforce Survey 2012.Note: The results are weighted to account for the probability of selection and for differential surveynonresponse patterns. Percentages might not sum to 100% because of rounding. High-volume providers arethose who treated 10 or more patients with HIV in 2010.6AUGUST 2016HIVSpecialistwww.aahivm.orgcounterparts. Physicians reported conducting on average 1.5HIV-related clinician visits per hour, compared with 1.4 visitsper hour for nonphysician clinicians. In total, we estimatethat the HIV clinicians identified in this study provided 5.1million HIV-related medical visits nationally in 2010.Table 3 displays the total number of HIV-related visitsdemanded and received in 2008. This total includes visits inambulatory settings (on average, 5.1 visits per diagnosed personannually), as well as visits provided to hospital inpatients (onaverage, 0.92 visits per diagnosed person annually). Theseaverages include people with HIV who were engaged in care, aswell as those who received treatment sporadically. Overall, weestimate 5.1 million HIV-related medical visits were demandedin 2008. An estimated 62.8% of all HIV-related visits demandedwere for individuals ages 35 to 54. A total of 15.4 percent of allvisits in 2008 were for people 55 and older, a proportion that islikely to increase as the HIV population ages. Approximatelytwo thirds of total visits were for males (67.1%) and one thirdfor females (32.9%). Black non-Hispanics accounted for thehighest share of visits (45.0%), followed by white non-Hispanics(34.1%). Hispanic individuals represented 18.2% of all visitsdemanded. The South represented the highest proportion ofvisits (42.5%), followed by the Northeast (28.4%).Table 4 shows the forecasted number of HIV cliniciansand visits supplied from 2010 to 2015. Our model forecasts a
Table 2. Number of HIV Clinician Visits Supplied in 2010, by Clinician TypeType of Clinician(Column A) Number ofHIV Clinicians(Column B) Numberof Hours Worked perYear(Column E) TotalNumber of HIV VisitsSupplied(Column C) Proportionof Time Spent in HIVCare (%)(Column D) Number ofHIV Visits per 3,217NP/PAAll Clinicians1,872IDS infectious disease specialist; NP nurse practitioner; PA physician assistant; PCP primary care physician.Source: HIV Clinician Workforce Survey 2012.Notes: The results shown in Columns B, C, and D were derived from the model using statistically significant subgroup means only. The results are weighted to account for the probability ofselection and for differential survey nonresponse patterns.decline in the number of primary care and infectious diseasephysicians managing HIV care by 2015 of about 400 and 200clinicians, respectively. The number of nurse practitionersand physician assistants supplying HIV care is expected toincrease from 408 clinicians in 2010 to 511 clinicians in 2015.The total number of visits supplied is expected to decline 6.1%,from 5.1 million in 2010 to 4.8 million in 2015, with nonphysician clinicians providing an increasing share of HIV care.The decline in visits supplied is largely because the numberof clinicians entering the HIV workforce over the next fewyears is not sufficient to fill the gap left by clinicians leavingthe HIV workforce because of retirement and mortality. Thedecline in supply is also due to the demographic shift in theHIV workforce toward female clinicians. A disproportionatenumber of new entrants is female and, on average, femaleclinicians in HIV medicine work 11.2% fewer hours per weekthan their male counterparts (40.3 hours for women versus45.4 hours for men).Table 3. Number and Percentage of HIV Visits Demanded, byDemographic Group and Region, 2008Number of VisitsDemanded (inthousands)Percentageof VisitsDemanded5,148100.0Younger than 13 years280.513 to 24 years2935.725 to 34 years80015.535 to 44 years1,62331.545 to 54 years1,61431.355 to 64 years65812.865 years or older1322.6Male3,45567.1Female1,69332.9White, non-Hispanic1,75834.1Black, non-Hispanic2,31745.0Other/multiple race, non-Hispanic1382.7Hispanic only93518.2Northeast1,46328.4SouthDemographic GroupTotalAge .5Midwest60411.7West89117.3Source: National Ambulatory Medical Care Survey (NAMCS) (2009) and National Hospital AmbulatoryMedical Care Survey (NHAMCS) (2008), HCUP-NIS data (2002–2009), and federal and state HIVsurveillance data (2008).Note: Percentages might not sum to 100% because of rounding.www.aahivm.orgHIVSpecialistAUGUST 20167
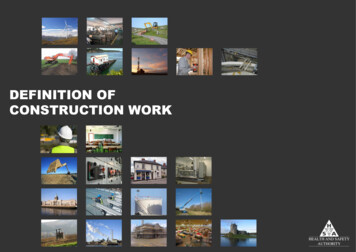
THE HIV CLINICIANWORKFORCE IN THEUNITED STATESTable 4. Forecasted Supply and Demand of HIV Visits, 5HIV 1,893,4501,849,7541,806,565TotalHIV Visits ,8661,966,3492,011,784Younger than 35 1,824,07035 to 44 1,925,4915 to 54 5,738TotalHIV CasesHIV Visits DemandedGenderAge Group55 years or olderTotalIDS infectious disease specialist; NP nurse practitioners; PA physician assistant; PCP primary care physicians.Sources: HIV clinician workforce survey, 2012.Table 4 also shows forecasts of the number of HIV patients and visitsdemanded and received from 2010 to 2015. The number of diagnosedcases is expected to increase by about 140,000 (from 0.9 million in 2010to slightly more than 1.0 million by 2015) and the total number of visitsdemanded is expected to increase 13.8% (from 5.4 million in 2010 to 6.2million in 2015). The growth in the number of visits demanded is dueprimarily to the continued number of newly diagnosed cases each yearand the low mortality rate among the currently diagnosed population. Theincrease in demand is also due to the aging of the diagnosed populationand the higher rate of HIV-related visits among individuals ages 45 to 54.Figure 1 expresses demand and supply projections in FTE HIV clinicians per year over the five-year forecasting period, adjusted to reflectthat high-volume HIV clinicians spend, on average, less than 40% of theirtime treating patients with HIV. The total number of FTE HIV clinicianssupplied in the United States is expected to decline 5.5% over this period,from 1,812 FTE HIV clinicians in 2010 to 1,713 in 2015. During thesame period, the total number of FTE HIV clinicians demanded in theUnited States is expected to increase 13.9%, from the base-year valueof 1,945 to 2,215 by 2015. The net result is an estimated shortage of 133FTE clinicians in 2010, growing to a shortage of 502 FTE HIV cliniciansin 2015. Because few clinicians work full time in HIV care, the number8AUGUST 2016HIVSpecialistwww.aahivm.orgof providers needed to fill this gap will be substantially higher than thenumber of FTEs required.If expanded HIV testing efforts are successful in identifying and linking to care 5% of the estimated 240,000 living but undiagnosed cases ofHIV annually over the forecasted period, the shortfall of FTE clinicianswill increase to 36% of supply. A 5% increase in the proportion of timeclinicians spend treating patients with HIV would reduce the deficit to24.8% of supply, while a 10% increase in the number of visits per hourwould reduce the shortage to 17.6% of supply.Physicians providing a low-volume of services are not included inthe estimate of HIV physicians in this model. Low-volume providers canaddress some of this excess demand. However, the projections reflect areal and growing shortage of HIV clinicians as current providers reachretirement age and the number of people living with HIV continues to grow.DISCUSSIONThe study offers several important insights into the HIV clinician workforce.HIV clinicians represent a range of medical specialties and health professions. Nurse practitioners and physician assistants are likely to become anincreasingly important component of the HIV workforce. Effective workforce
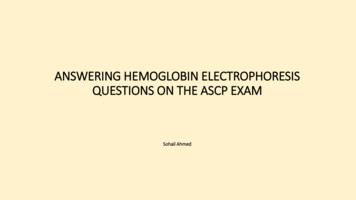
Number of FTE HIV Cliniciansstrategies will need to be taidiagnosed, people diagnosedFigure 1. Forecasted Supply and Demandlored to differences in trainingwith HIV but not yet in care,and scope of practice acrossand people in care but not yetof FTE HIV Clinicians, 2010–2015the range of HIV practitioners.receiving the optimal level ofAnother important feature ofcare. Nor do they take into2,400the HIV workforce is that mostaccount potential changes in2,200HIV clinicians spend only amarket conditions, such as2,2152,1612,107portion of their time treatingexpanded health insurance2,0532,0001,999patients with HIV. The capacitycoverage likely to occur after1,812of the HIV clinician workforcethe full implementation of the1,8001,8121,7931,7751,775might be expanded by increasAffordable Care Act in 2014.1,7351,7131,600ing the proportion of time thatOverall, the study shows aclinicians currently treatingsmall but rapidly expanding1,400patients with HIV spend inshortage of HIV providers.201120142010201220132015HIV care. Our analysis alsoOur forecasting model preYearidentified many clinicians whodicts that by 2015 the supFTEs DemandedFTEs Suppliedtreat a low volume of HIV paply of HIV clinicians will beFTE full-time equivalent.tients and who do not managesufficient to meet only threeSources: HIV Clinician Workforce Survey 2012, NAMCS (2009), NHAMCS (2008), HCUP-NISthe HIV treatment of thesequarters of total demand for(2002–2009), and federal and state HIV surveillance data (2008).patients on an ongoing basis.HIV-related medical servicesunder current market-basedThe HIV workforce might beexpanded by providing training or professional support, such as comanaging assumptions. Expanded HIV testing and diagnosis and improvementscare with HIV specialists, to low-volume clinicians.in linkages, engagement, and adherence to care—without an increaseThe study has several limitations. First, there are gaps in the data
of Life And Disability Insurance for the HIV Positive Population Larry M. Halpern and Jason M. Halpern 18 Ending the HIV Epidemic The New York State Plan 1 LETTER FROM THE DIRECTOR A Special Report By James M. Friedman, MHA, Executive Director, AAHIVM 24 BEST PRACTICES PARTNER Study By William R. Short, MD, MPH, AAHIVS 27 AT THE FOREFRONT