Transcription
2019Malcolm BaldrigeNational Quality Award Application
Table of ContentsOrganizational ChartGlossary of Terms andAbbreviationsOrganizational Profile .Page i-vCategory 1: Leadership .Page 1Category 2: Strategy .Page 7Category 3: Customers . .Page 12Category 4: Measurement, Analysis, and Knowledge Management Page 16Category 5: Workforce . .Page 21Category 6: Operations . Page 27Category 7: Results . Page 34
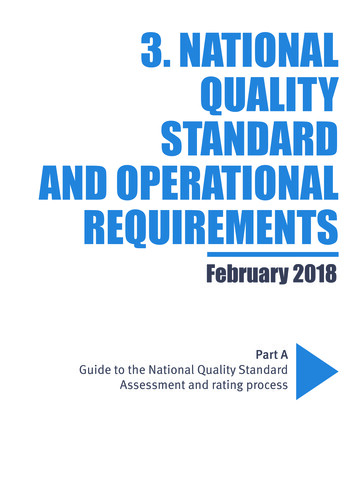
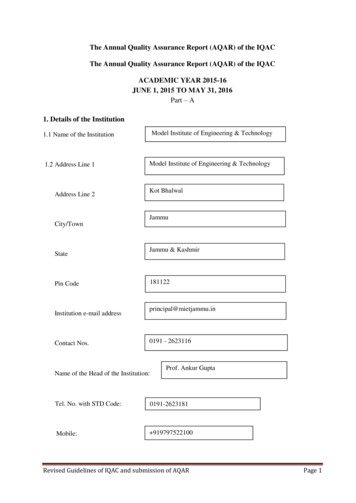
CityCouncilCity ofAmesOrganizationalChartBoard ofTrusteesAD003 – 04/19PRESIDENT & CEOBrian DieterQUALITYKaren Kiel RosserMedical StaffExternal Relations:Foundation/Older Adult Services/Volunteer ServicesMelissa McGarryFINANCEGary Botine(Privacy Officer)NURSINGCory Geffre, RNCLINICAL &SUPPORT SERVICESAmber Deardorff, RNCommunity RelationsSteve SullivanInpatient Nursing Services/House ManagersMatt Aitchison, RNHome Health/Hospice/Public HealthLes White, RNDietaryMatt HartBehavioral HealthChristy KrauseEmergency ServicesDieter Friton (Interim)Business Office/Patient Access ServicesHeather VandewaterChaplaincy ServicesKatherine WernerFirst NurseClinical Applications SystemsEvan DarnellFacilitiesJohn RodilossoCardiopulmonary Services:AccountingLori Vander WerffNeurodiagnostics/Home MedicalEquipmentTammy JarnaginProcess Improvement/LeanRon SmithGuest ServicesEnvironment Services/Valet/TransportationCathy WrightMedical Staff ServicesSally HouserShaunda Calkins, RNSupply Chain ManagementSue DraperQuality ManagementDarla Handsaker, RN(Compliance Officer)ICCUSarah Heikens, RN (interim)Maternal/Child/PediatricsAmy Dagestad, RNJane Jackson, RN (Interim)Medical/Surgical & Nursing SupportTeamJo-el Sprecher, RNMICS/SecurityDieter Friton, MHA, NRPMedical/TelemetryAmanda Lass, RNOncology/Cancer ServicesPalliative CareSarah Heikens, RNRehabInpatient HemodialysisJoelle Schmidt, RNPharmacyDoug Wetrich, RPhProfessional DevelopmentAmy Stark, RNBrian R. Dieter, FACHEPresident & CEOOutpatientNursing ServicesJane Jackson, RNAmbulatory CareBonnie Castro, RNCath Lab/Cardiac RehabCheryl Pietz,RN/Carrie Adams,RNDiabetes and NutritionEducationThyra Cox, RNGI ServicesDonna Henderson, RNPain Medicine ClinicJane Jackson, RNWound Healing Clinic/Wound Ostomy Care /StrokeProgramJane Jackson, RNBusiness IntelligenceAJ SmithHealth InformationManagementVicki DunnInformation SystemsScott CarlsonSecurity OfficerNicole PapeHuman Resources:Education Management/Medical LibraryPen ny Bel lvill eLaboratoryConnie HendersonRadiation OncologyScott CueRadiologyScott CueRehab & Wellness:Hospital Services/OP Svcs: Ames &Story City/Lifetime Fitness CenterMatt PetersenSurgical Services:Operating Room/Sterile Processing/Anesthesia/Post Anesthesia CareBrian Van Brocklin, RN
Glossary of Terms and AbbreviationsAAAHRMM .American Association for HealthcareResource & Materials ManagementAAR.After Action ReportACTS .Ambassadors, Communications, Teamwork,SafetyAHA .American Hospital AssociationAHRQ .Agency for Healthcare Research andQualityAIDET .Acknowledge, Introduce, Duration,Explanation, Thank YouAMI.Acute Myocardial InfarctionAMPT .Web-based Employee Recognition PlatformANCC .American Nurses Credentialing CenterAOS.Available on SiteA/R.Accounts ReceivableASC.Ambulatory Surgery CenterAT.Administrative TeamBBOTBSNCCACAHCAMCAPCARF.Board of Trustees.Bachelors of Science and Nursing.Cancer.Critical Access Hospital.Comprehensive Accreditation Manual.College of American Pathologists.Commission on Accreditation forRehabilitation FacilitiesCAS.Clinical Applications SystemsCAT.Computerized Axial Tomography, CATScan, a diagnostic test used to diagnoseconditions and diseasesCBES .Computer Based Education SystemCBL.Computer Based Learning ModulesCDC.Centers for Disease ControlCEO.Chief Executive OfficerCFO.Chief Financial OfficerCHF.Congestive Heart FailureCLIA .Clinical Laboratory ImprovementAmendmentsCMS .Centers for Medicare and MedicaidServicesCME .Continuing Medical EducationCNA.Certified Nursing AssistantCPOE .Computerized Prescriber Order EntryCT.Computerized TomographyDGlossaryDART . Days Away, Restricted or TransferredDMACC . Des Moines Area Community CollegeDNV. Det Norske VeritasDRG . Diagnosis Related GroupEe-Gram . Electronic Employee Newslettere-Physician . Electronic Physician NewsletterEAP. Employee Assistance ProgramEOC. Environment of CareED. Emergency DepartmentEDI. Electronic Data InterchangeEEOC . Equal Employment OpportunityCommissionEHR. Electronic Health RecordEMC . Emergency Management CommitteeEMP . Emergency Management PlanEMTALA . Emergency Medical Treatment and ActiveLabor ActEOS. Employee Opinion SurveyES. Environmental ServicesEPA .Environmental Protection AgencyFFMEAFMLAFLSAFOCUS. Failure Mode Effects Analysis. Family Medical Leave Act. Fair Labor Standards Act. Find a process to improve, Organize a team,Clarify current knowledge, Understandcauses of process variation, Select theprocess improvement toolFQHC . Federally Qualified Healthcare CenterFTE. Full Time EquivalentFY. Fiscal YearGGPO. Group Purchasing OrganizationHHAZMAT . Hazardous MaterialsHCAHPS . Hospital Consumer Assessment ofHealthCare ProvidersHEAT . Hear, Empathize, Apologize, TakeOwnershipHeC. Healthcare Enterprise CooperativeHEN. Hospital Engagement NetworkHHQI . Home Health Quality ImprovementHIMSS . Healthcare Information and ManagementSystems SocietyHIPAA . Health Insurance Portability andAccountability Act
HR.Human ResourcesIICU.Intensive Care UnitIDHP .Iowa Department of Public HealthIHA.Iowa Hospital AssociationIHC.Iowa HealthCare CollaborativeIHI.Institute for Healthcare ImprovementIMRT .Intensity Modulated Radiation TherapyIOE.Indicator(s) of ExcellenceIA DNR .Iowa Department of Natural ResourcesIP.InpatientIRPEISISCOISPITJJC.Iowa Recognition for PerformanceExcellence.Information Services.Information Security Compliance Officer.Internet Services Provider.Information Technology.Joint Commission on Accreditation ofHealthcare OrganizationsKKPMs .Key Performance MeasuresLERPLEMLILOSLPNLSS.Lawson Enterprise Resource Planning.Leadership Evaluation Manager.Leadership Institute.Length of Stay.Licensed Practical Nurse.Lean Six SigmaMMBNQA .Malcolm Baldrige National Quality AwardMcFC .McFarland ClinicMD.Medical DoctorMEC .Medial Executive CommitteeMGMC .Mary Greeley Medical CenterMICS .Mobile Intensive Care ServicesMMIC .Midwest Medical Insurance CompanyMPA .Masters of Public AdministrationMRI.Magnetic Resonance ImagingMVV .Mission, Vision, and ValuesNNEOGlossary.New Employee OrientationNDNQI . National Database of Nursing QualityIndicatorsNHSN . National Healthcare Safety NetworkNRC Health . National Research CorporationOOFIOIGOICOPOSHA. Opportunity for Improvement. Office of the Inspector General. Organizational Integrity Committee. Outpatient. Occupational Safety and HealthAdministrationOPSC . Organizational Profile & Strategic ContextOR VAT . Operating Room Value Analysis TeamPPCPCIPDCAPETPFACPGPHiPIPITPMSPNPPPRCPRIDE. Personal Computer. Percutaneous Coronary Intervention(s). Plan-Do-Check-Act. Position Emission Tomograph. Patient & Family Advisory Council. Press Ganey. Preventable Harm Index. Performance Improvement. Product Improvement Team. Performance Measurement System. Pneumonia. Performance Plan. Professional Research Consultants. People, Respectful, Innovative, Dedicated,EffectivePSC. Patient Satisfaction CommitteePTCA . Percutaneous Transluminal CoronaryAngioplastyPTO. Paid Time OffQQIPQPSCRRIEREAP. Quality Indicator Project. Quality & Patient Safety CouncilRFPRNROI. Rapid Improvement Event. Rewards for Employee AchievementProgram. Request for Proposal. Registered Nurse. Return on InvestmentSSAN. Storage Area Network
SCIP .Surgical Care Improvement ProjectSCM .Supply Chain ManagementSLA(s) .Service Level Agreement(s)SMART .Specific, Measureable, Achievable,Relevant, and Time-boundSNAP .Supplemental Nutrition Assistance ProgramSNF.Skilled Nursing FacilitySPTF .Strategic Planning Task ForceSWOT .Strengths, Weaknesses, Opportunities,ThreatsSP.Strategic PlanSPP.Strategic Planning Process5s.Sort, Straighten, Sweep, VOMVPW-ZGlossary.Turn Around Time.Transitional Care Unit.The Joint Commission on Accreditation ofHealthcare Organizations.Upper Iowa University.Urinary Tract Infection.Value Analysis Team.Value Based Purchasing.Value Stream Mapping.Voice of the Customer . Vector of Measures.Vice President
P.1a(1) Health Care Service Offerings MGMC is a public,not-for profit, 220-bed hospital. Main health care servicesoffered include inpatient (IP), outpatient (OP), emergencydepartment (ED), and home healthcare (HH) services (see alsoFigure P.1-1). A workforce of approximately 1,300 non-union,patient care and support staff, and a medical staff of over 200providers deliver health care services to those in need. FigureP.1-1 highlights the relative importance of each service nizational success and financial viability are supported byits focus on delivering health care services both efficiently andeffectively (Figures 7.1b(1)) and with a patient centered focus(Figures 7.2a).Figure P.1-1 MGMC Service mentHomeHealth/HospiceVolumeRevenue%8,510 admissions 245,524,39943%125,169 visits 286,892,88650%28,059 visits 34,623,8606%17,260 visits 6,933,4281%Mechanisms used to deliver health care services includedirect and indirect patient care and support services providedby a workforce described in P.1a(3) and Figure P.1-3.Mary Greeley Medical CenterP.1a(2) Mission, Vision, Values, and Culture. The mission,vision, and values (P.1-2) are the foundation of MGMC’sculture and as such, are the basis for the Indicators ofExcellence (IOE), long-term and short-term goals, and AnnualAction Plans within the strategic plan.P.1-2 MGMC Mission, Vision, Values, Core CompetenciesMissionTo advance health through specialized care and personal touch.VisionTo be the best.ValuesP – People Oriented, R – Respectful, I – InnovativeD – Dedicated, E – Effective (PRIDE)Core CompetenciesQuality, Safety, Patient ExperienceThe organization’s tag line Doing What’s Right captures a keycharacteristic of its culture and a unique element of MGMC’senvironment. This tag line, developed in part by employees,patients, and stakeholders during the re-branding process(1.1a(1)), reinforces the MVV and guides decision making,planning and engagement. It supports a culture whereemployees are empowered to continuously improve their workand to do what’s right.Through the SPP MGMC identifies and establishes corecompetencies (2.1a(4)) of high quality, safe care that isdelivered by an engaged workforce which, in turn, results in anexceptional patient experience. These three core competenciessupport the MVV, and are central to the strategic plan and itsIndicators of Excellence (IOE).P.1a(3) Workforce Profile MGMC’s workforce profile isdetailed in Figure P.1-3 and describes employee, physician andvolunteer educational requirements, workforce groups andsegments. The employed workforce is defined by twosegments: 1) patient care and 2) support services. The nonemployed workforce is segmented by physicians andvolunteers. Students are not included in our workforce numbersper the Baldrige definition as they do not do the work of theorganization.Figure P.1-3 Workforce Profile, Segments and Key RequirementsWorkforcePercent mentsEMPLOYEES 1,310RN/BSN,Patient Care70%MSN, PhD,Respect andAD, TechnicalCommunication(7.3-17; 7.4-1)High schoolSupport30%diploma, AD,ServicesTechnicalMGMC EmployedP.1 ORGANIZATIONAL DESCRIPTIONP.1a Organizational EnvironmentFor more than a century, Mary Greeley Medical Center hasprovided quality patient care for central Iowans. The hospital,which opened in 1916, was built by Captain Wallace Greeleyand given to the city of Ames, Iowa, in memory of his belovedwife, Mary, who died in 1914. Captain Greeley was a formerUnion Army officer during the Civil War. He and Mary settledin Ames, where he went on to become a prominentbusinessman, mayor and state legislator. Captain Greeley andMary also helped establish the city’s public library. In July1915, six months after Mary’s death, Captain Greeleyannounced his vision for the city’s first hospital. Prior to 1916,Ames had no hospital facilities for its citizens. Captain Greeleyconsulted a group of local physicians about where to locate thenew hospital and what to include in the building. He alsobrought in a medical specialist from Chicago who wasnationally known as a consultant in the design and constructionof hospitals. On Dec. 29, 1915, construction began on MaryGreeley Memorial Hospital. A local newspaper referred to theproject as “a most magnificent gift” to the city. The originalcost of the hospital was 80,000 and Captain Greeley providedan additional 3,000 for equipment and furnishings. Theoriginal building had 30 patient rooms. At the hospital’sdedication on Sept. 24, 1916, which was attended by more than2,000 people, Captain Greeley said, “It affords me greatpleasure, more than words can express, that I contributesomething towards the welfare of not only those now in need,but also for those who will be here long after we have passedaway.”Today, Captain Greeley’s vision to improve the quality oflife in this community and honor the memory of Mary, liveson. Mary Greeley has grown with the region it serves and playsa vital role in the health of Ames and surrounding communities.PHYSICIANS 200Non-EmployedPREFACE: ORGANIZATIONAL PROFILEPhysiciansPost-Graduate, MD, DOVOLUNTEERS 500Non-specific; must completeorientation and competenciesVolunteersassociated with on(7.4-4)PurposefulWork(7.3-22; 7.4-3)i
P.1a(5) Regulatory Environment MGMC adheres to theIowa Code as well as all local, state and federal standards,regulations, and licensures as noted in Figure P.1-4.Figure P.1-4 Key Regulatory Agencies and AccreditationsLegal / RegulatoryHIPAAPrivacy and security of health information (Figure 7.4-10)EEOCNon-discrimination of employees (Figure 7.3-3)FLSAFair and equitable labor practices (Figure 7.3-3)Occupational Health and SafetyOSHAWorkplace safety (Figures 7.3-9; 7.3-11)CDCStandards for disease and infection control (Figure 7.3-12)P.1b(2) Patients, Other Customers and Stakeholders Keyhealth care market segments include a primary market (StoryCounty) and secondary market (Boone, Hamilton, Hardin,Marshall, and Greene counties). Patients are the key customersand are segmented as noted in Figure P.1-5. The keystakeholder is the community. Key requirements andexpectations are listed in Figure P.1-5.Figure P.1-5 Key Customer and Stakeholder GroupsKey Groups (andSegments)Key Requirements andExpectationsFigures 7.1(a)CommunicationFigures 7.2-2;7.2-3TimelyOPResultsQuality/SafetyIPPatients (Customer)P.1a(4) Assets MGMC’s main site is in Ames, Iowa, and hasover 570,000 square feet of building space on the main campus.In 2012, MGMC began a multi-phased construction projectthat included a new, six-story patient care tower, new powerplant and data center, a covered sky walk, and an expandedemergency department and ambulance garage. Phase 1 (newinpatient tower) was completed in April, 2014, and phase 2(lobby, skywalk, ED and ambulance garage) was completedlate 2016. MGMC is committed to its mission of advancinghealth and as such, in 2008 decided to collaborate with partnerMcFarland Clinic in the purchase of a shared Electronic HealthRecord (EHR). This integrated EHR operates a fullcomplement of applications to support the delivery of patientcare services for both inpatient and outpatient/ambulatory careand provides MGMC with a competitive advantage in the carecoordination process (Figure P.2-3, SA1). MGMC does nothave any patents.P.1b Organizational RelationshipsP.1b(1) Organizational Structure MGMC is governed by afive-member elected Board of Trustees (BOT). The MGMCBOT oversees and supports the strategic direction for theorganization as well as provides oversight of quality outcomesand physician credentialing and privileging. The President &Chief Executive Officer (CEO) reports to the BOT. Seniorleaders reporting to the President include the Chief FinancialOfficer (CFO), the Chief Nursing Officer (CNO), the VicePresident of Clinical and Support Services, and the VicePresident and Quality Improvement Officer. Leaders managers and they report to their ‘one-up’ (i.e.directors report to VP’s, supervisors/managers’ report todirectors). The structure of MGMC’s leadership system (Figure1.1-1) is rooted in the PDCA methodology and the philosophyof managing for daily improvements (1.1c(1)).CommunicationFigures 7.2-6;7.2-7; 7.2-8TimelyEDHomeHealthStakeholderRecent changes to MGMC’s workforce composition includethe need for adequate capability and capacity of the workforceto support our vision. Ames, Iowa has one of the lowestunemployment rates in the country (Ames 1.2%; Iowa 2.7%, and national 4.1%), and must compete with otherbusinesses for staff (capacity). Changes in workforce needscontinue to be related to our employed workforce, specifically,our drive to increase the percentage of BSN prepared nurses.Research proves that patients experience fewer complicationswhen the majority of nurses providing their care are preparedat the baccalaureate level. To date, more than 50% of our nursesare BSN prepared (from 30% in 2011; Figure 7.3-7).Keydrivers that engage the workforce in achieving MGMC’smission and vision are listed in Figure P.1-5 and weredetermined as described in 5.2a(2). MGMC does not have anyorganized bargaining units. Workforce special health andsafety requirements are described in 5.1b(1) and Figure 5.1-3and 6.2c(1).CommunityCare CoordinationFigure 7.2-10Care of the Patient (carecoordination)Figure 7.2-12CommunicationFigure 7.2-14Improved outcomesFigures 7.1aCost effectiveFigures 7.4-14;7.5-5P.1b(3) Suppliers, Partners, and Collaborators Key suppliers,partners, and collaborators and the role they play in theorganization are described in Figure P.1-6.Accreditation and LicensureTJCDNVStandards for business, clinical, and facility safety andaccreditation (Figure 7.4-8)Standards for business, clinical and facility safety andaccreditation. (Figure 7.1-31)Financial and EnvironmentalCMSMedicare/Medicaid billing (Figure 7.4-8)EPAEnvironmental impact (Figures 7.4-11; 7.4-12 )Mary Greeley Medical Centerii
Figure P.1-6 Key Suppliers, Partners and CollaboratorsRole in InnovationKey Supply NetworkRequirementsSuppliersMechanism of Two-WayCommunicationSupplier of medicaland non-medicalsupplies,equipment,serviceProvide cost effectivesupplies (SA1, SA2)Group purchasing power;cost effective (SA1)Quarterly business/SLAreview; on-site meetings;national vendor meetings;board memberIdentify waste reduction;standardize inventory;negotiate new and improvedpricingTimeliness, availability, costeffectiveness, expensereduction Figures 7.1cPartnersRole in EnhancingCompetitivenessFormal contract withclinic (McFC) todeliver direct patientcareProvide superior care toachieve excellent clincialoutcomes; enhance carecoordination (SA1, SA3)Medical staff directorshipmeetings; SLA review;member of SPTFSupport improvementefforts through RIE & VSM;support use of best practicesthrough protocol driven careEffective and efficientclinical care delivered;Figures 7.1a,bCollaboratorsType and Role inWork SystemBusiness leadersproviding intermittentsupport to those whoprovide careLocal colleges anduniversities providingintermittent support foreducational prioritiesof the workforceRecruiting businesses toarea; support for localhealth careMember, chamber board;economic developmentmember; communitycollaborationOngoing support for studentlearning during practicum &preceptorships; nurseresidency; on-site RN toBSN programCollaborate on plan designto create steerage to MGMCto reduce overall healthcarecostsUse of technology tosupport on-site experience;collaborate on identifyingcreative solutions to increaseRN to BSNCost effective pricing;Figures 7.4-14; 7.5-5Student nursing pool;evaluate student nursesduring practicum; exposeMGMC to new graduatenursesP.2 ORGANIZATIONAL SITUATIONP.2a Competitive EnvironmentP.2a(1) Competitive PositionMGMC is the largestindependent medical center in its primary and secondarymarkets and has established itself as the market leader througheffective strategic deployment of its mission and vision, acommitment to performance excellence, and successfulworkforce management. Based on the 2018 Iowa HospitalAssociation database (the most current, available data),MGMC’s size and market share compared to its keycompetitors is listed in Figure P.2-1. Growth of MGMCcompared to market segments is noted in Figures 7.5a(2).Figure P.2-1 Market ShareProviderMGMCMercy Des Moines(DSM)UnityPoint Des Moines(DSM)MarshalltownNumberBedsPrimary Secondary Market(6 59.7%15.4%objectives of the Value Based Purchasing (VBP) program(Figures 7.1a and 7.2a(1)) so that alignment of these efforts isachieved. Additionally, changes in the way healthcare is beingdelivered (shift from IP to OP) and reimbursed which willpresent both strategic challenges (Figure P.2-4) and strategicopportunities (also 2.1a(2)) for MGMC.P.2a(3) Comparative Data Key sources of comparative andcompetitive data, including those from within thehealthcare industry and those outside the healthcareindustry are listed in P.2-2Figure P.2-2 Comparative and Competitive DataData SourceMeasureCMS/HCAHPS(HC)Patient engagement andclinical quality metricsMarket share; Cost forservicesCore measures forprocess of careFull Time Equivalent(FTE) and operationaleffectivenessIHA (HC)Press Ganey (HC)Premier OperationsAdvisor (HC)OSHA (HC NHC)Key competitors within a 35-mile radius of MGMC.NDNQI (HC)MGMC collaborates with local and state leaders andorganizations to further its mission and to address its strategicchallenges and opportunities. MGMC’s commitment to alearning environment coupled with the requirement forbaccalaureate-prepared nurses resulted in a collaborativearrangement with Iowa State University to offer a new RN-toBSN program on their campus. To support efforts to increaseBSN-prepared nurses by 2020, MGMC’s Foundation providesscholarships to students in need. To date, MGMC has increasedthe percent of BSN prepared nurses (Figure7.3-7) whichexceeds its goal.P.2a(2) Competitiveness Changes Key changes taking placethat affect MGMC’s competitive situation include increasedpressure to efficiently and effectively coordinate care andmanage outcomes. MGMC’s SP incorporates the goals andMary Greeley Medical CenterSafe and effective carethrough increased nursingeducation; Figures 7.3-6,7.3-7, 7.3-8NHSN (HC)IHC (HC)Moody’s & Poor(HC NHC)NRC (HC NHC)Workforce safetyExample Results7.2-20; 7.2-247.5-5 through 7.5-97.1aLeader BusinessReviews (1.1c(2))7.3-8; 7.3-9Nursing practicemeasuresHospital AcquiredInfectionsHospital EngagementNetwork7.1-26; 7.3-6; 7.3-7Financial metrics7.5-1 through 7.5-4Patient engagement7.2-3 through 7.2-117.1-9 and 7.1-107.3-12Provider engagement7.3-23; 7.3-24Employee engagement7.3-17; 7.3-18HC healthcare; NHC other industry/non-healthcare **cycle of learning tothe processDuring the 2019 SPP, MGMC defined what being the bestmeans and determined this to be ‘incremental and sustainableimprovements in our performance.’ For MGMC, its vision Toiii
SC1Declining payment, payment change, consumer driven care, andnon-traditional competitors.SC2Increasing behavioral healthcare needs.SC3Alignment with our physicians to continuously improve value.SC4Workforce capability and capacity.Key Strategic AdvantagesSA1SA2SA3SA4Most comprehensive medical center in six county service area.Lean transformation and PI broadly deployed resulting in processdiscipline.Key partners clinic network, and referral loyalty to MGMCresulting in a high degree of confidence in the community.Highly engaged staff and educated board of trustees.Strategic Opportunities (2.1a(2))SO1Develop partnerships to improve models of care.SO2Leverage our quality, safety and patient experience results tomaintain and develop markets.SO3Be the convener to support community health.P.2c Performance Improvement SystemThe Leadership System (Figure 1.1-1) provides the overalldirection for performance improvement at MGMC. Thissystem, as well as all systems at MGMC, are aligned with thePerformance Improvement Model (Figure 6.1-1) and thePDCA method which supports a framework and culture ofcontinuous learning and performance improvement. In 2017MGMC adopted the DMAIC method (Figure P.2-3: Define,Measure, Analyze, Improve, Control) to support data-drivenperformance improvement efforts and to enhance sustainabilityof improvements. Combined, the PDCA and DMAIC modelscreate a robust, systematic approach for improvement andinnovation. Adding DMAIC allows MGMC to be moreintentional about data collection and establish baseline metricsin the early stages of improvement (define, measure).Additionally, the control phase adds focus on sustainabilitythrough ongoing metric review and systematic deployment ofbest practices.Mary Greeley Medical CenterPlanKey Strategic ChallengesDoFigure P.2-3 Strategic Challenges, Advantages, OpportunitiesFigure P.2-3 PDCA & DMAIC Method – Standard Work forImprovement & Innovation Events (6.1a(1); Figure 6.1-1) Pre-work meeting to discuss project What is the goal of the project? Strategic Initiative this project supports? Complete charter; define scope, problemDefine Identify participants including wild card Select dates for project Identify metric(s) for project Determine future state opportunity BI - Data-mining /collection of current state ** Conduct observations if necessaryMeasure Identify source for benchmarks/comparison Develop baseline report via data collection Project kick-off with full team Review scope of project with team Team develops purpose statementAnalyze Team maps out current state Team ‘goes to see’ the process/work FMEA & team selects opportunities Works key opportunities into system Create & test Standard Work to supportImprove improvement Conduct small test of change Monitor baseline metrics to determine improvement First Friday report out; sharing and learning Standardize new process Monitor metrics Celebrate winsControl Sustain through validation of Standard Work Deploy improvements as appropriate Post-event follow up with executive champion **CheckP.2b Strategic ContextKey strategic challenges and advantages, identified during theSPP, are listed in Figure P.2-3.Key elements of MGMC’s performance improvement systemare embedded in the philosophy that every employee has twojobs – 1) to do your work and 2) to improve your work. Thisphilosophy is further supported by a commitment to engageemployees closest to the work to design and redesign theirwork processes. Involving those closest to the work in thedesign and redesign of their work is a philosophy that creates arespectful work environment and one that fosters positivechange and supports innovation. The adoption of the MalcolmBaldrige Performance Excellence criteria, including acommitment to the ongoing self-assessment and annualapplication process at both the state and national level furthersupports a culture of continuous improvement. MGMCincorporates the feedback received into its performanceimprovement strategies through the Annual Action Planningprocess (2.1a(1)).ActBe the Best does not necessarily set the expectation that allresults will be at the national top decile. Rather, the visionframes benchmark selection to focus the organization oncontinually striving to get better every day. Where appropriate,MGMC compar
Amy Stark, RN. Pharmacy . Doug Wetrich, RPh. Supply Chain Management. Sue Draper. Inpatient Nursing Services/ House Managers Matt Aitchison, RN Outpatient Nursing Services. Jane Jackson, RN. Home Health/Hospice/ Public Health . Les White, RN. Chaplaincy Services. Katherine Werner. Rehab Inpatient Hemodialysis. Joelle Schmidt, RN. Medical .