Transcription
Shaun FixFlorida’s Premier Provider Of Quality Medical Training ProgramsNationally Accredited and OSHA ProgramsCEU ProviderSince 1988PHTLSPREPARATIONPACKET9th EditionNote: This packet contains the latest trauma guidelines, review information and pre-test. It ismandatory that participants review the textbook, complete the pre-test and be familiar with the PHTLSassessment and management criteria prior to the course. A pre-test score of 76% is required for thiscourse.The pre-test will be collected at the beginning of the class.Feel free to contact our office should you have any questions(772) 878-3085 * Fax: (772) 878-7909 * Email: info@medicaltraining.cc597 SE Port Saint Lucie Blvd * Port Saint Lucie, Florida 34984Visit Our Website MedicalTraining.cc
Pre-Hospital Trauma Life SupportDay 145 minWelcome, Course Intro, Collect Pre-test –Lesson 1 (Introduction)-45 min10 min60 min10 min60 min45-60min60 min30 min10 minStation 1:AssessmentLesson 2 (Scene Mgt & Primary Survey) –BREAKLesson 3 (Airway)BREAKLesson 4 ( Breathing, Ventilation & Oxygen)LUNCHLesson 5 (Circulation)Lesson 6 (Secondary Survey) –BREAKSkills Stations- 40 minutes eachSkills-PHTLS AssessmentSequenceCaseBaseline 1 & 2(Practice full PHTLSsequence)-Helmet Removal(Sports, Motorcycle)-PerilaryngealsAirwaysStation 2:AirwaySkills-Jaw Thrust (chin lift 2rescuer)-OPA,NPA-BVM – 1 & 2 personCaseAirway Case 1, 2(OPA & NPA)Airway Case 6(Trauma ET)Airway Case 8 (Cric)-Trauma Intubation(Neutral C-Spine, frontal,bougie)-CricothyrotomyStation 3:Bleeding Control &Breathing ControlSkills-Plural Decompression-Tourniquet-Wound packing(Hemostatic agents)ENDCaseBreathing Case 1(Decomp)Circulation Case 1Circulation Case 5Circulation Case 5N
Pre-Hospital Trauma Life SupportDay 260 minLesson 7 Part 1 (Disability- Brain Injury)-10 min60 min10 min60 min45-60 min60 minBREAKLesson 7 Part 2 (Disability- Spinal Trauma)BREAKLesson 8 (Special Considerations)LUNCHLesson 9 (Summation)-Station 1:Final Scenario Evaluations- 40 minutes each(Each student is team leader in 1 caseCaseSkillsReview RapidSpecial Case 2, 6 & 14ExtricationStation 2:SkillsCaseReview IO for TraumaMulti Trauma 1, 2, & 3SkillsCaseReview Traction SplintReview Pelvic BinderMulti Trauma 4, 5 & 6Circulation Case 4 (Pelvic)Station 3:60 minWritten Exam
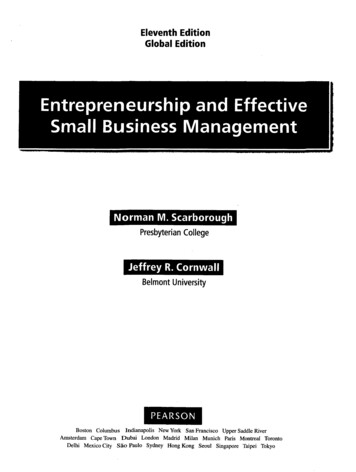
Prehospital External Hemorrhage Control ProtocolApply direct pressure/pressure dressing to injuryDirect pressure effective(hemorrhage controlled)Direct pressure ineffective or impractical(hemorrhage not controlled)Wound amenable totourniquet placement(e.g. extremity injury)Apply a tourniquet*Wound not amenable totourniquet placement(e.g. junctional injury)Apply a topical hemostatic agentwith direct pressure#Pack wound if necessarySpine Board DebateIt is agreed that the long board is an appropriate device for extrication and patient movement on scene and to astretcher, but 2015 brought about documented controversy as to its effectiveness at truly immobilizing the spineand its benefits; Key Issues:- There are no documented studies to support that straight rigid board immobilization with a collar isbeneficial.- Some patients’ anatomy actually flexes the head forward while others hyperextend the head when placed ona board.- Patients will all begin to complain of neck and back pain if left on a hard board.- Skin breakdown can occur at points that contact the board.- Obese patients are at risk for positional asphyxia- Emergency airway procedures are more difficult to perform on immobilized patientsThe lack of supporting benefit and the growing potential for detrimental side effects has led many areas to decreaseor completely remove the use of spine boards for anything more than extrication or movement. Instead opting forplacing a collar on the patient and lying the spine on the stretcher.*Some protocols for ruling “in” or “out” the use of spinal immobilization are still utilized.
PHTLS ShockThere are three types of shock: Hypovolemic shock Vascular volume smaller than normal vascular size Loss of fluid and electrolytes Dehydration Loss of blood and fluid Hemorrhagic shockDistributive shock Vascular space is larger than normal Neurogenic “shock” (hypotension) Psychogenic shock Septic shock Anaphylactic shockCardiogenic shock Pump failureClassification of Hemorrhagic ShockClass IClass IIClass Mildly Decreased30-405-15Anxious, confusedCrystalloid and bloodClass IVBlood loss (mL)Blood loss (% vol)Pulse rateBlood pressurePulse pressureRespiratory rateUrine output (mL/hr)CNS/ mental statusFluid replacementUp to 750Up to 15% 100NormalNormal or increased14-20 30Slightly anxiousCrystalloid 2000 40% 140DecreasedDecreased 35NegligibleConfused, lethargicCrystalloid and bloodVital SignSkin temperatureSkin colorBlood pressureLevel ofconsciousnessCapillary refillingtimeHypovolemicCool, clammyPale, cyanoticDropsAlteredNeurogenicWarm, dryPinkDropsLucidSepticCool, clammyPale, mottledDropsAlteredCardiogenicCool, clammyPale, cyanoticDropsAlteredSlowedNormalSlowedSlowedSigns Associated with Types of ShockShock AssessmentVital atedGreatly increased;marked tachycardiathat can progress tobradycardiaSkinWhite, cool, moistWhite, cold waxyBlood pressure rangeNormalDecreasedLevel ofconsciousnessUnalteredAltered, rangingfrom disoriented tocomaType of FractureRibRadius or ulnaHumerusTibia or fibulaBlood Loss Potential125 mL250-500 mL500-750 mL500-1000 mLFemurPelvis1000-2000 mL1000-unlimited mLManagement-Ensure oxygenation and ventilation-Control hemorrhage (external or internal)-External- direct pressure or tourniquet or homeostatic agent-Internal-direct pressure (extremity immobilization/ PASG for pelvis/ low abd.)-Move toward a definitive facility-Control body temp (lower the pt)-Fluid replacement for Class II, III, or IV shock-Isotonic crystalloids (lactated Ringers preferred; warm if possible)-Ideally blood or packed RBC’s (now being used prehospital)-Controllable bleeds- 1-2 liters (adult) (20 mL/kg peds) – Titrated to SBP 80-90 mmHg-Uncontrolled (internal) bleeds- the least amount of fluid required to maintain SBP 80-90 mmHg
PHTLS 9th Ed. FINAL EVALUATION STATION FLOW SHEETStudent (Leader):Evaluator:Beginning Time:Scenario Number:Ending TimeCompletedYesNoAssessment & TreatmentIdentify Safe SceneProper Standard PrecautionsPerform Primary SurveyLevel of Consciousness/ResponseX – Stop Exsanguinating hemorrhageAirwayBreathingVentilation/Air ExchangeCirculation/PerfusionExternal Hemorrhage ControlPulseSkin ConditionDisabilityExposure of All Critical Body Areas for AssessmentProperly Identify Critical and Non-Critical Trauma PatientsUse of Appropriate Spinal Immobilization Technique(s)NOTES:Proper Use of Padding/Buttress MaterialIdentification of All Life-Threatening InjuriesProper Treatment of All Life-Threatening InjuriesPerformed Only Lifesaving Treatment(s) While On-SceneTimely Transported When IndicatedAppropriate Level Trauma Facility When IndicatedIdentification of All Non-Critical InjuriesProper Treatment Performed En-RouteCompleted Secondary Survey When IndicatedCompleted Scenario Within 10 Minutes On-Scene TimeReassessment of Patient's ConditionsSafety Observed Throughout ScenariosWorked Together as A TeamSuccessful Station Completion: YESNO
Sample Scenario Evaluation Skill StationInstructor InformationPatient InformationThis skill station involves a skier who lost control while skiing. Thepatient’s LOC is altered and he requires airway management and rapidtransport. Follow the written scenario, and provideinformation to all team members as the scenario progresses or as the teammembers ask.Moulage: Pale and diaphoretic, cyanotic lips and nails, multiple bodyabrasions, blood at mouthPosition: Laying on his side in a basket stretcherActions: Eyes open to pain, incoherent moaning, and withdraws frompainDispatch InformationYou and your partner work for a rural emergency medical service. Your ambulance has been dispatched to a local ski resort for a skiing accident in a remotesection of your response area. It is noontime in late winter, clear sky with 17 F (–8 C). The closest hospital with an emergency department is 40 minutesaway by ground; the closest level I trauma center is a 60-minute ride by ground or 15 minutes by air ambulance.Scene Assessment/General impressionResort staff direct you to the first aid building. There you find three members of the ski patrol and the patient’s wife. The ski patrol packaged the patient andmoved him to the aid station at the base of the hill. No interventions have occurred. The ski patrol reports the patient lost control and tumbled into trees. Theyarrived 5 minutes after the accident and his condition has not changed. The accident happened 20 minutes ago. Copyright 2020 National Association of Emergency Medical Technicians (NAEMT). *Course materials are developed by NAEMT for the sole purpose ofconducting NAEMT education courses and may not be utilized for any other purpose.*Primary SurveyTreatments/Critical Actions31-year-old male, approximately 270 lb (122 kg); patient dressed inheavy winter clothing and ski boots*Note: icon indicates a Critical ActionX: No major external hemorrhageA: Partially obstructed—gurglingB: Rapid and shallowC: Fast radial pulse, skin pale and clammyD: 8 (E-2, V-2, M-4), PERRLA, moves all four extremitiesE: Various small abrasions on hands, knees where the ski suit ripped,blood at mouth Initial Patient Impression:BP:112/72 (MAP 85)GCS:8 (E-2, V-2, M-4)Temp:98.8 F (37.1 C)Critical/Rapid TransportSpinal motion restriction Manual opening of the airway with suctioning of theoropharynx Insert NPA and assist ventilations with high-flow oxygen and bagmask Drug assisted intubation if within scope of practice Rapid transport to trauma center, request air medicaltransport Maintain body heatIV during transport to maintain BP at 90 mm Hg systolic
Sample Scenario Evaluation Skill StationReassessment Vital SignsCritical actions doneCritical actions NOT doneBP:126/74 (MAP 91)BP:92/60 (MAP 71)P:130, weakP:150, weak, rapid, irregularR:20, assistedR:8, irregularSkin:Pale, cool, clammySkin:Cyanosed, cool, clammySpo 2:94%/O 2Spo 2:90%/O2GCS:8 (E-2, V-2, M-4)GCS:4 (E-1, V-1, M-3)Glucose:90 mg/dl (5 mmol/l)Glucose:90 mg/dl (5 mmol/l)etco2:38 mm Hgetco2:60 mm HgPain:Unable to obtainPain:Unable to obtainTemp:98.8 F (37.1 C)Temp:98.8 F (37.1 C)SampleSigns/symptoms:Reduced LOCAllergies:Penicillin (per wife)Medications:NonePast medical history:Back surgery 8 years ago (per wife)Last oral intake:Breakfast, 3 hours agoEvent leading to incident:SkiingTransport and DestinationHead:Obvious deformity and bleeding from jawTransport Timing: Emergent/RapidNeck:Unremarkabletransport Destination: Trauma centerChest:Equal, bilateral breath sounds and shallowAbdomen:Soft, nontenderDiscussion PointsPelvis:Stable Extremities:Abrasion of hands and knees, scant bleedingBack:Unremarkable What are the basic and advanced methods to maintainan airway?Are there any perceived complications with the coldwinter gear the patient is wearing?
NAME:PLEASE DO NOT WRITE ON EXAMCOURSE: PHTLS 9TH EDITION PRE-TESTHERE# MISSED:1. A B C D E2. A B C D E3. A B C D E4. A B C D E5. A B C D E6. A B C D E7. A B C D E8. A B C D E9. A B C D E10. A B C D E11. A B C D E12. A B C D E13. A B C D E14. A B C D E15. A B C D E16. A B C D E17. A B C D E18. A B C D E19. A B C D E20. A B C D E21. A B C D E22. A B C D E23. A B C D E24. A B C D E25. A B C D EGRADE:RECORD PRE-TEST ANSWERSTHIS SHEET WILL BE COLLECTED
PHTLS 9th Edition Pre-testPlease record your answers on the answer sheet provided.1. A roofer is found on the ground following a fall. He is alert, but complaining of acuteshortness of breath. Breath sounds are absent on the left. Which of the followingindicators is generally not a sign of tension pneumothorax?a) Subcutaneous emphysemab) Bradycardiac) Distended neck veinsd) Tracheal deviation away from the site of injury2. A 19 y.o. male was an unrestrained passenger in a 2 car collision. He is evaluated forselective spinal immobilization. Which of the following signs might point towards theneed to immobilize?a) Skin breakdownb) Obvious presence of a Colles’ fracturec) Altered level of consciousnessd) Tenderness in bilateral hip areas3. When cells are deprived of adequate oxygenation, the short term backup system thatcan fuel the body using stored body fat as the energy source is called:a) ATP molecular systemb) Anaerobic metabolismc) Ketogenesisd) Aerobic metabolism4. Patients with a TBI (traumatic brain injury) are challenging to treat and transportsafely. Which of the following clinical markers is not considered to be an extracranialcause of secondary brain injury issues?a) Anemia from blood lossb) Hypotensionc) Hypoxiad) Coup-countercoup injury5. When treating a trauma patient, tools such as bag mask, IV fluids, and a back boardto achieve a goal are called:a) Preferencesb) Tactical carec) Principlesd) Action Intervention
6. Receiving a call to a situation where many people are suffering from similar toxicsymptoms from a chemical leak gives the responder some insight as to whatadditional protective gear may be needed. This is an example of:a) Pre arrival assessmentb) Care alteration strategyc) Triaged) Unified command7. A 63 y.o. gunshot victim is found to be unresponsive to stimuli with obviousasymmetric pupils. Extensor posturing is noted. What would be the preferred rate ofventilation in this individual until capnography is available?a) 15 b.p.m.b) 20 b.p.m.c) 10 b.p.m.d) 30 b.p.m.8. A victim of chest stabbing injury has an open pneumothorax. An occlusive dressingwas applied at the scene. During transport, the patient develops a sudden episode oftachycardia and respirations increase to 44. What should your next action be?a) Intubate with rapid sequence inductionb) Perform an emergency cricothyrotomyc) Release and re
PHTLS PREPARATION PACKET 9 th Edition Note: This packet contains the latest trauma guidelines, review information and pre-test. It is mandatory that participants review the textbook, complete the pre-test and be familiar with the PHTLS assessment and management criteria prior to the course. A pre-test score of 76% is required for this