Transcription
Increasing Self-Esteem and School ConnectednessThrough a Multidimensional Mentoring ProgramKeith A. King, Rebecca A. Vidourek, Beth Davis, Warren McClellanABSTRACT: Hi h levi'l.s of self-estecrn and po.-iitive sthool. peer, and family connec lions represent protective far. tors against youthinvolvement in riskv lyi'havior. This paper reports findin .s from year one of the Healthy Kids Mentoring Program, a multidisciplinarynienloniig pr i: ram for fourth-grade students in a Midwestern public school. In October 200(1. 2Hfourih-grade students were admittedinto the program, based on findings from a 5.' -ilem surrey distributed to all fourth-grade sUtdcnis CV 2.?*.?; regarding overall setjesteem, school, peer, and family coniierledne.ss and involvemem in risky behavior. The program, which ran from January 2000 lo May2000. consisted of four components: 11 relationship imilding, 2) self-esteem enhancement, M goal setting. 4) ucademic assistant e.Prctest-Posltcsi data showed significant improvements at posttcsi in mentored students' sclf-esieem levels and positive connt'ctions tosihool, peers, andfumily. Mentared stiidenis also were significantly less likely to be depressed or involved in bullying andfighiing iitpastiest than at prelesi, C 'otnpared to nonmeniored students, mentored students reported significantly higher school and familyloiinevledness scores ut posttest. Recommendations for effective mentoring program design are offered. (J Sch Hcalih.2002:72(7):244-29yiesearch indicates high self-esteem serves as a protectivefactor to youth involvement in risky health behavior.' *High self-esteem is associated with high academic achievement, involvement in sport and physical activity, and development of effective coping, und peer pressure resistanceskills." Conversely, low self-esteem is associated withyouth involvement in alcohol, tobacco, and other drug use;depression; suicide; violence; early sexual activity; teenage pregnancy; and poor peer relationships.'''- In the schoolenvironment, high levels of self-esteem increase the likelihood Ihat youth will connect positively to peers, teachers,and the school as a whole, important determinanls of academic success.'-''Similar to self-esteem, a sense of positive school, peer,and family connectedness (feeling that one "fits in" and"belongs") protects youth from engaging in negative healthbehavior."'""" Positive social connections decrease risklaking behavior by providing youth with prosocial andempowering opportunities."" Youth who feel supportedand cared for by parents, teachers, and peers report feelingmore efficacious in making healthy, informed decisions anddisplaying features of resiliency to potential life stressors."*Students spend a large portion of their time in school, soschool-based health education and prevention programshave been implemented to increase youth self-esteem andpositive school, peer, and family connections. Theseprograms focus on getting students involved in interactive,student-oriented, decision-making, cooperative learningactivities, as well as including aspects of parental involvement, peer counseling, tutoring, and mentoring.'"The specific aspect of mentoring involves pairing anadult or youth with a student needing assistance.'" The overarching goal of most meiitoring programs is to reduce riskybehavior while connecting the youth in need to an individual lrom the school or community.'"" The mentor serves asa positive role model while providing emotional and socialRKeilh A. King, PhD, CHES, As.\isiant Professor, Health Promotion andEducation Program, University oj (incinnaii. Ml. 0002. 526 IC,Cincmnali, OH 45221-0002; (keith.king( huc.edu]: Rebecca A. Vidourek,BEd, Researih Assistant, fleatlh Promotion and luhicalioii Program,iiniver.sirv of Cincinnati. ML 0002, 526 TC, Cincinnati, OH 45221-0002:Iteth Davis, MS, Projeci Coordinalor, Healthy Kids - It's My lime,Cincinnati, OH; and Warren McClellan, MEd, Principal, l.ovelandIntermediate School, Cincinnali, OH. this article was subniilled .lamiaryJ, 2002, and revised and accepted for publication Mti\-2H, 2002.support and academic assistance. While mentoringprograms can have beneficial effects, unfortunately asubstantial percentage of these programs point solely toanecdotal evidence to support their overall effectiveness.Furthermore, preventive interventions often occur in themiddle or high school years, despite the fact that earlyinterventions may prove more effective in preventingcurrent and future negative health behavior.-' Early interventions are critical to preventing future health problems.Nevertheless, few evaluative studies on elementary schoolmentoring programs have been published in the professional literature.This exploratory study was undertaken to determineoverall effectiveness of the Healthy Kids MentoringProgram in fostering high levels of self-esteem and positiveschool, peer, and family connections. Due to theexploratory nature of the study, readers are encouraged toview this paper as an overall program description andprocess evaluation with preliminary findings. If successfulprogram results were found then future youth engagementin negative health behaviors may be prevented and childhealth status may be improved.METHODSProgram DescriptionThe Healthy Kids Mentoring Program, designed forfourth-grade students at a Midwestern suburban publicschool, consisted of four components: 1) relationship building, 2) self-esteem enhancement, 3) goal setting, and 4)academic assistance (tutoring). Mentors met with studentstwice each week for VA hours each session on schoolgrounds. During each meeting, mentors devoted time toeach program component.Relationship Building. To develop a positive relationship with a student, mentors were instructed to use dialoguejournals and continuous meeting icebreakers. Each week,mentors read one question (provided by the program coordinator and evaluator) in a dialogue journal, replied by writing their answers and thoughts in the joumal, then passedthe journal on to the student they were mentoring at thenext mentoring session. Examples of dialogue questionsincluded, "What are you most proud of having accomplished?" "What is the bravest thing that you ever did?""Who are your heroes and why?" "What is the hardest294 Journal of School Health September 2002, Vol. 72, No. 7
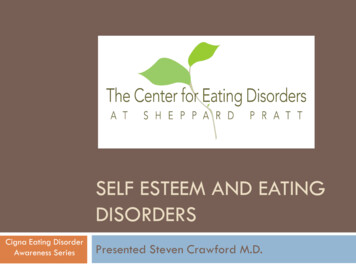
thing about growing up?" Students read the mentors'responses, answered the question themselves, an.swered anyquestions the mentor posed for them, then posed a questionTor Ihe mentor to answer. Mentors and students used thejoumaj to communicate and learn more about each other.Mentors also received descriptions oi several smallicebreakers to use with the students in the program. At thebeginning ot each mentoring se,s,sion, mentors conducted abrief icebreaker to foster positive connections betweenmentor and student. Examples included "My unique characteristics," "Discussion of your three wishes." and"Important things about myseif."Self-Esteem Enhancement. Mentors received a guidebook ol self-esteem enhancement activities to use with thestudents they were mentoring. The activities were developed based on Ihe four conditions of self-esteem: sense ofconnectedness. sen,se of power, sense of" uniqueness, andsense of positive role models. Mentors were encouraged tochoose activities they believed would prove most suitableand effective for the child, while ensuring tliat at least oneactivily was chosen from each of the four self-esteemconditions. Examples included "Developing a Me Poster,""Writing a Name Poem," and -Construeting a Happiness is,, Booklet."Goal Setting. During the first mentoring session of eachweek, students worked with mentors to develop a goal theywould try to accomplish that week. Examples of goalsmcltided completing all homework as assigned, answeringa question in class, complimenting a peer, thanking ateacher or parent for their help, and developing a list ofcharacteristics of a positive friend. Mentors assistedstudents m developing their weekly goals by ensuring thegoals were measurable, realistic, and obiainable. Eachweek, a goal agreement form was completed by studentsand their mefitors. The (onn mcluded the date the goal wasdeveloped, target completion date, actual goat, why thestudent wished !o complete this goal, and signattires of thestudent, mentor, and parent/guardian.Academu Assistance. Students in the program often haddilhculty in the spL-cific .school subject of reading.Therefore, mentors were encouraged to spend 15 to 30pninutcs each ses.sion helping students complete assignedreadings and study assigned vocabulary/spelling words Toensure consistency with academic assistance, mentorsreceived training sessions as well as guides on strategies tomcrease reading and academic skills. '' ' The program coordmator personally contacted mentors bimonthly to addressgoals, strategies, and potential difficulties, and to maintainconsistency and integrity of the program.Mentor Recruitment and Trainingrn November 1999, 32 mentors were recruited from thecommunity where the school was located. Mentors rangedfrom high school students to senior citizens. In December1999, mentors received initial training regarding theprogram specifics by the program coordinator, school principal, and project evaluator. In this initial training session,the four program components were delineated clearJy'examples were provided, mentor behavioral expectationswere set, legal i.s.sues were discussed, and questions weretaken. Mentors received a program guidebook that providedthem with examples of activities to engage in with studentsto enhance self-esteem and foster a positive relationship.Mentors also were encouraged to use a dialogue journalwith students to help develop the mentoring relationship.In December 1999, mentors received a second programtraining session. An expert in literacy education from anearby university provided effective strategies mentorscould me lo help student.s become more interested in readmg, as well as to improve their reading skills. A guidebookof practical reading enhancement strategies was provided toall mentors and to the school library.Program Coordinator ResponsibilitiesThe program coordinator's role was critical in effectively delivering the mentoring program. This individualhad extensive experience in health education and mentonngof children. The coordinator worked collaboratively withthe program evaiiiator lo develop the program and setprogram expectations. Meetings between the coordinatorand evaluator were conducted to ensure consistency amongprogram leadership, delivery, and desired outcomes Thecoordmator provided ongoing contact and support withparents by email messages, telephone conversations andface-to-face meetings. This individual also served as a liaison between parents and school, parents and mentormentors and students, and the school and the evaluatorTable 1Impact of Healthy Kids Mentoring Programon Self-Esteem, School, Peer, and Family ConnectednessNumberof ItemsSelf-EsteemSchool ConnectednessPeer ConnectednessFamily ualRange'15-209 4.517,6- Actual ranges based on posttest scores" - Mean scores based on a four-point Likert-type scale (1 strongly disagree, 2 disagree, 00agree, 4 strongly agree)Joumal of School Health September 2002, Vol. 72, No. 7295
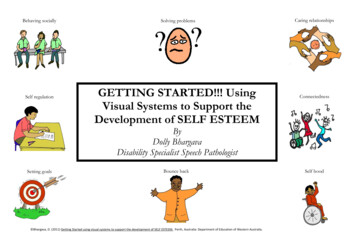
InstrumentA four-page, 55-item survey instrument was developedbased on a review of the literature lo measure students'overall self-esteem: school, peer, and family connectedness;and involvement in unhealthy behavior. Four subscaies(sell-esteem, school connectedness, peer connectedness,family connectedness) were assessed using a modifiedversion of the Hare Abbreviated Self-Esteem sciile. * Eachsubscale consisted of five self-esteem items and requiredstudents to respond by using a four-point Likert-type scale(1 strongly disagree, 2 disagree, 3 - agree, 4 stronglyagree).Students' involvement in unhealthy behavior wasassessed by 35 items that addressed a variety of healthbehaviors including nutrition (n 9); physical activity (n 2); hygiene (n 3); sufcty (n 5); violence (n 5); depression (n - 2); alcohol, tobacco, marijuana, and inhalant use(n 6); and communication with adult role models {n - 3).Health behavior items were formatted similarly lo the YouthRisk Behavior Survey.'' Nutrition, physical activity,hygiene, and safety items were not used for student entryinto the program but to gain overall information ahoutstudenl behavior for use later by the school.Violence, depression, and substance use items were usedas criteria tor program admission. Students were requiredto indicate their recent involvement in weapon carrying,weapon carrying on school grounds, bullying, beingbuflied. physical fighting, and depression by circling theappropriate number of days they engaged in such behaviorthe past 30 days. Stjbstance use items measured lifetime useof alcohol, tobacco, marijuana, and inhalants (yes or no)and recent use (use in the pasi 30 days). Students also wererequired to state how frequently they talked to aparent/legal guardian, aduit at school, and/or friend whenthey had a problem by using a five-point Likert-type scale(I never, 5 - always).Stability reliability (test-retest reliability) of the instrument was assessed by distributing the survey to a sample offourth-grade students (N 32) on two occasions one weekapart, yielding Pearson r correlation coefficients of .70 forhealth behaviors, .8.5 for self-esteem, .HI for schoolconnectedness, .73 for peer connectedness, and .73 forfamily connectedness. Intemal reliability of the instrumentwas assessed by computing Cronbach alphas for each of thesubscaies: .66 (health behaviors), .81 (self-e.steem), .80(school connectedness), .72 (peer connectedness), and .76(family connectedness).Student Admission into ProgramIn October ] 999, the survey was distributed to all iounhgrade students (N 283) at a midwestem suburban publicschool. Recent letter grades also were obtained for eachstudent. Data then were analyzed to identify students inneed and eligible for the mentoring program. Students inneed met one of the following conditions: I) had selfesteem scores at least one standard deviation below thegroup mean, 2) had engaged in two or more risky healthbehaviors, 3) had been sad or depressed for two consecutiveweeks in the past month, 4) had abused alcohol, tobacco, orother drugs in the past 30 days, 5) had failed two or moreclasses in the first academic quarter of 1999. Based onthese criteria, 32 students were selected for the program.These students met with the school counselor to validatetheir survey responses. All 32 students reported honestlyanswering the survey items. Parents of the students thenwere contacted lo gain consent for studenl admission intothe mentoring program. Parents of four students declined togrant consent. The remaining 28 students (11 girls and 17boys) received parental consent and were admitted into theprogratn.Evaluation ProceduresAll fourth-grade students completed the 5,'5-item surveyinstrument in October 1999 in their homerooms. Thesurvey items and instructions were read verbatim tostudents to increase internal validity of the evaluation byTable 2Comparison Between Mentoring Group and Control Groupon Self-Esteem Levels, and School, Peer, and Family ConnectednessSelf-EsteemMentor GroupContro! GroupSchool ConnectednessMentor GroupControl GroupPeer ConnectednessMentor GroupControl GroupFamily ConnectednessMentor GroupControl .90.85NS14.214017.614239.53.000N : 28 studentsMean scores based on a four-point Likert-type scale (1 strongly disagree, 2 disagree, 3 agree, 4 strongly agree)296 Journal of School Health September 2002, Vol. 72, No. 7
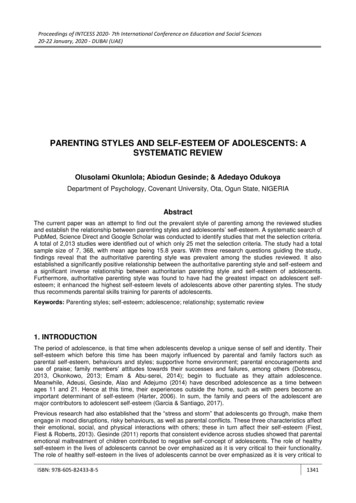
minimizing potential difficulties from student reading abilities. Students completed the survey as the proctor read eachquestion and possible scale responses. Students meetingthese criteria, and having parental consent, were admittedinto the program.The program began the first week of January- 2000 andended the last week of May 2000. In June 2000. all fourthgrade students (N 283) completed another survey (thesame instrument as the pretest) according to the samepretest administration procedures. An end-of-the-year celebration banquet was held at the school for students andparents in the program. Qualitative data regarding programeffectiveness was obtained from parents and students at thebanquet (parents of two students did not attend) and bypost-program telephone conversations conducted by theprogram coordinator.Data AnalysisDescriptive statistics, including frequencies, means, andstandard deviations, were used to examine demographicand background characteristics of respondents. Pairedsample t-tests were conducted to assess program impact onmentored students' self-esteem, connectedness, and engagement in risky health behavior. Analyses of variance(ANOVAs) examined parametric subscale data. All dataanalyses were performed by the Statistical SoftwarePackage for the Social Sciences (SPSS). Alpha level ofsignificance was set at .05 to reduce the likelihood ofcommitting a Type I error.RESULTSimpact of Program on Self-Esteem andConnectedness ScoresPaired sample t-tests were conducted to assess programimpact on mentored students' self-esteem and connectedness scores from pretest to posttest. Results indicatedstudents' overall self-esteem, school connectedness, peerconnectedness, and family connectedness were significantly higher at posttest than at pretest (Table I). A morespecific item-by-ivem display of pretest-posttest scores formentored students is presented in Table 2.To assess potential differences between the experimentalgroup (mentored students) and the control group (nonmentored students) a series of F-tests was conducted. Comparedto nonmentored students, mentored students achievedsignificantly higher school connectedness and familyconnectedness scores at posttest (Tahle 3). While mentoredstudents improved statistically from pretest to posttest intheir overaU self-esteem and peer eonneetedness scores,posttest scores in these two areas did not differ significantlyfrom nonmentored students' scores.Table 3Mentoring Students' Self-Esteem, Peer, School, and Family Connectedness ScoresSubscale ItemSelf-Esteem1 liKe myself1 feel there are many good things about me.1 feel proud of myself.1 feel confident.1 like the way 1 am.PretestM(SD)2,803 ,673,733,63(,47)(,48)(.45)(.49)Peer Connectedness1 have as many friends as others my age.1 am as popular as others my age.Other my age think ! am fun to be with.Other my age wish there were like me.1 am a person others turn to for help.2.37 (1.1)3,10 (,76)2.63(1.3)1.97 (1.1)1,57 chool ConnectednessMy teachers are fair with what they expect from me.1 am usually proud of my report card.School IS as hard for me as it is for most others.My teachers are happy with the kind of work 1 do.MosI of my teachers understand me.2.96(1,1)2,60 (1.3)2,82 (,92)2.40 (1,0)2.50 (.90)3.50 (,63)3.07 (1,0)3,23 (.94)3.27 (,58)2,83(1,2)Family ConnectednessMy parents are proud of the kind of person 1 am.My family pays attention to me at home.My parents try to understand me.1 am an important person to my family.1 feel wanted at home3,73 (.64)3,00 (.85)2,97(1,1)3,50 (.82)2,17 N 28 studentsMean scores based on a four-point Likert-type scale (1 strongly disagree, 2 disagree, 3 agree, 4 ; strongly agree)Journal of School Health September 2002, Vol. 72, Mo. 7 297
Involvement in Health BehaviorsPaired sample t-tests were conducted to assess programimpact on mentored students' involvement in risky behavior. Health behaviors assessed included current involvement(within the past 30 days) in weapon carrying; fighting;bullying; depression; and alcohol, tobacco, marijuana, andinhalant use. At posttest, mentored students were significantly less likely to have bullied a peer in the past 30 days.t(27) 3.47, p .002, to have physically fought with a peerin the past 30 days, t(27) 3.48, p .000, and to have feltdepressed, t(27) 2.97, p .006.Students also indicated how safe they felt at school byusing a four-point Likert-type scale (1 extremely unsafe,2 unsafe, 3 - safe, 4 extremely safe). Mentoredstudents were significantly more likely at posttest than atpretest to report feeling safer at school, t(27) - 3.47, p .002. Students also were asked to report how often they talkto their parent/guardian when they have a problem {1 never, 2 rarely. 3 - sometimes, 4 most of the time, 5 always). Data revealed that mentored students were significantly more likely at posttesl than at pretest to report talking more frequently with their parent/guardian when theyhad a problem, t(27) - 2.43, p .021.Academic AchievementAcademic grades for mentored students were evaluatedbefore and after program implementation. One criterion forentry into the program was to have failed two or moreclasses in the first academic quarter of 1999. The mentoringprogram began in the middle of the second quarter (January2(X)0). Fourth-quarter grades were compared against firstquarter grades to assess potential program effects. Ot 28students in the program, 20 students (71%) showed academic letter grade improvements from the first quarter. Ofthese 20 students, 18 improved their letter grades in reading. Seven students improved their grades in one to twosubject areas, while 13 students improved their grades inthree or more subject areas.DISCUSSIONResearch in school-based intervention indicatesprograms offering safe environments, encouragement andsupport, empowering activities, and specific guidelines forappropriate behavior contribute to increased self-esteem.'Mentoring programs that successfully incorporate suchaspects are associated with improved student attitudetoward school, healthier behavior, and fewer absences,detentions, and suspensions.""'-' School-based programscan enhance student self-esteem by focusing on academicachievement, and school, peer, and family connectedness.'''''"This exploratory study was conducted to as.sess theeffectiveness of the Healthy Kids Mentoring Program. Thefollowing limitations affect evaluation of the program.First, the program was delivered to elementary students atone suburban school district in southwestern Ohio. Resultsmay not generalize to other grades, schools, or programs.Future years of the program will focus on fourth- and fifthgrade students. Second, ihe control group may haveincluded randomly assigned students who were part of thementoring program after follow-up data collection tookplace. However, a ''delayed" control group as such stillwould lend itself to limitations of equivalence, because thecontrol group would not completely parallel the experimental group. Third, the control group may have been obtainedthrough random-assignment of students from a matchedschool. However, concerns of school-by-sehool comparisons restricted this type of sampling method. Finally,outcomes from this study may result from potential threatssuch as testing, maturation, and history. Thus, exercisecaution when attempting to generalize results from thisstudy.The Healthy Kids Mentoring Program produced significant increases in student self-esteem, academic achievement, and positive school, peer, and family connectedness.The program placed emphasis on building a relationshipbetween student and mentor, employing various icebreakersand self-esteem enhancement activities. Previous mentoringprograms often relied solely on the nature of the relationship to increase self-esteem.'" Healthy Kids is a uniquementoring program that specifically addressed these twocomponents on a weekly basis.Results from the Healthy Kids Mentoring Programrevealed that the program significantly affected students'sense of school and peer connections. The NationalLongitudinal Study of" Adolescent Health cited schoolconnectedness as the leading protective factor againstviolence, suicide, depression, substance abuse, early sexualinvolvement, and teen pregnancy."' Positive school connections prove critical to student engagement in healthy behavior. As noted, time and emphasis were devoted to buildingpositive school and peer connections among mentoredstudents. Mentors received an arsenal of icebreaker andrelationship-building activities to use with students.Offering mentoring sessions only on school grounds mayhelp students to direct positive feelings about the programtoward the school, thus improving their overall school attitudes." Continued support, care, and encouragement fromadults also helps produce more favorable attitudes.-"Interestingly, while the Healthy Kids program did notpossess a specific component facilitating peer relationships,mentored students reported higher levels of peer connectedness after the program. Positive peer relationships areimportant to the development and continued maintenanceof social, emotional, and mental well-being.'" Within thegoal-setting component of the Healthy Kids program, acommon long-tenn goal was to "make a lot of friends." Toaccomplish this long-term goal, mentors worked withstudents on communication skills, characteristics of qualityfriendships, and what it means to be a "good friend." Inaddition, short-term goals such as "complimenting at leastone peer today," "thanking one peer each day for his or herhelp," and "helping a peer to accomplish a task" may havecontributed to improved peer connectedness at the end ofthe year.Mentored students' sense of family connectednessimproved after program completion, perhaps due to a carryover effect from students spending four months conversingand developing a positive relationship with an adult mentor.In addition, mentors encouraged students to talk with theirparents about the program and about any problems theywere experiencing. The need to regularly communicatewith parents was a message continually delivered tostudents. Positive parental involvement represents an essential ingredient to healthy child growth and development"'"298 Journal of School Health September 2002, Vol. 72, No. 7
and, therefore, should become part of any mentoringprogram. Posttest data from this study revealed mentoredstudents as significantly more likely at posttest than atpretest to report talking more frequently with theirparent/guardian when they had a problem.The academic assistiince component of the Healthy KidsMentoring Program associated positively with significantgains in student achievement during the fourth quarter.Approximately 71% of students improved their grades.ITiese effects most likely occurred due to academic assistance and attention to students' feelings of connectednessand overall self-esteem. Positive student connections withschool and family are associated with improved academicachievement and school performance.' Mentors in theprogram set high but attainable acadetnic expectations withstudents, characteristics of authoritative teaching/parentingsiyles that enhance student learning and display of appropriate behavior.'' Improved self-esteem scores that occurredhave been associated with improvements in reading andacademic performance.'CONCLUSIONSBased on findings from this study, the following recommendations are offered to individuals interested in develop- ing effective school-based mentoring programs.1) Obtain and maintain administrative support.2) Devote resources toward creation of a mentor projectcoordinator. Advocate for a school health coordinator.3) Develop a multidimensional mentoring program thatincludes such components as relationship building, selfesteem enhancement, goal setting, and academic assistance.4) Recruit mentors from the community around theschool.5) Provide ongoing training sessions for mentors, andremain available for ongoing technical assistance.6) Obtain parental and community support.7) Keep parents informed about program events andprogress.8) During the planning phase, contact a program evaluator to help determine students eligible for the program, andto plan pretest-posttest analy,ses. References1. Youngs BB. Self-esieem in ihe school: more than a feel-gotid moveiiienl, NASSP Bull. 1993:76:5* 66.2. Brooks RB, Seil-cslCfm through the ,schaol years: Its normal developmcnl and hazardous dcctinu. Pediatr Clin North Am. l992;39:537-549,3. Lawrence D. Improving scit esfeein and reading, Educ ResIMS5;27:I94-2(H),4. Ourney P, Sell-esieem enhancement in children: a review of theliiidings. Educ Res. 1987;29:130-136."i, Torres R, em:ulde/ F. Maceira D- Self-csleem ami value of healthas correlates of atio it; seen! health behavior.Adolescence.l')95:3O(MS):4(13-4i2,6, Miller Rt,, Positive self-esteem and alcohol/drug relat(;d attitudesamong schooXchWAxcn.J Ale Drug Educ. I98fi;33(3):26-3I,7, Hershbergcr SL, Pilkington NW, D'Aiigelli AR. Predictors ofsiiicidL' attempts among gay, lesbian, and bisexual \outh, ,/ Adolesc Res.I'W: 12:477-497.5. Kaplan HI, SadLxrk BJ, Pocket Handbook of Clinical Psvchiatrv.R:iltimore, Md: William,s & Wilkins; 1990,y, Rc.sniuk MD. Bearman PS. Blum RW. c! al, ProieLling adolescentsInim hami: limiings from the National Longitudinal Siiidy on ,'\dQlescentHealth, JAMA, i997:27K:H23-K32,10, McDermott RJ. Saivela PD. Hoalt PN, Ba.irafharya SM. Marly PJ,Emery CM, Multiple LMH relates of cigarette use among high schoolstudents .1 Sch Health I M92:62:146-150,11, Hawkins JD, Catatano RF, Miller JY. Risk and protective factorsfor alcohol and other drug problems in adolescence and early adulthood:implications for substance abuse prevention. Psychol Bull. I992;112:64-105.12, Cole RL, Slocumb E
Self-Esteem Enhancement. Mentors received a guide-book ol self-esteem enhancement activities to use with the students they were mentoring. The activities were devel-oped based on Ihe four conditions of self-esteem: sense of connectedness. sen,se of power, sense of" uniqueness, and sense of positive role models. Mentors were encouraged to