![[Unlocked] Chapter 16: Psychological Disorders](/img/28/chap16-20psy.jpg)
Transcription
Psychology JournalWhat is a phobia? Write yourown working definition in yourjournal. Then describe somespecific phobia that you haveheard of. PSYCHOLOGYChapter OverviewVisit the Understanding PsychologyWeb site at glencoe.com and clickon Chapter 16—Chapter Overviewsto preview the chapter.446
What Are PsychologicalDisorders?Reader’s Guide Main IdeaPsychologists draw the line betweennormal and abnormal behavior in practice by looking at various attempts todefine abnormal behavior, adjustments,and psychological health. Vocabulary DSM-IV Objectives Define psychological disorder. Distinguish between the concepts ofnormality and abnormality.Exploring PsychologyNormal or Not?A man living in the Ozark Mountainshas a vision in which God speaks to him.He begins preaching to his relatives andneighbors, and soon he has the wholetown in a state of religious fervor. Peoplesay he has a “calling.” His reputation as aprophet and healer spreads, and in timehe is drawing large audiences everywherehe goes. However, when he ventures intoSt. Louis and attempts to hold a prayermeeting, blocking traffic on a main streetat rush hour, he is arrested. He tells thepolicemen about his conversations withGod, and they hurry him off to the nearest mental hospital.—from Understanding Psychology, Richard A.Kasschau, 1995ho is right? The prophet or the police officers? It is often difficult to draw a line between normal and abnormal behavior.Behavior that some people consider normal seems abnormal toothers. Many believe that having visions and hearing voices are importantparts of a religious experience. Other people believe these are symptomsof a psychological disorder. The man in the example above was interviewed by psychiatrists, diagnosed as paranoid schizophrenic, and hospitalized. Had he stayed home, people would have continued to see himas perfectly normal—even popular.WChapter 16 / Psychological Disorders 447
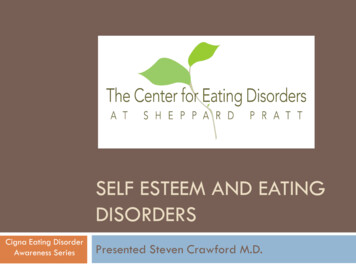
Figure 16.1Defining BehaviorThis person is obviouslysuffering, but is herbehavior abnormal? Theabnormality of her behavior would depend onwhether other elements ofa psychological disorderare present. Why isadjustment an importantway to distinguish normal behavior fromabnormal behavior?DEFINING ANDIDENTIFYINGPSYCHOLOGICALDISORDERSIn our example, the man wasclassified as mentally troubledbecause his behavior was so differentfrom what others felt was normalunder the circumstances. Yet the factthat a person is different does notnecessarily mean that he or she is suffering from a mental illness. Indeed,going along with the crowd mayat times be self-destructive. Mostreaders—and most psychologists—would agree that a teenager who usescocaine because nearly everyone inhis social circle does has problems.How, then, do psychologists distinguish the normal from the abnormal? There are a number of ways to define abnormality, none of which isentirely satisfactory. We will look at the most popular ways of drawingthe line between normal and abnormal in terms of deviance, adjustment,and psychological health. Then we will look at the application of theseprinciples in legal definitions of abnormality. Finally, we will consider thecriticism that in all these models people are arbitrarily labeled mentally ill.Deviation From NormalityDid You Know?Hysteria Sometimes a lack of knowledgeleads to nonsensical explanations for psychological phenomena. For example, theterm hysteria comes from the Greek wordfor “uterus.” The ancient Greeks diagnosedwomen with mental disorders by using atheory that the womb somehow movedaround the body, occupying different positions. This “wandering of the uterus” theoryled to characterizing any highly emotionalbehavior as hysteria. In the Middle Ages,the wandering uterus theory was used toexplain demonic possession and led topersecutions of women for witchcraft.448 Chapter 16 / Psychological DisordersOne approach to defining abnormality is to saythat whatever most people do is normal.Abnormality, then, is any deviation from the averageor from the majority. It is normal to bathe periodically, to express grief at the death of a loved one, andto wear warm clothes when going out in the cold,because most people do so. Because very few peopletake 10 showers a day, laugh when a loved one dies,or wear bathing suits in the snow, those who do somay be considered abnormal.The deviance approach, however, as commonlyused as it is, has serious limitations. If most peoplecheat on their income-tax returns, are honest taxpayers abnormal? If most people are noncreative, wasShakespeare abnormal? Different cultural norms mustalso be taken into consideration (see Figure 16.2).Because the majority is not always right or best, thedeviance approach to defining abnormality is not byitself a useful standard.
AdjustmentAnother way to distinguish normal from abnormal people is to saythat normal people are able to get along in the world—physically, emotionally, and socially. They can feed and clothe themselves, work, findfriends, and live by the rules of society. By this definition, abnormal people are the ones who fail to adjust. They may be so unhappy that theyrefuse to eat or so lethargic that they cannot hold a job. They may experience so much anxiety in relationships with others that they end upavoiding people, living in a lonely world of their own. However, not allpeople with psychological disorders are violent, destructive, or isolated.Sometimes, a person’s behavior may only seem normal. Also, behaviorthat is socially acceptable in one society may not be acceptable inanother. Again, the cultural context of a behavior must also be takeninto consideration.Psychological HealthThe terms mental illness andmental health imply that psychological disturbance or abnormalityis like a physical sickness—suchas the flu or tuberculosis. Although many psychologiststhink that mental illness isdifferent from physical illness,the idea remains that there issome ideal way for people tofunction psychologically, just asthere is an ideal way for peopleto function physically. Somepsychologists believe that thenormal or healthy personwould be one who is functioning ideally or who is at leaststriving toward ideal functioning. Personality theorists suchas Carl Jung and AbrahamMaslow (see Chapter 14) havetried to describe this strivingprocess, which is often referredto as self-actualization. According to this line of thinking, to benormal or healthy involves fullacceptance and expression ofone’s own individuality andhumanness.One problem with thisapproach to defining abnormality is that it is difficult toFigure 16.2Is This Normal?What we consider normal and abnormal behavior depends onthe context of the behavior. Here two men in Michoacán State,Mexico, display cultural dance masks. Why must you considerthe cultural context of a behavior when determiningwhether the behavior is abnormal?Chapter 16 / Psychological Disorders 449
determine whether or not a person is doing a good job of actualizing himself or herself. How can you tell when a person is doing his or her best?What are the signs that he or she is losing the struggle? Answers to suchquestions often are arbitrary.That definitions of abnormality are somewhat arbitrary has led some theorists to conclude that labeling a person as mentally ill simply because his orher behavior is odd is a mistake as well as cruel and irresponsible. The foremost spokesperson of this point of view is American psychiatrist ThomasSzasz (1984).Szasz argued that most of the people whom we call mentally ill arenot ill at all. They simply have “problems in living” that cause seriousconflicts with the world around them. Yet instead of dealing with thepatients’ conflicts as things that deserve attention andrespect, psychiatrists simply label them as sick andshunt them off to hospitals. Society’s norms remainunchallenged, and psychiatrists remain in a comfortable position of authority. The ones who lose arethe patients, who by being labeled abnormal areThe Insanity Defensedeprived both of responsibility for their behavior andof their dignity as human beings. As a result, SzaszWhen John Hinckley was tried forshooting President Ronald Reagan in 1981,claimed, the patients’ problems intensify. Szasz’s posihe was found “not guilty by reason of insantion, however, is a minority stand. Most psychologistsity.” This raised public concerns about theand psychiatrists would agree that a person wholegal definition of sanity.claims to be God or Napoleon is truly abnormal andIn this case, not guilty did not meandisturbed.that Hinckley did not commit the crime; itThe fact that it is difficult to define abnormalitymeant that he could not tell right fromdoesnot mean that such a thing does not exist. Whatwrong or could not control his behavioritdoesmean is that we should be very cautious aboutbecause of a psychological disorder.Therefore, he could not be held criminallyjudging a person to be mentally ill just because he orresponsible for his behavior.she acts in a way that we cannot understand. It shouldThe terms sane and insane are legalalso be kept in mind that mild psychological disordersterms. Psychological research has identifiedare common. It is only when a psychological problemso many disorders of varying degrees thatbecomes severe enough to disrupt everyday life that itinsane is too simplistic a term for a personis thought of as an abnormality or illness.with a psychological disorder. In fact, manypeople with psychological disorders areclassified as sane under current legalstandards.People found not guilty by reason ofinsanity are not simply released; they areconfined for treatment in special hospitals.Studies show that people found not guiltyby reason of insanity are held for at least aslong as people found guilty and sent toprison for similar crimes (AmericanPsychiatric Association, 1993). After theHinckley insanity defense, many states created review boards to oversee the treatmentprovided to those who have been found notguilty by reason of insanity.450 Chapter 16 / Psychological DisordersTHE PROBLEM OF CLASSIFICATIONFor years psychiatrists have been trying to devise alogical and useful method for classifying emotional disorders. This task is difficult, because psychologicalproblems do not lend themselves to the same sort ofcategorizing that physical illnesses do. The causes andsymptoms of psychological disturbances and breakdowns and the cures for those breakdowns are rarelyobvious or clear-cut.All of the major classification schemes haveaccepted the medical model; they assume that abnormal behavior can be described in the same manner as
any physical illness. Thephysician diagnoses a specificdisease when a person hasProfiles In Psychologycertain symptoms.In 1952 the American Psychiatric AssociationAbraham Maslowagreed upon a system for1908–1970classifying abnormal symptoms, which it published in“Human life will neverthe Diagnostic and Statisticalbe understood unless itsManual of Mental Disorders, orhighest aspirations areDSM. This book has beentaken into account.”revised four times as theDSM-II (1968), DSM-III(1980), and DSM-IIIne of the founders of humanistic psychology, AbrahamRevised (1987). The mostMaslow spent his life developing theories that shapedrecent comprehensive recounseling, education, social work, theology, marketing, andvision, the DSM-IV, wasmanagement. Early in his career, Maslow upset behaviorists bypublished in 1994 and acontradicting their theories of motivation and personality. If youminor text revision, DSMrecall, behaviorists propose that individuals learn new behaviors byIV-TR, in 2000.responding to environmental stimuli that reward or punish theirA major change ocbehaviors. Maslow emphasized that each individual has freedom incurred in the shifts fromdirecting his or her own future. Maslow believed that individualsDSM-II to DSM-III-R.could achieve personal growth and self-fulfillment.Before 1980, the two mostMaslow developed a theory of motivation that describes ancommonly used diagnosticindividual’s hierarchy of needs (see Chapter 12). Individualsdistinctions were neurosisprogress from filling basic, biological needs to the highest socialand psychosis. Althoughneeds of what Maslow called self-actualization—the fulfillment ofthese terms have beenone’s greatest human potential. Individuals organize their livesreplaced by more specificaround these needs, trying to fulfill the needs at each level. If needsones, they still are used byare not fulfilled at any level, conflict results. Attention to thesemany psychologists. Howneeds, then, is a method to resolve psychological conflict.ever, the conditions originally identified under neurosisand psychosis have beenexpanded into more detailedcategories, including anxiety disorders,DSM-IV: the fifth version ofsomatoform disorders, dissociative distheAmerican Psychiatricorders, mood disorders, and schizophrenia.OAssociation’s Diagnostic andStatistical Manual of MentalDisordersDSM-IV: New Ways to Categorize Mental IllnessWithin each diagnostic category of the DSM-IV, the followingdescriptions are included:1. essential features—characteristics that define the disorder;2. associated features—additional features that are usually present;3. information on differential diagnosis—that is, how to distinguish thisdisorder from other disorders with which it might be confused; andChapter 16 / Psychological Disorders 451
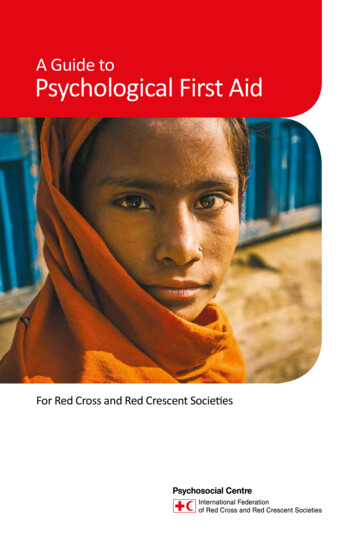
4. diagnostic criteria—a list of symptoms, taken from the lists of essentialand associated features, that must be present for the patient to begiven a particular diagnostic label.These more precise diagnostic criteria reduce the chances that thesame patient will be classified as schizophrenic by one doctor and manicdepressive by another. Because researchers often rely on diagnostic labelsto study underlying factors that may cause disorders, it is especiallyimportant for their work that patients with similar symptoms be classifiedin the same diagnostic category.The DSM-IV also recognizes the complexity of classifying people onthe basis of mental disorders. Often a person may exhibit more than onedisorder or may be experiencing other stresses that complicate the diagnosis. In early classification systems, it was difficult to give a patient morethan one label. The DSM-III-R and now the DSM-IV have overcome thisDSM-IV—Major Psychological Disorders of Axis IFigure 16.3Individual cases of psychological disorders are diagnosed on the fiveaxes of the DSM-IV. Axis I classifies symptoms into categories. Whatare impulse control disorders?Disorders usually first diagnosed ininfancy, childhood, or adolescenceIncludes disorders typically arising before adolescence, includingattention deficit disorders, mental retardation, and stutteringDelirium, dementia, and other cognitive disordersIncludes disorders of perceptual, memory, and thought distortion thatstem from damage to the brain, such as Alzheimer’s diseaseSubstance-related disordersIncludes maladaptive use of alcohol and drugsSchizophrenia and other psychoticdisordersCharacterizes types of schizophrenia and psychotic disorders bysymptomsMood disordersIncludes disorders characterized by emotional disturbance, such asdepression and bipolar disorderAnxiety disordersIncludes disorders characterized by signs of anxiety, such as panicdisorders and phobiasSomatoform disordersIncludes disorders characterized by somatic symptoms that resemblephysical illnesses, such as conversion disorder and hypochondriasisDissociative disordersIncludes disorders that are characterized by sudden and temporarychanges in memory, consciousness, identity, and behavior, such asdissociative identity disorderSexual and gender-identity disordersIncludes preferences for unusual acts to achieve sexual arousal andsexual dysfunctionsEating disordersIncludes disorders such as anorexia nervosa and bulimia nervosaSleep disordersIncludes disorders associated with sleep, such as insomnia andsleepwalkingImpulse control disordersIncludes disorders characterized by a tendency to act on impulsesthat others usually inhibit, such as to gamble excessively or stealSource: DSM-IV, American Psychiatric Association, 1994.452 Chapter 16 / Psychological Disorders
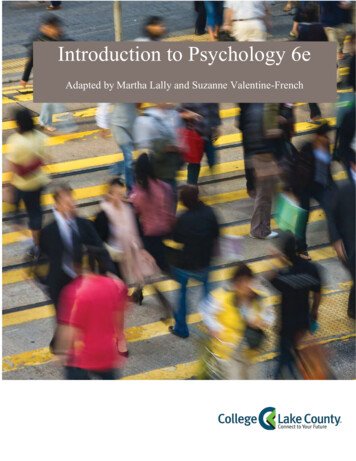
Figure 16.4PET ScansThe biological roots of abnormal behavior include genetic factors andoccurrences that can lead to abnormal brain development. From leftto right, these PET scans show a normal human brain, a brain tumor,and a brain aneurysm. Which axis of the DSM-IV describes themedical conditions of psychological disorders?problem by using five major dimensions, or axes, to describe aperson’s mental functioning. Each axis reflects a different aspect of apatient’s case.Axis I is used to classify current symptoms into explicitly defined categories. These categories range from disorders that are usually first eviReading Checkdent in infancy, childhood, or adolescence (such as conduct disorders) toHow does the DSM-IVsubstance-use disorders (such as alcoholism) to schizophrenia. Figure categorize psychological16.3 shows a listing of major Axis I categories.disorders?Axis II is used to describe developmental disorders and long-standingpersonality disorders or maladaptive traits such as compulsiveness,over-dependency, or aggressiveness. Axis II is also used to describe specific developmental disorders for children, adolescents, and, in somecases, adults. Examples of developmental problems that would be classified under Axis II are language disorders, reading or writing difficulties,mental retardation, autism, and speech problems.It is possible for an individual to have a disorder on both Axis I andAxis II. For example, an adult may have a major depression noted on AxisI and a compulsive personality disorder noted on AxisII. A child may have a conduct disorder noted on AxisI and a developmental language disorder on Axis II. Inother cases, a person may be seeking treatment primarNeurosis In DSM-II, neurosis was usedily for a condition noted on Axis I or Axis II only. Theto describe a variety of anxiety-baseduse of both Axes I and II permits multiple diagnosesdisorders. Today, these disorders areand allows the clinician flexibility in making proviidentified individually in DSM-IV as moodsional diagnoses when there is not enough informationdisorders, anxiety disorders, somatoformavailable to make a firm diagnosis.disorders, and dissociative disorders.Axis III is used to describe physical disorders orAlthough anxiety-based behaviors are stillgeneral medical conditions that are potentially relevantsometimes described as neurotic, the termto understanding or caring for the person. In someneurosis is no longer used to identify anycases, a physical disorder such as brain damage or apsychological disorder.chemical imbalance may be causing the syndromediagnosed on either Axis I or II.Did You Know?Chapter 16 / Psychological Disorders 453
PSYCHOLOGYStudent Web ActivityVisit the UnderstandingPsychology Web site atglencoe.com and clickon Chapter 16—StudentWeb Activities for anactivity on psychologicaldisorders.Axis IV is a measurement of the current stress level at which the person is functioning. The rating of stressors (such as death of a spouse or lossof a job) is based on what the person has experienced within the past year.The prognosis may be better for a disorder that develops following a severestressor than for one that develops after no stressor or a minimal stressor.Axis V is used to describe the highest level of adaptive functioning present within the past year. Adaptive functioning refers to three major areas:social relations, occupational functioning, and the person’s use of leisuretime. Social relations refer to the quality of a person’s relationshipswith family and friends. Occupational functioning involves functioning as aworker, student, or homemaker and the quality of the work accomplished.Use of leisure time includes recreational activities or hobbies and the degreeof involvement and pleasure a person has in them.This five-part diagnosis may be extremely helpful to researchers tryingto discover connections among psychological disorders and otherfactors such as stress and physical illness. Although it is helpful, theDSM-IV labels a person, which may have negative influences on that person in the long run. When the label of a mental disorder is applied, it canreduce that person’s sense of responsibility for his/her own actions. It alsoaffects how others, including mental health professionals, regard that person. Experiments have demonstrated that labels affect how others viewsomeone. In one experiment, grade-school boys behaved in a more criticalmanner toward other boys if they had been led to believe that those otherboys had a psychological disorder, such as attention deficit disorder (Harriset al., 1992). It is important to note that many people develop a disorderlisted in the DSM-IV at some point in their life. Of course, many of these incidences are temporary. In effect, many people who qualify for a disorder asdiagnosed according to the DSM-IV are not very different from anyone else.Assessment1. Review the Vocabulary What is theDSM-IV? How do psychologists use it?2. Visualize the Main Idea Using a diagram similar to the one below, identifyand describe three approaches psychologists use to identify psychologicaldisorders.3. Recall Information What are theadvantages and disadvantages of categorizing people by the DSM-IV?4. Think Critically Many people sufferfrom mild psychological disorders.When do you think it is necessary for aperson to seek help?ApproachesIdentifying aPsychologicalDisorder454 Chapter 16 / Psychological Disorders5. Application ActivityCome up with your owndefinitions of normal and abnormal behavior.Explain how they differ from the descriptions inthis section and why you defined them the wayyou did.
Anxiety DisordersReader’s Guide Main IdeaAnxiety disorders are marked by excessive fear, caution, and attempts to avoidanxiety. Vocabulary anxietyphobiapanic disorderpost-traumatic stress disorder Objectives Identify the behavioral patternsthat psychologists label as anxietydisorders. Explain what causes anxiety disorders.Exploring PsychologyNormal Anxiety or Not?If you are walking down the street anda large dog runs at you barking, it’s perfectly normal to be afraid. However, if youget anxious if a dog appears on the TVyou’re watching, that’s a disorder. If a student gets up to give a speech in class andfinds that his hands are trembling and histhroat is dry, that’s normal anxiety. If astudent runs out of the room crying whencalled on to speak or faints while giving aspeech, that isn’t normal.—from the files of Judith R. Levine, SUNYFarmingdalenxiety is a general state of dread or uneasiness that a person feelsin response to a real or imagined danger. People suffering fromanxiety disorders feel anxiety but not just normal anxiety. Theysuffer from anxiety that is out of proportion to the situation provoking it.This intense anxiety may interfere with normal functioning in everydaylife. Anxiety disorders are the most common type of mental illness in theUnited States, affecting 40 million Americans annually (NIMH, 2006).These disorders share certain characteristics, including feelings of anxietyand personal inadequacy and an avoidance of dealing with problems.People with anxiety disorders often have unrealistic images of themselves.People who are deeply anxious seem unable to free themselves of recurringworries and fears. Their emotional problems may be expressed in constantworrying, sudden mood swings, or a variety of physical symptoms (forexample, headaches, sweating, muscle tightness, weakness, and fatigue).Anxious people often have difficulty forming stable and satisfying relationships. Even though their behavior may be self-defeating and ineffective in solving problems, those driven by anxiety often refuse to give uptheir behaviors in favor of more effective ways of dealing with anxiety. InAChapter 16 / Psychological Disorders 455
the DSM-IV, the anxiety disorders discussed include generalized anxietydisorder, phobic disorder, panic disorder, obsessive-compulsive disorder,and post-traumatic stress disorder.GENERALIZED ANXIETY DISORDEROnce in a while, everyone feels nervous for reasons he or she cannotexplain, but a severely anxious person almost always feels this way.anxiety: a vague, generalizedAnxiety is a generalized apprehension—a vague feeling that one is inapprehension or feeling thatdanger. This anxiety potentially could blossom into full-fledged panicone is in dangerattacks, which may include choking sensations, chest pain, dizziness,trembling, and hot flashes. Unlike fear, which is a reaction to real andidentifiable threats, anxiety is a reaction to vague or imagined dangers.Some people experience a continuous, generalized anxiety. Fearingphobia: an intense and irraunknownand unforeseen circumstances, they are unable to make decisions ortional fear of a particular objector situationenjoy life. They may become so preoccupied with their internal problems thatthey neglect their social relationships. People who experience generalized anxiety often have trouble dealing with their family and friends and fulfilling their responsibilities, and this adds to their anxiety. They areFigure 16.5 Normal Anxietytrapped in a vicious cycle. The more they worry, the more difficultythey have; the more difficulty they have, the more they worry.Many situations may causeOften the experience of generalized anxiety is accompaniedtemporary anxiety or tension.by physical symptoms such as muscular tension, an inability toAnxiety becomes a problem onlyrelax, a furrowed brow, and a strained face. Poor appetite,when it interferes with your abilityindigestion, diarrhea, and frequent urination are also common.to cope with everyday life. WhatBecause anxious people are in a constant state of apprehension,are some characteristics ofthey may have difficulty sleeping or, once asleep, may wake uppeople who suffer from anxietysuddenly in the night. As a result, they may feel tired when theydisorders?wake up in the morning.Why are some people so anxious? Some theorists stress therole of learning in producing anxiety. If a man feels very anxiouson a date, for example, even the thought of another date maymake him nervous, so he learns to avoid having dates and therefore never has a chance to unlearn the anxiety. His anxiety maythen generalize to other situations and become a worse problem.Other research suggests that anxiety disorders may be partlyinherited. Environmental factors, such as unpredictable traumatic experiences in childhood, may also predispose someone todeveloping an anxiety disorder. Such a disorder usually occursfollowing a major life change, such as getting a job or having ababy. The uncertainties of modern life also may help explain thehigh incidence of generalized anxiety.PHOBIC DISORDERWhen severe anxiety is focused on a particular object, animal,activity, or situation that seems out of proportion to the real dangers involved, it is called a phobic disorder, or phobia. Phobias456 Chapter 16 / Psychological Disorders
Figure 16.6PhobiasSome people’s lives are consumed by inappropriate fears. Thesefears interfere with normal, everyday life. These people are sufferingfrom a phobia. What is the fear of flying called?Acarophobia: fear of itching or theinsects that cause itchingAcrophobia: fear of heightsAerophobia: fear of flyingAgoraphobia: fear of open spacesAtelophobia: fear of imperfectionAutophobia: fear of being aloneCatagelophobia: fear of being ridiculedClaustrophobia: fear of closed spacesEntomophobia: fear of insectsFelinophobia: fear of catsHeliophobia: fear of the sunHemophobia: fear of bloodHydrophobia: fear of waterLogizomechanophobia: fear of computersLygophobia: fear of darknessNosocomephobia: fear of hospitalsVerminophobia: fear of germsZoophobia: fear of animalsmay be classified as specific phobias, social phobias, and agoraphobia. Aspecific phobia can focus on almost anything, including high places (acrophobia), enclosed spaces (claustrophobia), and darkness (nyctophobia)(see Figure 16.6). Victims of social phobias fear that they will embarrassthemselves in a public place or a social setting. Perhaps the most commonspecific fear is of speaking in public, but others include eating in public,using public restrooms, meeting strangers, and going on a first date.Phobic individuals develop elaborate plans to avoid the situationsthey fear. For example, people suffering from an extreme fear of being ina public place (agoraphobia) may stop going to movies or shopping inlarge, busy stores. Some reach the point where they will not leave theirhouses at all because that is the only place they feel safe.Phobias range in intensity from mild to extremely severe. Most people deal with phobias by avoiding the thing that frightens them. Thus thephobias are learned and maintained by the reinforcing effects of avoidance, which reduces anxiety but not the phobia. One form of treatment forphobias involves providing the phobic person with opportunities to experience the feared object under conditions in which he or she feels safe.PANIC DISORDERAnother kind of anxiety disorder is panic disorder. (Panic is a feelingof sudden, helpless terror, such as the overwhelming fright one mightexperience when cornered by a predator.) During a panic attack, a victimpanic disorder: an extremeanxiety that manifests itself inthe form of panic attacksChapter 16 / Psychological Disorders 457
What fears are most commonamong teenagers?Although most people do not experiencesevere phobias, many do experience mildfears. Find out what fears your classmatesexperience or have experienced.Procedure1. Prepare a list identifying some objects, animals, activities, or situations that are feared.2. Distribute the list among your friends, classmates, and the adults you know.3. Direct them to check the items on the listthat ide
—from Understanding Psychology,Richard A. Kasschau, 1995 Chapter 16 / Psychological Disorders447 W ho is right? The prophet or the police officers? It is often dif-ficult to draw a line between normal and abnormal behavior. Behavior that some people consider normal seems abnormal to others