Transcription
VESTIBULARTHERAPY ANDASSESSMENTJuly 29, 2016Marc Hinze, PT, MPT, CIMTBronson Rehabilitation Services
Objectives Vestibular Assessment Vestibular Rehabilitation Progression of Vestibular Exercise
Vestibular System Vestibulo-spinalReflex (VSR) Vestibulo-ocularReflex (VOR) Functions– Postural Stability– Gaze Stability– Sensory Integration Impairments– Dizziness– Unsteadiness/sense of motion– Blurred Vision– Headache– Nausea
Prevalence of Vestibular Symptomswith Concussion 90% of children with concussion had 1 ormore abnormal balance and vestibularfindings (Zhou et al) 69% of adolescents with concussion alsohad a visual diagnosis(Master et al)– Accommadative Disorder (Focusing)– Convergence Dysfunction (Viewing near targetwithout double vision)– Saccadic Dysfunction (eye motion)
Vestibular Screening Dizziness– Motion Provoked: Head movement, Bending,changing direction– Visually provoked: Busy patterns, watching motion,busy environments– Positional Sensitivity: supine sit, sit stand– Eye Motion: Visual tracking Imbalance Difficulty Reading– Blurred vision– Eye strain– Headache and fatigue Neck Pain: Cervicogenic Dizziness
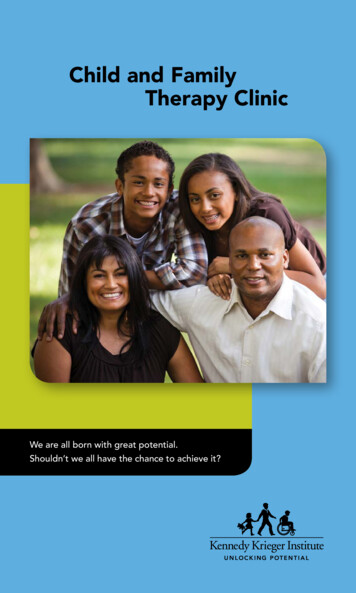
Vestibular Ocular Motor ScreenVOMS TestNot 0-10CommentsBaseline SymptomsSmooth Pursuits (eyes move, head still) stand 3 ftaway, follow PT fingertip in H pattern, 2 reps, 2seconds/rep-eyes onlySaccades - Horizontal (eyes move, head still) stand3 ft away, PT 2 fingtips 3ft apart 10 reps as quicklyas possible-eyes only L/RSaccades - Vertical (eyes move, head still) stand 3ft away, PT 2 fingtips 3ft apart 10 reps as quickly aspossible-eyes only up/downConvergence (Near Point) PT/pt holds 14 point font"x" on tongue depressor move slowly until seesdouble or eyes turn out measure 3x in cm from endof noseVOR-Horizontal (eyes on target, head moves) ptholds 14 point font "x" on tongue depressor 10 reps,rotates head 20 deg R/L @ 180 bpmVOR-Vertical (eyes on target, head moves) pt holds14 point font "x" on tongue depressor 10 reps,rotates head 20 deg up/down @ 180 bpmVisual Motion Sensitivity (VMS) 5 reps, rotatethumb/eyes/head/trunk together 80 deg @ 50 bpm 5 cm normal
Smooth Pursuits Ability of the eyes to smoothly follow aslow moving target with the headstationary Normal eye pursuit is smooth Abnormal pursuit is choppy and canincrease symptoms
Saccades Ability of the eyes to move quickly andaccurately between targets with the headstationary Normal – good ability to track withoutsymptoms Abnormal – poor symmetry, nystagmus,increase in symptoms
Convergence Ability to view a near target withoutdouble vision 14 point font target on a tongue depressor Abnormal is when one eye turns outwardor the patient reports double vision 5cm from the end of nose
Vestibulo-ocular Reflex The ability to stabilize vision as the head moves Screen– Head turns 20 deg R/L at 180 beats/min whilemaintaining focus on target Test is abnormal if eyes slip off target or reports blurredvision and target motion Repeat in vertical direction– Dynamic Visual Acuity Test (DVAT) Using Snellen eye chart the patient reads the lowest linewithin their comfort 20 deg of head turns R/L are performed at 120 bpm A 3 three line or greater move on the Snellen chart isconsidered abnormal
Visual Motion Sensitivity Test visual motion sensitivity Head, eyes and trunk all move togetherwhile following a visual target The patient stands with feet shoulderwidth apart
Vestibulo-spinal Assessment Tools SOPFunctional Gait AssessmentDGIBESSPositional Sensitivity Assessment
Gans Sensory OrganizationalPerformance Test Feet together EO, ECTandem EO, ECFoam EO, ECFUKUDA – 20 to 50 marches. Abnormal spin or drift
Vestibular-ocular Assessment VOMS DVAT
Goals of Vestibular Therapy Decrease Dizziness and Visual SymptomsImprove BalanceIncrease Activity LevelReturn to Work, Academics, ReadingReturn to Sport
Principles of Vestibular Therapy Individualized Program Transient increase in symptoms areexpected Modify exercise intensity as needed Sports specific/work specific
Cervico-vestibular Rehab Non-provocative ROM Postural education Strengthening and stretching for muscularimbalance Upper cervical manipulation? Upper cervical joint mobilization
General Guidelines for VestibularExercise Perform 2-3 times per day Exercise should not increase headache a½ level on the pain scale Exercise may provoke dizziness. If dizziness reaches a level of 5-7/10make modifications to reduce intensity ofexercise– Decrease reps– Decrease speed– Perform sitting vs standing
VOR Progression Sitting Standing Decrease base of support (stand shoulderwidth to feet together, modified tandem totrue tandem etc.) Altered surface
Balance Progression Level surfaceBase of supportAltered surfaceSingle leg stanceStatic to dynamic
Clinician-DirectedProgram Adaptation
Clinician-DirectedProgram Adaptation and Substitution
Clinician-DirectedProgram Substitution
References Carender W, Alsalaheen BA, Vestibular Physical Therapy Post-Concussion:Indications, Assessment and Treatment, Return on Investment: A Sports MedicineApproach, U of M Health System. May 20-21, 2016Alsalaheen BA, Whitney SL, Mucha A, Morris LO, Furman JM, Sparto PJ. Exerciseprescription patterns treatedwith vestibular rehabilitation after concussion.Physiother. Res. Int 2012Alsalaheen BA, Whitney SL, Mucha A, Morris LO, et al. Rehabilitation for dizziness andbalance disorders after concussion. JNPT 2010; 34:87-93.Barnett BP, Singman EL. Vision concerns after mild traumatic brain injury. Curr TreatOptions Neuol 2015;17:5.Broglio SP, Tomporowski PD, Ferrara MS. Balance performance with a cognitive task:A dual-task testing paradigm. Medicine & Science in Sports & Exercise. 2005; 689695.Collins MW, Kontos AP, Reynolds E. A comprehensive, targeted approach to theclinical care of athletes following sport-related concussion. Knee Surg SportsTraumatol Arthroscm 2013.Ellis MJ, Leddy JJ, Willer B. Physiological, vestibulo-ocular and cervicogenic postconcussion disorders: an evidence-based classification sysyem with directions fortreatment. Brain Injury. 2015;29(2):238-48.Kontos AP, Elbin RJ. Schatz P, et al. A revised factior structure for the PostConcussion Symptom Scale: baseline and post-concussion factors. Am J Sports Med.2012; 40(10):2375-2384.Kontos AP, Elbin RJ, Lau B et al. Posttraumatic migraine as a predictor of recoveryand cognitive impairment after sport-related concussion. Am J Sports Med. July2013;41(7):1497-1504.
References Lau BC, Kontos AP, Collins MW, Mucha A, Lovell MR. Which on –field signs/symptomspredict protracted recovery from sport-related concussion among high school footballplayers? Am J Sports Med. 2011;39(11):2311-2318.Lee H, Sullivan SJ, Schneiders AG. The use of dual-task paradigm in detecting gaitperformance deficits following a sports-related concussion: A systematic review andmeta-analysis. Journal of Science and Medicine in Sports. 2012; 705:2-6.Master CL, Scheiman M, Gallaway M et al. Vision diagnoses are common afterconcussion in adolescents. Clinical Pediatrics 2016;55(3):260-267.Mucha A, Collins MW, Elbin RJ, Furman JM, Troutman-Enseki C, DeWolf RM,Marachetti G, Kontos AP. A brief vestibular/ocular motor screening (VOMS)assessment to evaluate concussions. Am J Sports Med. October 2014;42(10):24792486.Schneider et al Cervicovestibular rehabilitation in sport-related concussion: arandomized controlled trial. Br J Sports. 2014.Zhou G, Brodsky JR. Objective vestibular testing of children with dizziness andbalance complaints following sports-related concussion. Otolaryngology-Head andNeck Surgery 2015;152(6):1133-1139.Gans R, Vestibular Rehabilitation Seminar, The American Institute of Balance. 2005
Adding a New Slide To add a new slide, click ‘New Slide ‘above and choose the slide you would liketo add. Scroll down the list to seetransition and fact slides. Delete this slide.
Thank you!bronsonhealth.com
–Postural Stability –Gaze Stability –Sensory Integration Vestibular System Impairments . Using Snellen eye chart the patient reads the lowest line . Assessment and Treatment, Return on Investment: A Sports Med