Transcription
EVERYTHING YOU ALWAYSWANTED TO KNOW ABOUT VOICEAND RESONANCE DISORDERS BUTWERE AFRAID TO ASK (I.E. THEMARY AND MARC VELUM AND LARYNXSHOW)Marc Haxer M.A.CCCandMary K Berger M.S.CCCUniversity of Michigan Health SystemsAnn Arbor, MI
So where do we start?
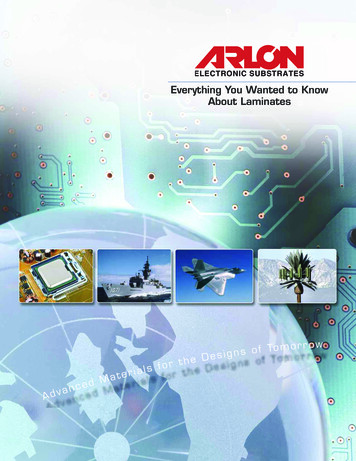
Anatomy Structures Hard palatePalatine raphe/posteriornasal spineSoft palate/velumUvula/musculus uvulaeAnterior faucial arches(palatoglossus)Posterior faucial arches(palatopharyngeus)Palatine tonsils
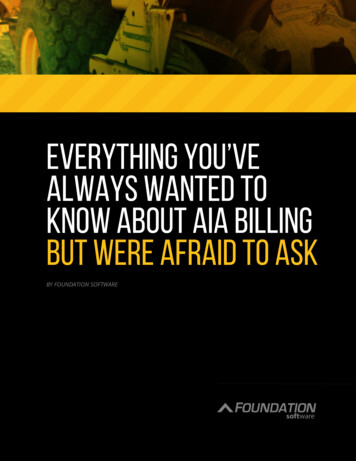
TYPES OF CLEFTING
Anatomy
Anatomy/physiology Muscles Palatine aponeurosisTensor veli palatiniLevator veli palatinimuscle repaired at thetime of eus)Musculus uvulaeSuperior constrictorlateral wall movement
Perceptual exam Performed by a Speech PathologistThe Gold Standard for the diagnosis ofvelopharyngeal dysfunctionNeed imaging to determine intervention.
Oral motor exam Head/neck: ears, torticollis, cranial vaultFace: structures, symmetry, sensationMandible: structure, ROM, strength testingDentition: occlusion, missing teeth, denturesTongue: structure, strength, ROM, RAMPalate: uvula, fistula, length, distance to posteriorpharyngeal wall, Passavant’s ridge, mesialmovement of lateral pharyngeal walls, gagresponse.
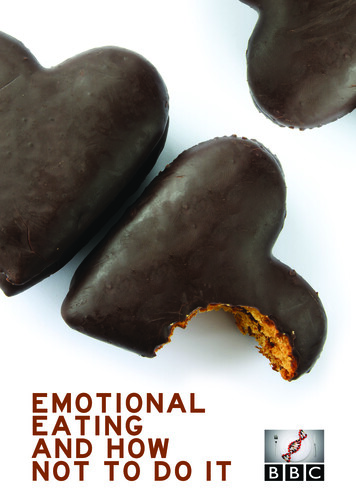
Left unilateral cleft lip and palate
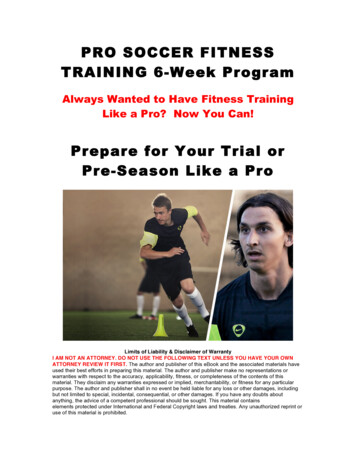
Bilateral cleft lip and palate
Cleft palate only
Oronasal fistulaCommunication betweenthe oral and nasalcavities Cancomplain of nasalregurgitation May be difficult to seeor tell if trulycommunicates Often no effect onspeech resonance Gum test
Submucous cleft palatebifid uvula zona pellucida (thin, bluetinged mucosa) posterior nasal spinenotching lateral levator musclebulges /- hypernasality nasal regurgitation withliquids Occult cleft-absentmusculus uvulae
Velopharyngeal valveSoft palate (velum) contacts posteriorpharyngeal wall to transmit air pressureand sound energy into the oral cavity fororal consonant and vowel productions.Normal valving allows adequate intraoral air pressure, normal oral resonanceand sufficient breath support for normallength of utterance. Structural defect MAYinterfere with closure.
Speech perceptual exam Articulation-place and manner, ation-quality, consistencyProsody-inflection, timing, rateSpeech intelligibility rating (4 point scale)Speech acceptability rating (4 point scale)
Velopharyngeal dysfunction- VPDVelopharyngeal dysfunction (VPD) orVelopharyngeal Inadequacy (VPI)- absence ofclosure of velopharyngeal port withhypernasality, nasal air emission. Variety ofcauses. Average 5%-25% of cleft childrenhave resonance disorder. Needs furtherworkup.
Hypernasality If normal resonance, all consonants and vowelsproduced orally except m and n. Velopharynx closedwith no air into nasal cavity. All breath support forspeech directed orally.If air leak into nose results in hypernasality, nasalemission, nasal turbulence and/or nasal grimace.Impaired velopharyngeal closure most commonetiology for hypernasality; oronasal fistula MAY causehypernasality/nasal air emission.
Velopharyngeal dysfunctionVelopharyngeal dysfunction (VPD) orvelopharyngeal inadequacy (VPI) withoutpresence of a cleft: R/o submucous or occult cleft Articulation disorder S/p adenoidectomy Velocardiofacial syndrome (DiGeorgesyndrome, 22q11 deletion) “the black hole”
Velopharyngeal insufficiency Palatetoo short Structural problem Not enough tissue attime of initial cleftrepair Submucous cleft (SMC) Deep pharynx due tocranial base anomalies FollowingadenoidectomyNeeds surgery to correct.
Velopharyngeal closure using adenoid
Velopharyngeal incompetence Reducedmovement ofsoft palate Physiological cause Poor muscle function Pharyngeal hypotonia Velar paralysis orparesis Dysarthria Apraxia
Manifestations of VPDPrimary Manifestations Nasal regurgitationInappropriate air flowNasal rustles/ turbulenceHypernasal resonanceCompensatorymisarticulationsPoor speech intelligibilitySecondary Manifestations Nasal grimaceHoarsenessVocal cord nodulesShort utterance lengthSoft voice syndrome
Resonance disorders Resonance descriptors (don’t say “nasally speech”) Hypernasality-especially on vowels and voiced oralconsonants Hyponasality/denasality-too nasal resonance /m, n,ng/ Cul de sac resonance (hypertrophiedtonsils/adenoids) Mixed resonance-hyper- and hyponasality(congestions, deviated/deflected septum) Audible nasal turbulence; nasal rustle -Phoneme specific VPD
Hypernasality If normal resonance, all consonants and vowelsproduced orally except m and n. Velopharynx closedwith no air into nasal cavity. All breath support forspeech directed orally.If air leak into nose results in hypernasality, nasalemission, nasal turbulence and/or nasal grimace.Impaired velopharyngeal closure most commonetiology for hypernasality; oronasal fistula MAY causehypernasality/nasal air emission.
Oral consonants High pressure consonants:p,b,t,d,k,g,s,z,sh,ch,jLow pressure consonants:r,l,w,h,y and vowelsHigh pressure consonants may be weakened ornasalized with VPD.
HyponasalityNasal consonants /m/ /n/ /ng/ Velopharynxopen allowing consonant to resonantthrough nose Sensitive to nasal obstruction Only nasal consonants effected by hyponasality Causes /m/ to sound like /b/, /n/ to sound like /d/and /ng/ to sound like /g/. Reduced nasal emission with mirror on nasal productions
Mixed resonanceEvidence for both hypernasality due tovelopharyngeal dysfunction and hyponasalitydue to often nasal obstruction Often reduced nasal air emission from onenaris on mirror exam
Phoneme specific nasal emission (PSNAE)Hypernasality or nasal airemission due toarticulation error pattern Not physical etiology;otherwise normalresonance; competent VPmechanism Causes phoneme-specificnasal emission (usuallysibilant sounds).Never surgery-alwaysspeech tx
Assessing resonance withoral consonants Cul de sac testing (Bzoch,1979) produce the oralwords/sentences with thenose open then with the noseclosed. If normal resonance,will be identical productions.Nasal mirror testing undernares for nasal emission(speech and non speechtasks).
Assessing resonanceModified tongue anchor technique: puff cheeks aroundprotruded tongue (Dalston, 1990). See-scape Nasal tubing/stethoscope Assess for presence of compensatory misarticulations **Repeat standardized words, sentences, serial countingand spontaneous speech sampling .**See word/sentences lists at end of presentation
Articulation issues and clefting Cleft lip/ alveolus only-normal incidence of articulationerrors unless untreated hearing deficitsHearing impairmentIncidence of developmental articulation errors similarCompensatory misarticulation errors (generally backing ofplace of articulation in vocal tract with nasal air flow for oralproductions)Abnormal dentition/occlusionDue to inability to achieve velopharyngeal closureMislearning errors (structural or unrelated to cleft)Substitutions and omissions more common than distortions
Compensatory misarticulationsMaladaptive articulation pattern that occurs in individuals who havevelopharyngeal dysfunction. Articulation valving occurs moreposterior in the vocal tract to compensate for reduced intraoral airpressure. Glottal stopPharyngeal stopPharyngeal fricativeLaryngeal fricativeVelar fricativeMid-dorsum palatal stopPosterior nasal fricative/nasal turbulenceOften accompanied by a nasal grimace.
Compensatory misarticulations
Active vs. passive errors Obligatory vs. compensatoryBoth have structural origins (esp. VPD)Passive/obligatory errors: hypernasality, nasalized oralconsonants, weak pressure consonants. Disappear whenstructure corrected.Active/compensatory errors: e.g. glottal stops. Active attemptto compensate for structural deficit. Persist when structurecorrected.Harding and Grunwell, 1998; Hutters and Bonsted, 1987.
Phonation and VPD Hoarseness associated with hyperfunction of thelarynx vocal abuse, check for nodulesHypophonia- due to nasal emission have reducedloudness or may be masking audible nasalturbulence/emissionPeriods of aphonia
Decision time Speech PerceptualExamSound-specific VPISpeechTherapyVP InsufficiencySurgeryVP incompetenceAlmost but notquite closed/InconsistentlyclosedSpeech TherapyModerate to largegap/never closesPalatal Lift or surgery
Medical interventions forresonance disorders Surgical Management is indicated when: hypernasality is caused by structural orphysiological abnormalitymoderate to large velopharyngeal gapvelopharyngeal insufficiencyhyponasality.
Velopharyngeal Insufficiency:needs surgery
Velopharyngeal Insufficiency:needs surgery
VPD: Needs resonance therapy(pre- and post-tx example)
Speech language pathology management hypernasal resonance is associated with oral-motordysfunction/dysarthriahypernasality occurs primarily when the child is tiredthe child is status-post secondary palatal surgery andneeds therapy to increase lateral wall motion, closureof DSP port or increase elevation of the palateduring speechcooperative with adequate cognitive skills
Resonance therapy techniques Don’t blow it! Blowing and sucking exerciseshelp blowing and suckingBlowing exercises do not improvevelopharyngeal strengtheningBlowing can be used to assist withthe idea of oral air stream thatcan then be valved witharticulatorsBlowing bubbles to stimulate forbilabials and oral air flow
Resonance therapy techniques Auditory discrimination hypernasality audible nasal turbulence nasal snort hyponasality
Resonance therapy techniques Exaggerated articulation increasing ROM of the articulators mayassist with increasing palatal closure withincreased muscle recruitmentgenerally slow down rate of speech toimprove velopharyngeal closure andcoordination
Resonance therapy techniques Visual feedback See-Scape (AliMed, SuperDuper, ProEd) or nasal mirror for monitoring nasalair emissiontissue, tissue paper or paper paddle fororal air flow with plosivesfeather for oral air flow with fricativesNasometer (acoustic measurement withvisual feedback-Kay Pentax)biofeedback nasoendoscopy (directvisual feedback of velopharyngealclosure).
Resonance therapy techniques Auditory training: listening tube (fish tank tubing or flexible straw)microphone VU meter or feedback via the speakers(microphone by the mouth or the nose)audible nasal turbulencenegative practice (purposeful hypernasal speechthen purposeful oral production)cul-de-sac training- match oral productions withand without the nares pinched off
Resonance therapy techniques Tactile training: feel airflow on hands feel nasal air flow from nares feel vibration on side of nose with audible nasalturbulence only with voiced consonants yawning followed by vowel-target consonant(flattens base of tongue and elevations soft palate)
Resonance therapy techniques Awareness training:Teach concepts that child can understand to describeoral/nasal airflow for example:-Mr. Mouth/Mr. Nose-mouth and nose sound-”make the wind come out of your mouth”-throat sound or voice box sound
Resonance therapy Therapy note: If persisting hypernasality ornasal emission after a few months of tx, childshould be referred to a specialist for furtherassessment and consideration of physicalmanagement. Don’t keep in tx and continuallyasked to perform a speech task that isimpossible to do.
Compensatory misarticulation therapy Articulation therapy note: Articulation therapycan be effective for place of articulation evenif a surgery is still needed to reducevelopharyngeal dysfunction or a oronasalfistula.
Compensatory misarticulation therapy Accuracy training: Reinforcing place of articulation withexaggerated articulation, may recruit palatalmusculature to increase ROM. Has potentialto achieve velopharyngeal closure ONLY ifcompetent.
Compensatory misarticulation therapy Phoneme hierarchy in therapy: Train front sounds prior to back sounds Voiceless before voiced phonemes Basic articulation therapy rules apply too (introducesounds in developmental hierarchy, begin withsounds in isolation then C-V, V-C and C-V-Ccontexts, etc)Note: work with sounds the child can produce toidentify target sound selection
Compensatory misarticulation therapy Techniques: Whispering (eliminates glottal stops) Forward tongue placement (eliminatepharyngeal fricatives) Pair /h/ with target phonemes Introduce new sound that changes one featureof sound child can produce (t d, m b) OK to use nonsense words briefly for earlypractice
Compensatory misarticulation therapy Techniques-continued Build list of short words with correctlyproduced sounds to practice as warmup and to “remind” child of correctproductions Target at least 50 correct productionsin a 30 minute session with toddlers;100 correct productions with schoolaged children
Compensatory misarticulation therapy Glottal stops Whisper with over aspiration Emphasize fronted productions Voicing at the end of syllable with gradualVOT /h/ plus target labial or lingual oralplacement Produce nasal counterpart then plug nose(m b, n d, ng g); then use partial naresocclusion Use awareness training and be specific whereto place tongue/lips and how to direct airstream
Home programParent(s) need training to hear correctproductions for reinforcing Daily practice Short practice sessions (30-60 seconds) severaltimes per day Reinforcing for self-monitoring/corrections
Craniofacial Team Plastic SurgeryMaxillofacial SurgeryOrthodonticsPediatric DentistryProsthodonticsSpeech PathologyAudiologySocial Work aryngologyCoordinatorCommunityProfessionals
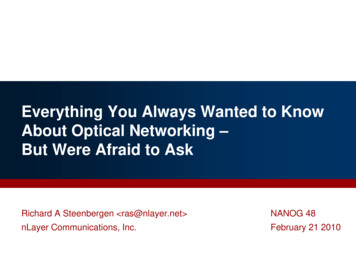
Larynx Cartilaginous tube Connects inferiorly to respiratory system Connects superiorly to vocal tract Trachea, lungsPharynx, oropharynx, nasopharynxAnatomic orientation important Highlights interactive relationship between vocal subsystems Pulmonary mechanismLaryngeal valveSupraglottic vocal tract resonator
Larynx Communicative function of larynx relies heavily onintegration of these vocal subsystems Lungs Vocal folds Provides aerodynamic tracheal pressure that blows vocal folds apartand sets them into vibrationProvide sound source for phonation as vocal folds repeatedlyoscillate during vibrationVocal tract Shapes and filters acoustic energy to produce sound recognized ashuman voice
Larynx Differential dx of voice disorders requires assessmentof these parametersLaryngeal health/function will influence quality of voiceproduction Compromised respiratory support will decrease potential foradequate VF vibration Alteration in shape/size of vocal tract will affect resonance Compromise in any area will adversely affect optimalproduction of voice and increase risk for developmentof voice problem
Schema of Vocal Subsystems
Larynx Complex arrangement of cartilages,muscles, mucous membranes, and connectivetissues Allowsfor wide degrees of variation in position,movement, and tension to support three basicfunctions Airway Airwaypreservation for ventilationprotection to block/repel environmentalinfiltrates Phonation for communication or singing Cartilagehousing serves as columnar protectiveshield for laryngeal valve
Larynx Laryngeal valveachieves thesefunctions throughthree levels of“folds” Aryepiglottic Falsevocal folds True vocal folds
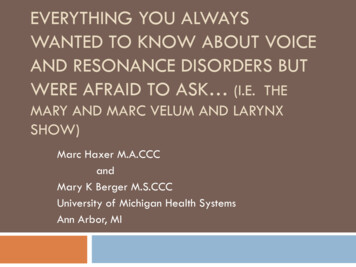
Neurologic Supply Cranial nerve X innervates larynx peripherally Vagus “wanderer”Innervates sites from skull to abdomenInnervates larynx through two important branches Superior laryngeal nerve (SLN) Branches off vagus near nodose ganglia in neckCourses alongside carotid arteriesForms internal/external branches Internal branch provides all sensory information to larynxExternal branch is motor nerve to cricothyroid (CT) muscleRecurrent laryngeal nerve (RLN) Extends to thoraxForms long loop under heart before coursing superiorly under thyroid gland and into larynxDifferent on right/left sides of bodyNerves (especially left) susceptible to injurySupplies all sensory information to area below VFs and all motor innervation to PCA, TA,LCA, and IA muscles
Schema of Laryngeal Innervation
Respiration for Phonation VF vibration is sound source for phonationPhonation dependent on respiratory power provided by lungsand abdominal/thoracic musculature Inferior border of lungs attached to diaphragm by double-walledpleural liningDuring inhalation, diaphragm contracts thus compressing viscera andpulling lungs inferiorly allowing for expanded lung volumeAs lung volume expands, air passively drawn into lungsDuring exhalation, passive elastic recoil/other musculature forces air outof lungsAir moved superiorly through VFs/vocal tractDuring exhalation for voice/speech, VFs adduct to midline thusconstricting outgoing airflowResulting aerodynamic energy sets VFs into oscillation creating vibratorysound that comprises phonation
Vocal Tract Resonance Sound waves from larynx pass through supraglotticair passage into pharynx, oropharynx, andnasopharynxAlso move articulators including velum, hard palate,tongue, and teethExcitation of air molecules within these spacescreates phenomenon called resonance
Etiologies of Voice Disorders Etiology: the science that deals with the causes ororigin of diseases or conditions e.g.,"the etiology is unknown" translates into we don’tknow the cause Medicine.net.Accessed 2/8/10
Etiologies of Voice Disorders West, Kennedy, and Carr (1937) There is always a reason for a voice disorder SLP’s job is to find cause(s) Sometimes easy Sometimes hard VF nodules in a screamerDifferential Dx of ADSD vs. Functional dysphonia vs. subtle VF motiondisorderSuccessful outcome dependent on clinician’s ability todetermine cause(s) based on number of reference points
Major Categories of Etiologic Correlates Voice misuse Phonotrauma Inappropriate vocal componentsMedically related disorders Directsurgery Indirect surgery Chronic illnesses and disorders Primary disorder etiologiesPersonality-related disorders
Medically related disorders Directsurgery Laryngectomy Total, hemi-, supraglottic, supracricoid Glossectomy Hemi-, anterior, posterior, total Mandibulectomy Total, partial Maxillectomy Total, partial Other head and neck surgeries Composite resection, Radical neck dissection
Medically related disorders Indirect surgery Thyroidectomy Partial versus totalHysterectomy May result in temporary/permanent lowering of pitchsecondary to hormonal changes General anesthesia/endotracheal tube Can result in mechanical trauma to VFs/trauma to posteriorlarynx Cardiac Surgery Emergent versus planned Cervical spine surgery Carotid endarterectomy Skull base surgery
Chronic illnesses and disorders Sinusitis/URIs Asthma,COPD, lung CA Allergies Laryngopharyngeal reflux disease Emotional Disorders Endocrine Dysfunction Smoking, alcohol, and drug abuse
Personality-related Disorders Environmental stress Dysphonia secondary to occurrences that cause emotional/physical stresses Loss of employment Death of spouse/significant other Family conflictConversion behaviors Dysphonia as psychological reaction to stressful situation Avoidance behavior(s) developed to counteract stressful situation(s) Whispering, muteness, unusual dysphoniasIdentity conflict Dysphonia secondary to difficulty in establishing individual’s personality High-pitched falsetto in post-pubescent adolescent Weak, juvenile, thin-sounding voice of adult female Increase in fundamental frequency in male-to-female transsexual patient
Pathologies of the LaryngealMechanism Voice disorder present when perceptual attributes ofindividual’s voice differ from those of similar age,geographical location, and cultural backgroundRange of etiologies of voice disorders large;differences may arise from variety of factors Structural, medical, or neurological changes inrespiratory, laryngeal, and vocal tract mechanisms Maladaptive or inappropriate voice use Psychogenic factors
Pathologies of the LaryngealMechanism Complimentary relationship among various physical,voice use, and psychogenic influences ensures that . . Mostvoice disorders/laryngeal pathologies will havecontributions from more than one etiologic factor There is considerable overlap among these threegroupings
Pathologies of the LaryngealMechanism Inappropriatevocal behaviors/excessive vocaldemands may generate organic pathology Psychological trauma/excessive emotional stressmay accompany onset of laryngeal dystonia(ADSD/ABSD) Voice/laryngeal disorders emerging after URI maypersist long after same has resolved
Pathologies of the LaryngealMechanism Previous examples highlight overlap of originaletiologic factor with secondary behaviors thatmaintain voice problemBecause of the above, intervention strategies are alsoeclectic and can include: Medical/surgical management Voice rehabilitation Psychological intervention Combination of the above
Pathology Classifications Structural changes in the vocal foldNeurogenic voice disordersSystemic disease contributors to laryngealpathologiesDisorders of voice useIdiopathic voice disorders
Structural Changes in the Vocal Folds Pathologies of the VFs include any that cause alteration inhistological structure of VFsChanges in mucosal layers or vocal fold muscle body willaffect: Mass, size, stiffness, flexibility, and tension of vibratingmechanism Glottic closure pattern during vibrationAny one of these vocal fold changes has potential to alter: Vocal quality Pitch Intensity
Structural changes of the vocal folds **NodulesPolypsVocal fold hemorrhage/varix**Reinke’s edema/polypoid degenerationLaryngitis: acute/chronicGranuloma/contact ulcerCongenital/acquired cystsPapillomaCongenital/acquired webs**Sulcus vocalis**PresbylaryngeusLeukoplakia and hyperkeratosisVF carcinoma** Voice therapy primary intervention
Vocal Fold Nodules
Vocal Fold Polyps
Vocal Fold Varix/Hemorrhage
Reinke’s Edema
Laryngitis
Contact Granuloma/Ulcers
Congenital/Acquired Cysts
Laryngeal Papilloma
Congenital/Acquired Webs
Sulcus Vocalis
Presbylaryngeus/Vocal Fold Bowing
Leukoplakia/Hyperkeratosis
Laryngeal Carcinoma
Pathology Classifications Neurogenic voice disorders **Unilateral vocal foldparalysisBilateral vocal fold paralysisAdductor spasmodicdysphoniaAbductor spasmodicdysphonia**Essential vocal tremor**Myasthenia gravisMultiple sclerosisHuntington’s chorea**Parkinson’s diseaseAmyotrophic lateral sclerosis** Voice therapy primaryintervention
Pathology Classifications Systemic diseaseinfluences on the larynxand voice Pharmaceutical effectsGrowth hormone influencesThyroid function influencesSex hormonal imbalancesRheumatoid arthritisAllergiesCandidaRespiratory diseasesReflux disease
Pathology Classifications Disorders of voice use Muscletension dysphonia Vocal Fatigue Vocal abuse/misuse Ventricular phonation Puberphonia/mutational falsetto Transgender voice Conversion aphonia
Pathology Classifications Idiopathic voice disorders Paradoxicalvocal fold motion Chronic cough Aboveare components of Irritable Larynx Syndrome alongwith Muscle Tension Dysphonia and Globus sensation Subglotticstenosis Laryngomalacia
The Voice Evaluation Primary objectives: Discoveretiologic factors associated w/development ofvoice problem Describe deviant vocal symptoms
The Voice Evaluation Components of the diagnostic voice evaluation Medicalexamination Patient interview Perceptual evaluation of voice Instrumental analysis Acoustic/aerodynamic Functionalanalysesevaluation of vocal fold movement
The Voice Evaluation Team members Otolaryngologist Voicepathologist Singing voice specialist Neurologist Allergist Endocrinologist Pulmonologist
The Voice Evaluation Otolaryngologist Voice pathologist Examines larynx for pathologyProvide Dx for voice problemDetermines mode of treatmentIdentifies cause(s) of voice disorderEvaluates vocal symptomsEstablishes improved voice through use of various therapeutic techniquesSinging voice specialist Evaluates efficiency/correctness of performance techniqueSuggests modifications as needed
The Voice Evaluation NeurologistEndocrinologistAllergistPulmonologist Abovemedical professionals consulted as needed to aidin diagnosis/management of vocal issues
Medical Examination Detailed history of problemHead and neck examination Otoscopic evaluationExamination of oral/nasal cavitiesPalpation of salivary/thyroid glands and lymph nodesVisual examination of larynx Indirect laryngoscopyFiberoptic laryngoscopyDirect laryngoscopyPertinent medical historyOther tests as indicated Radiographs, CT, MRI of head/neckBlood analysesSwallowing studies
Voice Pathology Evaluation Patient interviewQuestionnaire/QOL SurveyHistory of problemMedical historySocial historyOral mechanism examinationEvaluation of voice components Respiration, phonation, resonance, pitch, intensity, rateInstrumental analysis Functional evaluation of vocal fold movement Acoustic/aerodynamic analysesFlexible mendations
History History of Problem Place all of the information obtained during your patient interview into chronologicalorderMedical History Patient interview Medical chart review Information from physician consult Review of outside recordsSocial History Obtain information from social/work spheres that may have adverse impact onvocal/laryngeal function Change in family dynamics Change in employment status Death in family Levels of stress secondary to above?
Evaluation of Vocal Components Respiration Phonation Too high/too lowLimited in range?Can patient vary the same?Does the voice change with changes in pitch?Intensity Hypo/hypernasal, cul-de-sac, etc.Pitch Qualitative disturbancesAbility to maintain steady pitchConsistent versus inconsistentResonance Diaphragmatic versus clavicular/thoracic focusDegree of upper chest/shoulder/neck tensionToo loud/too softPatient’s ability to vary intensityAny associated vocal changes with variation?Rate Too fast/too slow, changes prior to evaluation, coordination w/respiration
Case Study 64-year-old maleMedical dx of acute necrotic pancreatitis Subsequently underwent elective cholycystectomy 2-month hospitalizationMultiple complicationsExtended second hospitalizationMultiple intubations/extubationsDecline in voice subsequent to hospital dischargeSeen by Otolaryngology/Head and Neck Surgery Dx of right vocal fold granulomaTx’d with anti-reflux measuresReferral to Speech Pathology for videostroboscopy
Videostroboscopy Vocal fold mobility within functional limits bilaterallyRight vocal fold markedly erythematousIrregular configuration to body of right vocal foldEdge of right vocal fold irregularGlottic closure incomplete given edge irregularityof right vocal foldAmplitudes of vibration/mucosal waves absent onright vocal foldVocal fold vibration asymmetric
Marc’s Fab Video Clip
Recommendations Follow-up with Otolaryngology/Head and NeckSurgery given concerning appearance of rightvocal fold Biopsy right vocal foldContinue with anti-reflux measures per physicianordersFollow-up with Speech Pathology perOtolaryngology
Results Biopsy positive for T1a N0 M0 moderatelydifferentiated squamous cell carcinoma of the rightvocal foldUnderwent definitive XRT using IMRTPost-tx, seen by Speech Pathology X2 for voicetherapy Vocalwarm-ups/cool downs Liptrills Pitch glides/steps on /oo/ VocalFunction Exercises (Stemple)
References Bzoch KR (Ed.): Communicative Disorders Related to CleftLip and Palate, 5th Ed., Pro-Ed, Austin, 2004.Golding-Kushner, K. Therapy Techniques for Cleft palateSpeech & Related Disorders, Singular Thomas Learning, SanDiego, 2001Kummer A, Cleft Palate & Craniofacial Anomalies, 2nd Ed.,Delmar Cengage Learning, New York, 2007Peterson-Falzone, S., Hardin-Jones,M., Karnell, M., CleftPalate Speech, 3RD Ed., Mosby, St. Louis, 2001Peterson-Falzone, S., Trost-Cardamone, J., Karnell, M.,Hardin-Jones, M., The Clinician’s Guide to Treating CleftPalate Speech, Mosby, St. Louis, 2006Stemple, J., Glaze, L., Klaben, B., Clinical Voice PathologyTheory and Management, 4th Ed., Plural Publishing, SanDiego, 2010www.cleftline.org (Cleft Palate Foundation)
C.S. Mott Children’sHospital- Opening 2011Thank youmaberg@umich.edU
Nasal words and sentence stimuli Mama,me me, new new, no no, inga inga Mama made some lemon jam. Nancy is a nurse. The monkey had a banana. Hand the mean dog some meat. The swing is neat and clean. Many men walked many miles. Amanda came from Maine. Santa came when the snow fell. Jane came in when the phone rang.
Oral sentences Buy a baby bib.Pop a bubble.Purple paperDaddy did it.It’s too tight.Go get it.Cookie and cakeChocolate chipcookies Dick took Patty.Peter had a puppy.Buy a baby bib.Tell Dad to do it.Katy had a cookie.Go get a big egg.I see a black dog.Zippers are easy.
Oral sentences Sissy sees the sky.Shoes and socksStop the bus.Should I wash the dishes?Zippers are easy to close.Jack had a magic badge.Chad’s teacher was at church.Check your watch.Chocolate chip cookies are delicious.Go get a big egg.
Feb 08, 2010 · EVERYTHING YOU ALWAYS WANTED TO KNOW ABOUT VOICE AND RESONANCE DISORDERS BUT WERE AFRAID TO ASK (I.E. THE MARY AND MARC VELUM AND LARYNX SHOW) Marc Haxer M.A.CCC and Mary K Berger M.