Transcription
HindawiInternational Journal of EndocrinologyVolume 2018, Article ID 4095789, 9 pageshttps://doi.org/10.1155/2018/4095789Review ArticleThe Gut Microbiome Profile in Obesity: A Systematic ReviewOlga Castaner ,1,2 Albert Goday,2,3,4 Yong-Moon Park,5 Seung-Hwan Lee ,6Faidon Magkos,7 Sue-Anne Toh Ee Shiow,8,9,10 and Helmut Schröder 1,111Cardiovascular Risk and Nutrition Research Group, Hospital del Mar Research Institute (IMIM), Barcelona, SpainCIBER de Fisiopatología de la Obesidad y Nutrición (CIBEROBN), Santiago de Compostela, Spain3Department of Endocrinology and Nutrition, Hospital del Mar Research Institute, Barcelona, Spain4Department of Medicine, University Autònoma de Barcelona and Universitat Pompeu Fabra, Barcelona, Spain5Epidemiology Branch, National Institute of Environmental Health Sciences, National Institutes of Health, Research Triangle Park,NC, USA6Division of Endocrinology & Metabolism, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, TheCatholic University of Korea, Seoul, Republic of Korea7Department of Physiology, Yong Loo Lin School of Medicine, National University of Singapore (NUS) and Clinical NutritionResearch Centre (CNRC), Singapore Institute for Clinical Sciences (SICS), Agency for Science,Technology and Research (A STAR), Singapore8Yong Loo Lin School of Medicine, National University of Singapore, Singapore9Division of Endocrinology, Department of Medicine, National University Health System, Singapore10Regional Health System Planning and Development, Singapore11CIBER de Epidemiologia y Salud Pública (CIBERESP), Madrid, Spain2Correspondence should be addressed to Olga Castaner; ocastaner@imim.es and Helmut Schröder; hschroeder@imim.esReceived 27 October 2017; Accepted 3 January 2018; Published 22 March 2018Academic Editor: Małgorzata Kotula-BalakCopyright 2018 Olga Castaner et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.Gut microbiome has been identified in the past decade as an important factor involved in obesity, but the magnitude of itscontribution to obesity and its related comorbidities is still uncertain. Among the vast quantity of factors attributed to obesity,environmental, dietary, lifestyle, genetic, and others, the microbiome has aroused curiosity, and the scientific community haspublished many original articles. Most of the studies related to microbiome and obesity have been reported based on theassociations between microbiota and obesity, and the in-depth study of the mechanisms related has been studied mainly inrodents and exceptionally in humans. Due to the quantity and diverse information published, the need of reviews is mandatoryto recapitulate the relevant achievements. In this systematic review, we provide an overview of the current evidence on theassociation between intestinal microbiota and obesity. Additionally, we analyze the effects of an extreme weight loss interventionsuch as bariatric surgery on gut microbiota. The review is divided into 2 sections: first, the association of obesity and relatedmetabolic disorders with different gut microbiome profiles, including metagenomics studies, and second, changes on gutmicrobiome after an extreme weight loss intervention such as bariatric surgery.1. IntroductionObesity is known to be a major public health problem thataffects more than 1.9 billion adults, which means 39% ofadults are considered obesity and overweight [1]. Estimationsfrom the noncommunicable diseases (NCD) collaborationreported that if these trends continue, by 2025, global obesityprevalence will reach 18% in men and surpass 21% inwomen; severe obesity will surpass 6% in men and 9% inwomen [2]. Obesity is associated with multiple pathologies,among them cardiovascular diseases, metabolic syndrome,and cancer [3].The latest public statements report the attributable deathsto obesity. The Global BMI Mortality Collaboration reported
2that mortality increased with body mass index (BMI) approximately in a log-linear manner and that the associations ofboth overweight and obesity with higher all-cause mortalitywere broadly consistent in four continents [4].Another troubling factor is the increase of childhood obesity, which is known to be a risk factor for obesity in adults [5].Gut microbiota has captured our attention in the lastdecade as an element that directly affects our health or disease status. In particular, it has been implicated in the aetiology of obesity [6]. In fact, the composition of gut microbiotaseems to play a role concerning obesity.Gut microbiota is considered as an assortment of microorganisms that inhabit the gastrointestinal tract. The composition of this microbial community depends on the host, but itcan also be modified by exogenous and endogenous events [7].With regard to the host, these bacteria are symbiotic, andplay an important role in physiological processes, for example, in digestion, or they can intervene in the metabolism,as they can increase energy production from the diet and takepart in the regulation of the fatty acid tissue composition [8].The different bacteria can also induce low-grade inflammation. All these processes are involved in obesity and metabolic disorders.With the introduction of human whole metagenomestudies, the associations of microbiota and disease were plausible and many have been encountered.It is known that most of the human’s populations microbiota is composed by 5 phyla Bacteroidetes, Firmicutes, Actinobacteria, Proteobacteria, and Verrucomicrobia [9] beingBacteroidetes and Firmicutes around 90% of the total bacterial species [9, 10].The composition of the bacterial diversity seems tochange between lean and obese, increasing the number ofFirmicutes to the detriment of Bacteroidetes [9, 11–13] inobese patients and also in type 2 diabetes, which is pathologyin close relationship to obesity. But some recent studies havefound controversial results [9, 11–15]: studies of associationbetween microbiota profiles and different phenotypes orbody mass index have adventured the positive and negativeassociations among the different phyla that populate theintestines. The searches of mechanistic pathways involvedin the contribution of microbiota to obesity or vice versa havebeen subject for many animal studies [10]. An interestingfinding was that obesity-resistant germ-free mice becomeobese and increase their energy harvest and caloric uptakeafter receiving a microbiota transplant [16].The new era of sequencers has widely unlocked theacquirement of information. Sequencing of specific regionsof 16S or 18S ribosomal genes allows the identification oforganisms and their relative abundance in purified DNA[17]. Thus, the sequencing of gut microbiota with 16S rRNAmade an inflexion point in the knowledge and relationshipof the microbial diversity with the different physiopathological states that intervene in health and disease, allowing theobservation of the behavior of the different bacterial phyla,and genus, links with different phenotypes, different typesof diets, and obesity in particular [18]. Furthermore, thedevelopment of high throughput DNA sequencing of shotgun genomic libraries to assess the microbiome (collectionInternational Journal of Endocrinologyof all genes in the microbial genomes), such as the HumanMicrobiome Project, is aiming to contribute to the assessment of the diversity and relative abundance of our commensal microbiota at different sites of our organism andto the understanding of their role on human health anddisease [19].Bariatric interventions have been implemented as a solution to extreme situations of weight gain in the past decades.The techniques have improved with two main variants: theRoux-en-Y gastric bypass (RYGB) and the laparoscopicsleeve gastrectomy (LSG).RYGB and LSG procedures modify the anatomy of thegastrointestinal system, which modulates nutrient transitand impacts gut physiology. They are known to produce along-term reduction in body weight and to decrease bloodglucose levels, both of which are relevant to obesity-relatedtype 2 diabetes and cardiovascular disease. Nevertheless, themechanisms implicated in the metabolic improvements associated with bariatric surgery are still challenging. [20]Some studies have pointed to the effect of surgery on themicrobiota diversity as a partial contribution to the resolution of the metabolic status of these patients [21].This review focuses on the current evidence of theassociations between the microbiota profile and the individuals’ phenotypes and on the effect of bariatric surgeryon gut microbiota.2. Methods2.1. Eligibility Criteria. We assessed observational humanstudies or clinical trials that evaluated the gut microbiota ofindividuals who suffered from obesity. Obesity was definedby body mass index (BMI). We also selected observationalstudies of extreme weight loss interventions, such as bariatricsurgery, but did not include dietary interventions, becausethere is a lack of homogeneity, and many reviews havealready focused on this theme.We selected the MeSH terms “Obesity” AND “Microbiota,” with the following filters: language: English, French,and Spanish; publication date: 5 years from August 20,2017. The search was performed in MEDLINE accessed byPubMed. All of them were screened based on the title andabstract.Other possible articles were screened and searched on thereference lists of the selected articles. With the reading of thetitle or title and the abstract, we selected observational studiesand clinical trials, and systematic reviews, in humans.3. Results3.1. Literature Search. General characteristics of the studiesare as follows: From the 570 articles retrieved from thesearch, 83 articles were selected based on the title andabstract to be read in depth. Finally, 15 studies were includedand are described in Tables 1 and 2. Eleven articles assesseddifferences in the microbiota profile between obese and lean;most of these studies were performed on adults, but 3 of themwere performed on children. Four articles assessed the effectson microbiota of bariatric surgery. 68 were discarded
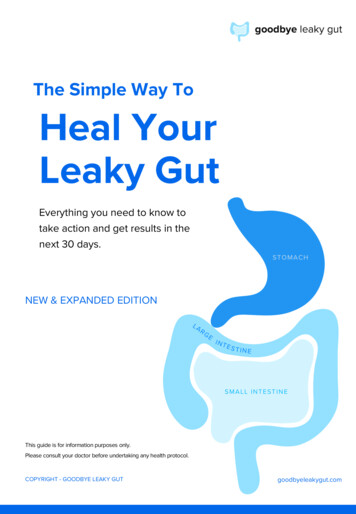
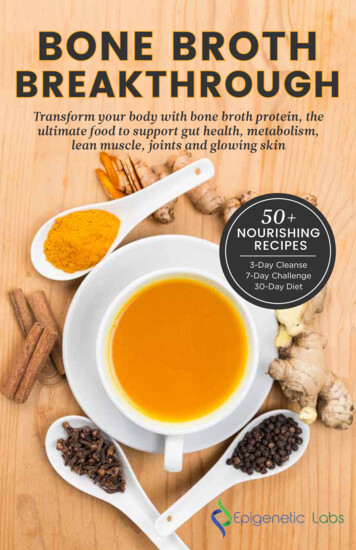
International Journal of Endocrinology3Table 1: Lean/obese clinical trials.StudyidentificationDescriptionKasai et al.2015 [22]Cross-sectional studyMicrobiota fecal samples16S DNA sequencingMetagenome@KIN softwareCorresponding OTU identifiedaccording to T-RFLPMillion et al.2012 [23]Cross-sectional studyMicrobiota fecal samplesqPCR targeting Firmicutes,Bacteroidetes, Lactococcus lactis,Methanobrevibacter smithii, andBifidobacterium animalisHaro et al.2016 [24]Cross-sectional studyBaseline fecal samples16S rRNA sequencingNLin et al.2015 [25]Angelakiset al. 2015[26]Bacterial diversity was significantly greater inobese subjects compared with nonobesesubjects.Reduced numbers of Bacteroidetes and ahigher F/B ratio in obese subjects comparedwith nonobese subjects.115L. reuteri was associated with obesity.M. smithii was depleted in obese subjects.Some Bifidobacterium or Lactobacillus specieswere associated with normal weight(B. animalis).7568 obese and 47 controlsF/B ratio changed with the BMI and between39 men and 36 women withgenders.CVD within CORDIOPREVMen had higher F/B ratio under a BMI of 33.studyBy contrast, men had a significantly lower F/B3 groups according to BMI:ratio than women in the BMI 33 group.BMI 30, 30 BMI 33, andAt genera level, BMI 33: higher BacteroidesBMI 33genus in women, but decrease in men.Healthy Chinese adultsAsian: normal BMI 23 (N 659 281), overweight 23- 27.5 (N 304), and obese 27.5 (N 55)Cross-sectional studyDuodenal microbiota16S rDNA sequencing105 lean subjects: BMI 20.75 obese subjects: BMI 36.8Illumina MiSeqFinucaneet al. 2014[27]Goodrichet al. 2014[30]Review of 4 different studies HumanMicrobiome Project (HMP) andMetaHITCross-sectional studyFecal samples from the twins UKpopulation16S rRNAIllumina MiSeqQIIME softwareOutcomesJapanese population: 23BMI 20 kg/m2 and 3356BMI 25 kg/m2(10)Subsample: 4 nonobese and 6obese subjectsQIIME softwareCross-sectional studyUpper gastrointestinal microbialdiversity16S rRNA sequencingHOMIM softwarePopulation descriptionBMI was not associated with the bacterialcommunity diversity as assessed by alphadiversity in the models.Firmicutes and Actinobacteria were the mostpredominant phyla of the bacterialcomposition of the duodenal microbiota inboth groups.The obese group presented a higherproportion of anaerobic genera and a lesserproportion of aerobic genera, mostlyassociated with the presence of Veillonella,Bulleidia, and Oribacterium.159The interstudy variability in the taxonomiccomposition of stool microbiomes far exceedsdifferences between lean and obeseHMP project: 24 obeseindividuals within studies. No quantitative(BMI 30) and 123 leanassociation between the continuous BMI(BMI 25) individualsvariable and the ratio of B/F. Variation in theMetaHIT project: DanishMetaHIT cohort included 12 relative abundance of F and B is much largeramong studies than between lean and obeseindividuals (BMI 35)individuals within any study. MetaHIT andHMP go in the opposite direction [11].977The family Christensenellaceae wassignificantly enriched in subjects with aBMI 25 compared to those with BMI 30.Overall, a majority (n 35) of the OTUs withhighest heritability scores were enriched inthe lean subjects. A subset of OTUs classifiedas Oscillospira were enriched in lean subjects,and M. smithii, though not significantlyheritable, was positively associated with a leanBMI.Twin population: 416 twinpairs, mostly females, meanage 60.6 0.3 yearsN 433: BMI 25N 322: BMI 25–30N 183: BMI 30
4International Journal of EndocrinologyTable 1: ctional studyFecal samplesBondia-PonsDiversity of the major bacterial groupset al. [35]by using 5 different validated bacterialgroup-specific DGGE methodsMurugesanet al. [31]Ignacio et al.[32]Hu et al. [33]Cross-sectional studyCross-sectional studyCross-sectional study fecal samplesfrom 67 obese (BMI 30 kg/m2) and67 normal (BMI 25 kg/m2)individuals50190Population descriptionOutcomes16 healthy monozygotic twin No differences in fecal bacterial diversity werepairs discordant for weight detected when comparing cotwins discordant(BMI difference 3 kg/m2)for weight. We found that within-pairControl pairs: ninesimilarity is a dominant factor in theconcordant monozygoticmetabolic postprandial response,pairsindependent of acquired obesity.190 unrelated Mexicanchildren9–11 years old81 normal29 overweight80 obeseNo statistical significant differences inabundance of phylum.84B. fragilis group and Lactobacillus spp. werefound at high concentrations in obese andoverweight children when compared with thelean ones and positively correlated with BMI.30 obese, 24 overweight, andBifidobacterium spp. were found in higher30 lean childrennumbers in the lean group than the(3–11 years old)overweight and obese ones. Furthermore, anegative correlation between BMI andBifidobacterium spp. copy number wasobserved.134No significant differences in theBacteroidetes, Firmicutes, and Proteobacteriapopulations in samples from normal andobese adolescents at the phylum level,although the proportion of Bacteroides washighest in normal children (45%), whereasthat in obese was 25%. Conversely, theproportion of Prevotella in BMI 25 was16%; obese adolescents (35%).Korean adolescents aged13–16 yearsT-RFLP reference human fecal microbiota profiling; qPCR: quantitative PCR; CVD: cardiovascular disease; DGGE: denaturing gradient gel electrophoresis.including the reviews which we read but did not include inthe study except if they were systematic (see Figure 1 ofSupplementary Materials).All the studies had a baseline assessment of the gutmicrobiota, and the changes in microbial composition wereassessed as outcomes.The 11 studies compared a baseline assessment of gutmicrobiota from different individual phenotypes whereasthe 4 studies which involved bariatric surgery compared thebaseline assessment with the change after surgery at differenttime points within each subject.Most of the studies were performed in Europe (75%),America (33%), and Asia (25%).Several molecular biology techniques were used to assessthe characterization of the gut microbiome: denaturing gradient gel electrophoresis (DGGE), fluorescence in situ hybridization probes (FISH), metagenomics shotgun sequencing,and characterization of the 16S rRNA genes in a sample, andgroups specific real-time polymerase chain reaction (PCR)are some of the assays. Some studies have made a step forwardand published results of functional analysis of the gut microbiota and metabolome. We have focused on the analysis ofthe diversity of microbiota among BMI.With regard to the time of publication, more than 50%were published in the last 2 years 2015–2017.3.1.1. The Association of Obesity and Related MetabolicDisorders with Different Gut Microbiome Profiles. Amongthe latest studies on microbiota profile between lean andobese patients, several studies searched for differential gutmicrobiota signatures associated with obesity. We found 11interesting studies, which compare microbiota in individualswith different BMIs.The first reported study observed that the bacterial diversity was significantly greater in obese subjects compared withnonobese subjects [22]. Next-generation sequencing revealedthat obese and nonobese subjects had different gut microbiota compositions and that certain bacterial species were significantly associated with each group. This study also agreesthat the ratio Firmicutes/Bacteroidetes (F/B) was higher inobese subjects and also overweight subjects (BMI 25) [22].In the case of the individuals who suffered from obesity,there was a strong association with the following bacterialspecies from the Firmicutes phylum: Blautia hydrogenotorophica, Coprococcus catus, Eubacterium ventriosum, Ruminococcus bromii, and Ruminococcus obeum. On the other hand,
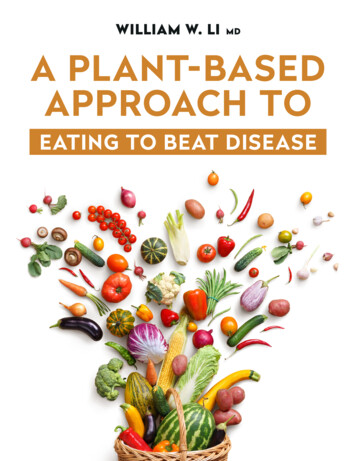
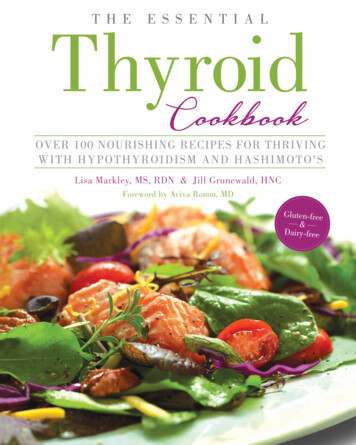
International Journal of Endocrinology5Table 2: Bariatric surgery clinical trials.StudyidentificationPalleja et al.2016 [36]DescriptionTremaroliet al. 2015[29]Shotgun sequencingClinical trialFecal samplesGraessleret al. 2013[37]Population descriptionOutcomesLongitudinal observational studyGut microbial diversity increased withinthe first 3 months after RYGB andFecal samplesParticipants were recruited forremained high 1 year later. RYGB led toQuantification of gut microbiomes atbariatric surgery: BMI 40 kg/m2 or altered relative abundances of 31 species:baseline (n 13), 3 months (n 12) 13BMI 35 kg/m2 with T2D/Escherichia coli, Klebsiella pneumoniae,after RYGB, and 12 months (n 8)hypertensionVeillonella spp., Streptococcus spp.,after RYGBAlistipes spp., and Akkermansia16S rDNA shotgun sequencingmuciniphila.Clinical trialFecal samples16S rDNAIllumina HiSeq 2000DammsMachadoet al. 2015[34]NSOLiD long-mate-paired shotgunsequencingSignificant differences in microbiotacomposition for RYGB versus OBSsamples but not for LSG versus OBS orRYGB versus LSG.Weight-stable women 9 years after29 microbial genera differed significantlyrandomization to either RYGB orbetween RYGB and controls:LSG and matched for weight and fat Gammaproteobacteria class and threemass lossspecies in the Firmicutes phylum21Control: 2 groups of nonoperated(C. difficile, C. hiranonis, andwomen with BMI matched toG. sanguinis).patients’ (1) presurgical BMI and (2)At the genus level:postsurgical BMI Proteobacteria (Escherichia, Klebsiella,and Pseudomonas) in RYGB.No different microbiota profiles for RYGBand LSG patients.10 unrelated subjects with obesitygrade III at 3 time points:(1) baseline10(2) 3 months after LSG(3) 6 months after LSG (N 5) ordietary weight loss regimen (N 5)Both interventions resulted in changes ofthe B/F ratio but with an inverserelationship between the main phyla.LSG: Bacteroidetes and FirmicutesDietary intervention: Bacteroidetes and FirmicutesIn LSG: Bacteroidetes correlatednegatively with weight. Firmicutespositively correlated with weight.3 men and 3 women, recruited forRYGB38–53 yearsPreoperative BMI 40.9–52.1 Firmicutes, Bacteroidetes,Actinobacteria, and Cyanobacteria.However, the ratios of B/F shifted from0.99 to 1.31, showing an apparent increase. Proteobacteria, Verrucomicrobia, andFusobacteria.3 months after RYGB, E. cancerogenus,Veillonella parvula, V. dispar, Shigellaboydii, and Salmonella entérica.Postoperative abundances of these specieswere also significantly higher than those inlean controls.Clinical trialFecal samples16S rDNAIllumina HiSeq 20006Shotgun sequencingBMI: body mass index, expressed as kg/m2; RYGB: Roux-en-Y gastric bypass; LSG: sleeve gastrectomy.in the lean individuals, there was a larger proportion of theBacteroidetes phylum species Bacteroides faecichinchillaeand Bacteroides thetaiotaomicron and also Firmicutes Blautia wexlerae, Clostridium bolteae, and Flavonifractor plautii.In agreement with these results, another study with a focusedapproach also observed that Firmicutes (L. reuteri) was associated with obesity and another genus Methanobrevibactersmithii was decreased. In this case, the authors focuseddirectly on targeting Firmicutes, Bacteroidetes, Methanobrevibacter smithii, Lactococcus lactis, and Bifidobacterium animalis, by quantitative PCR and cultures [23].Furthermore, a third party was introduced with gender,in a study with the aim at observing differences in microbiotabetween genders, but reported that the differences in gendercould be influenced by BMI [24]. They observed that the F/B ratio changed along with BMI, as it had been describedbefore [22], and also by gender. The F/B ratio tended toincrease with BMI up to 33 and decreased surprisingly whenBMI was 33. In men, Bacteroidetes genus decreased whenthe BMI increased, but no changes were observed in women.The methodologies differ between these studies. In oursequence of studies, the three assessments were performed
6in fecal samples of adult individuals who suffered from obesity comparing with normal weight adult individuals. Thetwo first studies were performed by metabarcoding 16SrRNA [22, 24], and the third one used a different methodology with a focused approach on PCR and cultures [23].Two of these studies were performed in Europe and theother one in Asia [22]; this fact is important because BMIcategories differ between Asia and Europe.Another two publications analyzed the upper gastrointestinal microbial diversity [25, 26] compared to the abovementioned studies that assessed microbiota from fecal samples. None of these two studies of microbiota from the uppergastrointestinal tract and duodenum found differences in themicrobiota diversity in terms of phyla, which may suggestthat the impact of obesity might affect the lower portions ofthe gastrointestinal tract.The analysis of the upper gastrointestinal microbialdiversity did not find association among the bacterial community with obesity. Alpha diversity was not associated withobesity but beta diversity was. The microbiome was characterized using the 16S rRNA gene DNA microarray (theHOMIM array), which uses 16S rRNA-based oligonucleotideprobes printed on glass slides. They also used anotherapproach to search for diversity in the community and foundthat BMI was not associated with the bacterial communitydiversity as assessed by alpha diversity in their models afteradjusting for multiple potential confounders. However,BMI was significantly associated with the variation in thecommunity composition, as assessed by multiple betadiversity parameters. As a limitation in this study, the microarray was only semiquantitative and contained a limitednumber of bacterial species. As a microarray based on the16S rRNA gene, this assay did not produce data that couldbe used to determine categories of bacterial functions.Another study performed in upper gastrointestinaltract, studying the microbiota of duodenum [26], alsoreported that there were no differences between obese andlean among the microbiota phyla. The only differencesfound were in the relative abundance of aerobic and anaerobic, being the obese population, presenting a higherproportion of anaerobic genera, mostly Veillonella, Bulleidia, and Oribacterium.A very interesting study [27] aimed at confirming someprevious published results of studies of considerable magnitude, such as the HMP (Human Microbiome Project fromthe NIH) and the MetaHIT project, and also at comparingthem with two previous studies of high reputation [11, 28].The researchers analyzed all the results together and couldnot find an association, so no difference was found betweenobese and lean individuals in their relative abundance of Bacteroidetes or Firmicutes. And interestingly, it was found thatthe variation in the relative abundance of Firmicutes andBacteroidetes was much larger among studies than betweenlean and individuals who suffered from obesity within anystudy. The relevance of this specific article is that it gives scientific justification that there are some real statisticallyproved discrepancies among the studies and that MetaHITand HMP not only do not recapitulate the findings observedbut even go in the opposite direction. So, at this point, noInternational Journal of Endocrinologysignificant association between BMI and taxonomic composition at the phylum level could be found.Other studies have been performed in twin pairs, whichprovide more information about the heritability of microbiota: one of the studies analyzed fecal samples of healthymonozygotic (MZ) twin pairs which were discordant inweight and compared them with other concordant BMI twinpairs [29]. Their results demonstrated that within-pair similarity was a dominant factor independent of acquired obesity.Another study [30] that wanted to assess which specifictaxa within the gut microbiome are heritable and to whatextent and how do heritable microbes relate to host BMI.They compared fecal samples from twins and found agreater similarity of microbiota within twin pairs compared to unrelated individuals.The most heritable taxon overall was the family Christensenellaceae (Firmicutes phylum), which associates with a lowBMI. The family Christensenellaceae was significantlyenriched in subjects with a lean BMI ( 25) compared tothose with an obese BMI ( 30).Within the three most dominant bacterial families, fromthe Firmicutes phylum and families Ruminococcaceae andLachnospiraceae, there was a significantly greater similarityfor MZ twins compared to dizygotic (DZ) twins, in contrastwith the Bacteroidaceae family, in which MZ and DZ twinshad similar pairwise diversity. Therefore, Firmicutes seemsto have more heritability.Three studies have focused their attention on gut microbiota association to obesity in children. Two of them wereperformed in Central and South America in children up to11 years old. Another study performed in youngsters aged13–16 was performed in Asia.A Mexican study [31] in 190 children did not find statistical differences between phyla. Despite that, several generaand families, from the Firmicutes phylum as well as someEnterobacteriaceae, increased in overweight and obese children: the genus Faecalibacterium sp., the family Lachnospiraceae, and the genus Roseburia sp. A decrease in the genusSuccinivibrio sp., the genus Erwinia sp. from the Proteobacteria phylum, and the genus Oscillospira sp. from the Firmicutes phylum was found.The genus Blautia sp., the genus Coprococcus sp., and thefamily Enterobacteriaceae from the Firmicutes phylum wereclearly increased in the overweight phenotype. Another studyin 30 obese children (3–11 years) found that there were highconcentrations of B. fragilis group and Lactobacillus sp. inobese and overweight children when compared with the leanones, with the fecal concentrations positively correlated withBMI [32]. Furthermore, a negative correlation between BMIand Bifidobacterium spp. was observed.In contrast, another study in Korean adolescents did notfind any significant differences in the Bacteroidetes, Firmicutes, and Proteobacteria populations in samples from normal and obese adolescents at the phylum level [33].However, there was a marked difference in the average proportions of Bacteroides and Prevotella between normal andobese samples at the genus level. This trend persisted at thefamily level. A significant association was found betweenthe compositions of several bacterial taxa and child obesity,
International Journal of Endocrinologywith the proportion of Bacteroides highest in normal childrencompared to those who suffered from obesity.With regard to the metabolically healthy obese subject, defined as those subjects which have normalizedlevels of the parameters that are used to define metabolicsyndrome (blood pressure, HDL cholesterol levels, glycaemia, and visceral fat), there is no literature characterizingthe microbiota profile of these subjects. Such findingswould be interesting to understand whether the microbialdiversity has a metabolic role in individuals who sufferedfrom obesity.3.1.2. Bariatric Surgery Weight Loss Impact on GutMicrobiota. We have found 4 articles in the last 5 years tolook for the effect of bariatric surgery on the microbiota profile. All four studies analyze the results comparing with abaseline before the intervention and have a follow-up of 6months to 1 year. Two of them studied the changes afterRYGB surgery, another one LSG, and another one includedboth types of surgery.Palleja et al. found that after RYGB surgery, the microbialdiversity increased and this diversity was maintained oneyear after surgery [36]. Another study that included the twotypes of surgery only found an increased diversity in theRYGB group whether there were no differences betweenindividuals who suffered from obesity, and the LSG group,which lead us to think that maybe the type of surgery andnot the weight loss is playing a role in the diversity.Opposit
Additionally, we analyze the effects of an extreme weight loss intervention such as bariatric surgery on gut microbiota. The review is divided into 2 sections: first, the association of obesity and related metabolic disorders with different gut microbiome profiles, i