Transcription
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeThe Female Predominant Persistent Immune Dysregulation of the Post COVID Syndrome:A Cohort StudyRavindra Ganesh MBBS, MD1; Stephanie L. Grach MD, MS2; Aditya K. Ghosh MD3; DennisM. Bierle MD1; Bradley R. Salonen MD1; Nerissa M. Collins MD1; Avni Y. Joshi MD MS4;Neal D. Boeder Jr MD1, Christopher V. Anstine MD1, Michael R. Mueller MD MS1, ElizabethC. Wight MD1, Ivana T. Croghan PhD1, Andrew D. Badley MD5, Rickey E. Carter PhD6, Ryanre-ProofT. Hurt MD PhD1urnalPAuthor AffiliationsDivision of General Internal Medicine, Mayo Clinic, Rochester, MN;2Mayo Clinic School of Graduate Medical Education, Rochester, Minnesota;3Department of Internal Medicine, Northeast Georgia Medical Center, Gainesville, Georgia;4Division of Allergy and Immunology, Mayo Clinic, Rochester, Minnesota;5Division of Infectious Disease, Mayo Clinic, Rochester, Minnesota;6Department of Quantitative Health Sciences, Mayo Clinic, Jacksonville, FloridaUncorrectedJo1Corresponding Author:Ravindra Ganesh MBBS, MD200 First Street SWRochester, MN 55905ganesh.ravindra@mayo.edu 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 1
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeAuthor Contributions: RG, SLG, AKG, DMB, BRS, NMC, AYJ, NB, CVA, MRM, ECW,ITC, ADB, REC, and RTH made substantial contributions to the concept and design of the study,the interpretation of data, and the critical revision of the manuscript for important intellectualcontent, made substantial contributions to the acquisition of data, the analysis and interpretationof data, drafting of the manuscript, and substantial contributions to critical revision of themanuscript for important intellectual content.oofConflict of interest:re-PrRG, SLG, AKG, DMB, BRS, NMC, AYJ, NDB, CVA, MRM, ECW, ITC, and REC have nolPconflicts to report.urnaADB is supported by grants from NIAID (grants AI110173 and AI120698) Amfar (#109593)Joand Mayo Clinic (HH Sheik Khalifa Bib Zayed Al-Nahyan Named Professorship of InfectioustedDiseases). ADB is a paid consultant for Abbvie and Flambeau Diagnostics, is a paid member ofrecthe DSMB for Corvus Pharmaceuticals, Equilium, and Excision Biotherapeutics, has receivedncorfees for speaking for Reach MD, owns equity for scientific advisory work in Zentalis andNference, and is founder and President of Splissen therapeutics.URTH is a consultant for Nestle.REDCap software provided via internal grant UL1TR002377A preliminary report of this work was previously published on medRxiv, Posted June 02, 2021.DOI: https://doi.org/10.1101/2021.05.25.21257820 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 2
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeAbstractObjective:To describe the clinical data from the first 108 patients seen in the Mayo Clinic Post COVID-19Care Clinic (PCOCC).Patients and Methods:After IRB approval, we reviewed the charts of the first 108 patients seen between January 19,oof2021 and April 29, 2021 in the PCOCC and abstracted from the electronic medical record into aPrstandardized database to facilitate analysis. Patients were grouped into phenotypes by expertre-review.urnalPResults:The majority of patients seen in our clinic were female (75%, 81/108), and the median age atJopresentation was 46 years (interquartile range [IQR] 37, 55). All had Post Acute Sequelae oftedSARS-CoV-2 infection (PASC) with six clinical phenotypes being identified – fatiguerecpredominant (n 69), dyspnea predominant (n 23), myalgia predominant (n 6), orthostasisncorpredominant (n 6), chest pain predominant (n 3), and headache predominant (n 1). Thefatigue-predominant phenotype was more common in women and the dyspnea-predominantUphenotype was more common in men. IL-6 was elevated in 61% of patients (69% of women,p 0.0046) which was more common than elevation in CRP and ESR which were identified in17% and 20% of cases respectively.Conclusion:In our post COVID clinic, we observed several distinct clinical phenotypes. Fatiguepredominance was the most common presentation and was associated with elevated IL-6 levelsand female gender. Dyspnea-predominance was more common in men and was not associated 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 3
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndromewith elevated IL-6 levels. IL-6 levels were more likely to be elevated in patients with PASC thanESR and CRP.Abbreviations:COVID-19 – Coronavirus Disease 2019oofCRP - C-reactive proteinre-PrCS - central sensitizationlPESR – Erythrocyte Sedimentation RateurnaGIM - General Internal MedicinePCOCC - Post COVID-19 Care ClinictedPoCoS - post-COVID syndromeJoPASC - Post-acute Sequelae of SARS-CoV-2 infectionrecPOTS - postural orthostatic tachycardia syndromencorSARS - Severe Acute Respiratory SyndromeUSARS-CoV-2 - Severe Acute Respiratory Syndrome Coronavirus 2 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 4
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeIntroductionSince its identification in December 2019, the SARS-CoV-2 virus, which causes CoronavirusDisease 2019 (COVID-19), has had a devastating global impact with over 4.7 million deathsworldwide as of September 2021. In addition to mortality, patients have been left with significantdebility after recovering from acute COVID-19. The earliest report of this condition was a caseseries from Italy of 143 patients who had been hospitalized for COVID-19. In this population,oofpersistent symptoms were observed over 60 days from initial onset in 87.4% of cases, with are-Prpredominance of fatigue (53.1%), dyspnea (43.4%), joint pain (27.3%), and chest pain (21.7%)lPduring outpatient follow-up.1 These findings were confirmed in a subsequent 6-month cohorturnastudy of 1733 patients from Wuhan, China, which again demonstrated persistent fatigue ormuscle weakness (63%), as well as sleep difficulties (26%) and anxiety and depressionJo(23%).2, Recent studies have estimated that between 10-30% of patients who recover fromtedCOVID-19 experience persistent symptoms months after resolution of acute illness.1-7 Theserecpersistent symptoms have been described using several terms including post-COVID syndromencor(PoCoS), post-acute COVID-19, and long-haul COVID.4-7 Recently the National Institutes ofUHealth (NIH) developed the term Post-Acute Sequelae of SARS-CoV-2 infection (PASC) todescribe those COVID-19 patients that have at least one symptom that developed after the acuteinfection and has persisted after the expected resolution of acute disease.Direct organ damage from COVID-19 has been observed in PASC patients with single-systeminvolvement such as anosmia, cardiomyopathy, neuropathy, or interstitial lung disease (ILD).Causes of disability beyond lingering effects of direct organ damage include widespread pain, 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 5
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndromefatigue with post-exertional malaise, orthostatic intolerance, and cognitive impairment includingthe commonly reported “brain fog”. This cluster of symptoms is similar to that seen in other postinfectious syndromes in which may progress to fibromyalgia (FM), chronic fatigue syndrome(CFS), postural orthostatic tachycardia syndrome (POTS), and other central sensitization (CS)syndromes. These CS syndromes are thought to share common pathophysiology with centralneuroinflammation and remodeling of brain and spinal cord pathways leading to enhancedoofsensitivity to multiple stimuli, sympathetic hyperactivity, and decreased efficacy of inhibitoryre-Prpathways.8-19urnalPResearch in CS has recently turned to the role of proinflammatory mediators in the developmentand persistence of these conditions.20 Prominent cytokine and chemokine elevations haveJoincluded IL-6, IL-8, IL-17, IL-1β, and TNF-α.20-22 High sensitivity CRP has been found to betedcomparably elevated in both fibromyalgia and chronic fatigue syndrome, with mixed data onrecelevated CRP.23 Not surprisingly, there has been similar interest in the cytokine releasencorsyndrome attributed to severe cases of COVID-19, especially in regards to IL-6.24 The potentialUoverlap between the inflammatory response of CS and PASC has not yet been determined.In response to the COVID-19 pandemic and the rising cases of PASC, our institution developeda multi-specialty team to coordinate efforts and share clinical and research approaches to PASC.This multispecialty team comprise physicians and scientists from General Internal Medicine(GIM), Preventative Medicine (Prev Med), Physical Medicine & Rehabilitation (PM&R),Psychology, Allergy and Immunology, Infectious Disease (ID), Pulmonology, Neurology,Cardiology, Pediatrics and Otorhinolaryngology (ENT). Subspecialists experienced in acute 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 6
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeCOVID-19 and PASC directly see patients with symptoms limited to their specific organ system,while the GIM (PCOCC) and Prev Med (CARP) clinics evaluate patients with multiple affectedsystems.25Herein we describe the clinical presentation and associated laboratory findings from ourUncorrectedJournalPre-Proofinaugural cohort of 108 patients seen in the Post COVID-19 Care Clinic (PCOCC). 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 7
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromePatients and MethodsThe current study was approved by the Mayo Clinic COVID-19 Research Taskforce and theMayo Clinic Institutional Review Board. The data for all patients in the PCOCC Clinic and hadprovided research authorization were entered into a prospectively maintained internal REDCap(Research Electronic Data Capture) database. Patients seen between January 19, 2021 and April29, 2021 were included. Acute symptoms (within the first 4 weeks of COVID-19 diagnosis oroofsymptom-onset) were recorded, followed by chronic symptoms (those persisting beyond 4 weeksre-Prfrom diagnosis or symptom-onset). Laboratory and other diagnostic testing data (protocollPdescribed below) were also collected as available.urnaStatistical MethodsJoData was abstracted from the electronic medical record and entered into a REDCap (ResearchtedElectronic Data Capture) database.26, 27 Patient’s clinical symptoms were analyzed by reviewersrecand they were assigned to one of 6 phenotypes – dyspnea, chest pain, myalgia, orthostasis,ncorfatigue, and headache-predominant. Lab data was entered from the electronic medical recordexactly with one exception as the lower limit of CRP in our lab is reported as 3.0 µg/L. As weUcould not identify exact values of data below this threshold, this value was entered as 3.0throughout in REDCap. Data was then analyzed using chi-squared analysis to identifydifferences between phenotypes for categorical values such as gender, and ANOVA to identifydifferences between phenotypes for quantitative data. 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 8
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeCare Team DesignPatients who had persistent symptoms post COVID-19 infection were either self- or physicianreferred to the PCOCC. All patients completed a standardized questionnaire which contains 52questions regarding initial COVID-19 infection, symptoms, and treatment, along with ongoingand persistent symptoms that continue to affect them. Patient questionnaires were reviewed by aGIM physician and those with symptoms limited to a single organ system were directly referredoofto the sub-specialty team for management of their PASC symptoms; for example, patients withre-Pranosmia were referred directly to Otorhinolaryngology (ENT). Patients with symptoms inlPmultiple organ systems were initially evaluated via a 30-minute virtual visit for the purpose ofurnaintroducing the PCOCC clinic and appropriate pre-ordering of tests and consults. Patients wouldthen be evaluated in person during a condensed itinerary of tests and consults geared toward theJopredominant symptoms. For patients with no evidence of tissue damage on testing, they weretedlikely to have a central sensitization (CS) phenotype, which was treated with a virtual treatmentrecprogram aimed at patient education with elements of cognitive behavioral therapy, healthncorcoaching, and paced rehabilitation. This program is 8 hours long, delivered as two 4-hourUsegments, and accompanied by health coaching and nursing follow up for 6 months. As part ofthe PCOCC evaluation, the team developed a standardized evaluation to be ordered for anypatient presenting to the clinic. This included basic laboratory testing (CBC, CMP, ESR, CRP),markers of COVID-19 inflammation (ferritin, D-dimer, IL-6), autoimmune screening (ANA andCRP with reflex to full panel if either positive), 6 minute walk test, and pulmonary function testsand chest imaging if patient had dyspnea. 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 9
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeResultsPatient demographics:The first 108 patients evaluated by our PCOCC team were included. Of these, 81 (75%) werefemale with a median age of 46 years (interquartile range [IQR] 37, 55). The average female agewas slightly younger than the overall cohort at 45 years. 94% of our patients wereoofWhite/Caucasian, 4% were Black/African American, and 2% were American Indian/PacificPrIslander. 98% of our patients identified as non-Hispanic and 2% were Hispanic (Table 1). There-most common comorbidities identified in our population were obesity (39%), anxiety (33%),lPdepression (28%), and gastrointestinal disease (25%). Symptoms reported most commonly in theurnaacute COVID-19 infection include fatigue (59%), Cough (58%), shortness of breath (52%), andJomyalgia (50%) (Supplementary Table 1). 16% of our population was admitted for acute COVID-ted19. Patients were evaluated in our clinics on average 148.5 days after the onset of symptomsrec(IQR 111.5, 179.3). At the time of evaluation, the most common symptoms were fatigue (89%),ncorshortness of breath (69%), brain fog (69%), anxiety (62%), and unrefreshing sleep (58%)U(Supplementary Table 2).Phenotypes:Six phenotypes were identified – fatigue predominant (n 69), dyspnea predominant (n 23),myalgia predominant (n 6), orthostasis predominant (n 6), chest pain predominant (n 3), andheadache predominant (n 1) (Table 2). Distribution of phenotypes by sex was unequal withmore women being predominant for fatigue (58/69, 84%), orthostasis (6/6, 100%), and chest 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 10
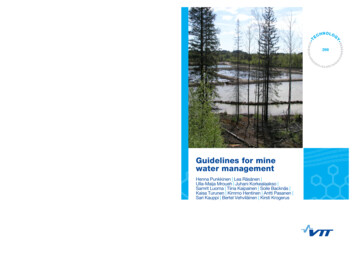
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndromepain (3/3, 100%). More men were predominant for dyspnea (12/23, 52%) and headache (1/1,100%). Myalgia-predominant phenotype was evenly distributed among sexes (3/3, 50%). Thesesex differences by phenotype were statistically significant (p 0.0004)Lab markers:oofLab markers varied significantly with IL-6 elevated in a higher proportion of patients (61%) thanPrCRP (17%) and ESR (20%) (Supplementary Figure 1, Table 2). IL-6 was elevated in are-statistically significant proportion of women (69% vs 39% in men, p 0.05) while there were nolPstatistically significant differences in elevated ESR (18% women vs 26% in men, p 0.76) andurnaCRP (15% in women vs 21% in men) between the sexes (Supplementary Table 3, Table 3). LabJomarkers also varied by phenotype with IL-6 levels being more elevated in patients with thencorCentral sensitization:rectedfatigue-predominant, myalgia-predominant, and orthostasis-predominant phenotypes (Figure 1).UThe fatigue-predominant, myalgia-predominant, and orthostasis-predominant phenotypes wereconsidered together as central sensitization phenotypes given their similarity across groups aswell as similarity to existing CS conditions of chronic fatigue syndrome, fibromyalgia, andPOTS. When considered together against the non-CS phenotype (dyspnea, and chest pain[n 26]), the CS-phenotype (n 82) had statistically significantly higher IL-6 levels (p 0.01) andhigher ESR and CRP levels but these did not reach statistical significance (Supplementary Figure2, Table 2). The CS-phenotype also had a statistically significantly higher proportion of women 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 11
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndrome(82%) than the non-CS phenotype (54%, p 0.0001). Age was not significantly different betweenpatients with CS (mean 45.7, SD 13.6) and without CS (mean 48.7 years, SD 14.8).DiscussionThe main objective of the PCOCC is to phenotype and then treat PASC patients who arestruggling with persistent symptoms for greater than 3 months. There are three major novelooffindings from the first 108 PASC patients seen in the PCOCC: 1) there is female predominancePrin the patients seeking care for PASC (n 81; 75%) 2) females were more likely to have anre-elevated IL-6 than males (69% versus 28%) and 3) ongoing fatigue was the most commonlPphenotype in females (n 58;72%) and dyspnea most common in males (n 12; 52%). Mosturnapatients seen in the PCOCC did not have clear end organ pathology/damage to account for theJoongoing symptoms and central sensitization (CS) phenotype (fatigue, myalgia, orthostasis) wastedthe most common categorization. Of patients with central sensitization phenotypes, 67/82 werencorrecwomen (82%) consistent with the known female predominance in CS (Table 2).29, 30UThe majority (n 62; 57%) of patients seen in the PCOCC clinic had elevated levels of the proinflammatory cytokine IL-6 at least 3 months after acute infection which was highly discordantwith ESR and CRP levels. To our knowledge this has not been described in PASC. AcuteCOVID-19 infection has demonstrated a similar, but more pronounced pattern of inflammatoryresponse similar to what has been seen in other cytokine release syndromes (CRS) such as sepsis,burns, and acute respiratory distress syndrome. The CRS response includes importantcomponents of the innate immune system such as IL-6, IL-8, IL-10 and monocytechemoattractant (MCP)-1.31-35 This innate hyperinflammatory CRS response seen during severe 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 12
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeCOVID-19 is thought to be the primary mechanism behind adverse outcomes. In addition, IL-6has been independently associated with mortality in COVID-19 patients requiring mechanicalventilation.24 It has been postulated that IL-6 inhibits antiviral activity and blockade has beenidentified as a potential therapeutic target,35, 36 however, recent trials of tocilizumab, amonoclonal antibody against IL-6 receptor alpha in hospitalized COVID-19 patients have shownmixed results.37, 38 Further research is needed to determine whether IL-6 levels correlate withre-ProofPASC symptom severity and resolution.lPThe present study demonstrated the persistent (greater than 3 month) elevation in IL-6 level wasurnamore frequent in females, and we hypothesize this could be partially responsible for the sexJodifferences observed in PASC.39-43 Sex is one of several variables known to influence the overalltedimmune responses to COVID-19. In a number of acute COVID-19 cohort studies, males hadrechigher rates of hospitalization, critical illness, and mortality when adjusted for comorbidities andncorage.40, 43, 44 A recent cohort study of hospitalized COVID-19 positive patients who had notreceived immunomodulatory medications and had detailed cytokine, chemokine, and blood cellUphenotyping samples compared to healthy controls found that males had a higher innateinflammatory response (IL-8 and IL-18) than females but when females had elevated innateimmune responses it positively correlated with disease progression.44 Sex-based differences inthe immune response vary throughout the lifecycle with post-puberty/pre-menopausal femaleshaving higher levels of inflammatory cytokines (IL-6, TNF, and IL-1β) compared to postpuberty/adult males. These effects may be mediated by sex hormones estradiol, progesterone, 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 13
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndromeand androgens as this difference changes in older age with men having higher inflammatorycytokine levels as they age.44-46Many patients seen in the PCOCC clinic have clinical presentations very similar to other CSphenotypes such as FMS, CFS and POTS.47-51 Symptoms also overlap with the Post ICUoofSyndrome (PICS) and post-infectious syndromes such as post-treatment Lyme diseasePrsyndrome.47, 52 This centrally sensitized subset of PASC patients are referred to as having postre-COVID syndrome (PoCoS). The presence of a common pathway mediated by immunelPdysregulation provides a common etiology of these conditions and IL-6 is elevated in theseurnasyndromes.53-57 IL-6 is associated with fatigue and sleep-disturbance in chronic stress andJoinflammation in central sensitization syndromes.58 Diagnosis of these conditions havetedtraditionally been frustrating as patients will have multiple disabling symptoms yet will haverecvery few (if any) abnormalities on laboratory and procedural testing. The most compellingncorexplanation is that of central sensitization wherein the brain and spinal cord become moresensitive to stimuli thereby reducing stimulus threshold for perception and amplifying existingUstimuli.59 Changes in the areas of the brain recruited secondary to a standard stimulus varysignificantly between healthy controls and those with CS on both PET-CT and functional MRIbrain imaging.60-63 Besides commonalities in clinical presentation, persistent elevation ofimmune markers, and changes in functional imaging, patients often display symptoms ofpersistent sympathetic system hyperactivity with palpitations, exercise intolerance, difficultyinitiating and maintaining sleep, and sensitivity to external stimuli.48-51 A familial predispositionto central sensitization syndromes has been demonstrated with up to a 13-fold increase in 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 14
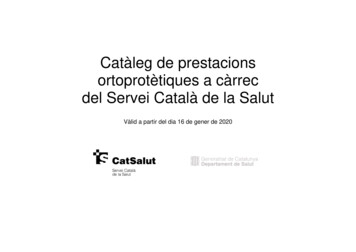
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndromeincidence of CS compared to the general population.64 This suggests a genetic component to CS,which has been supported by several studies identifying genes that occur at a higher frequency inpatients with CS, with fibromyalgia being the best studied of these syndromes.64, 65 Finally, inour experience, patients affected by these syndromes also share personality traits, oftendescribing themselves as “people pleasers” and “detail-oriented”.59 Indeed, there has been someoverlay between the genetics of fibromyalgia and anxiety and these conditions are highlyoofcomorbid.66 With these considerations in mind, we propose a “three hit” hypothesis whereinPrpatients need to have the appropriate candidate genes to have the potential for developing CS, there-personality type associated with CS, and then a “sensitizing event” which causes significanturnalPsystemic distress, often viral in nature, but may include other forms of trauma (life events,physical trauma, surgery, major medical illness) [Figure 2]. The symptoms predominant duringJothe sensitization event often remain as the predominant symptom seen in the illness phenotypetedbut may develop to include other symptoms as the illness progresses. This expansion ofrecsymptoms is likely related to secondary changes including impaired sleep and the distress andUncorconcern due to the impact of symptoms on life and physical activities.This study had several limitations. First, the study design is a prospective cohort without strictinclusion criteria which allows for heterogeneity across the sample population. This wasintentional as the GIM clinic is best suited for evaluating patients with symptoms across multiplesystems. Second, the selection of patients with multiple symptoms increased the concentration ofpatients with PoCoS, as patients with limited symptoms suggestive of one organ systeminvolvement or those with already identified post COVID end organ damage were directly 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 15
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndrometriaged to the appropriate specialty, e.g. anosmia to ENT, pulmonary fibrosis to Pulmonology.This was also intentional as we had designed a treatment program directed at helping theseindividuals. Third, our population was either self-referred or provider-referred which mayintroduce an element of selection bias, thereby diminishing generalizability to the generalpopulation. Fourth, our population was 94% White/Caucasian, and involved no patients ofHispanic descent. This was unintentional and likely secondary to our local demographic andoofdifferences in health seeking behaviors. Therefore, future research in a more diverse populationPris warranted. Fifth, the standard lab panel was not ordered in all patients, which reflects referringre-provider preference or patient-specific clinical decisions. Because of these limitations, our studyurnalPdata may not be widely generalizable to all PASC patients but provides previously unreportedtedJoinsights into PoCoS and its likely immune dysregulation etiology.recConclusionsncorIn our post COVID care clinic, we observed six distinct clinical phenotypes, of which the fatigueand dyspnea-predominant phenotypes were most common in women and men respectively. TheUphenotypes resembling known central sensitization syndromes (fatigue-, myalgia-, andorthostasis-predominant) were collectively considered as post COVID syndrome. This phenotypewas associated with elevated IL-6, predominantly occurred in women, and presented with threemajor subtypes – fatigue, myalgia, and orthostasis. Knowledge of these phenotypes and theinsights gleaned from the clinical data reported in this report may help in defining etiology andtreatment options for PoCoS. 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 16
Mayo Clinic ProceedingsFemale Predominant Post COVID SyndromeReferences1.Carfì A, Bernabei R, Landi F. Persistent Symptoms in Patients After Acute COVID-19.Jama. 2020;324:603-605.2.Garrigues E, Janvier P, Kherabi Y, et al. Post-discharge persistent symptoms and health-covid-19 in primary care. Bmj. 2020;370:m3026.Ladds E, Rushforth A, Wieringa S, et al. Persistent symptoms after Covid-19: qualitativelP4.PrGreenhalgh T, Knight M, A'Court C, Buxton M, Husain L. Management of post-acutere-3.oofrelated quality of life after hospitalization for COVID-19. J Infect. 2020;81:e4-e6.urnastudy of 114 "long Covid" patients and draft quality principles for services. BMC HealthLadds E, Rushforth A, Wieringa S, et al. Developing services for long COVID: lessonsted5.JoServ Res. 2020;20:1144.Logue JK, Franko NM, McCulloch DJ, et al. Sequelae in Adults at 6 Months Afterncor6.recfrom a study of wounded healers. Clin Med (Lond). 2021;21:59-65.COVID-19 Infection. JAMA Netw Open. 2021;4:e210830.Townsend L, Dyer AH, Jones K, et al. Persistent fatigue following SARS-CoV-2U7.infection is common and independent of severity of initial infection. PLoS One.2020;15:e0240784.8.Cook RL, Xu X, Yablonsky EJ, et al. Demographic and clinical factors associated withpersistent symptoms after West Nile virus infection. Am J Trop Med Hyg. 2010;83:11331136. 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 17
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndrome9.Duvignaud A, Fianu A, Bertolotti A, et al. Rheumatism and chronic fatigue, the twofacets of post-chikungunya disease: the TELECHIK cohort study on Reunion island.Epidemiol Infect. 2018;146:633-641.10.Islam MF, Cotler J, Jason LA. Post-viral fatigue and COVID-19: lessons from pastepidemics. Fatigue: Biomedicine, Health & Behavior. 2020;8:61-69.11.Kristiansen MS, Stabursvik J, O'Leary EC, et al. Clinical symptoms and markers ofoofdisease mechanisms in adolescent chronic fatigue following Epstein-Barr virus infection:Leis AA, Grill MF, Goodman BP, et al. Tumor Necrosis Factor-Alpha Signaling Mayre-12.PrAn exploratory cross-sectional study. Brain Behav Immun. 2019;80:551-563.urnalPContribute to Chronic West Nile Virus Post-infectious Proinflammatory State. Front Med(Lausanne). 2020;7:164.Moldofsky H, Patcai J. Chronic widespread musculoskeletal pain, fatigue, depression andJo13.Pedersen M, Asprusten TT, Godang K, et al. Predictors of chronic fatigue in adolescentsncor14.rec2011;11:37.teddisordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol.six months after acute Epstein-Barr virus infection: A prospective cohort study. BrainUBehav Immun. 2019;75:94-100.15.Pedersen M, Asprusten TT, Godang K, et al. Fatigue in Epstein-Barr virus infectedadolescents and healthy controls: A prospective multifactorial association study. JPsychosom Res. 2019;121:46-59.16.Rodriguez-Morales AJ, Simon F. Chronic chikungunya, still to be fully understood. Int JInfect Dis. 2019;86:133-134. 2021 Mayo Foundation for Medical Education and Research. Mayo Clin Proc. 2021;96(x):xx-xx.Page 18
Mayo Clinic ProceedingsFemale Predominant Post COVID Syndrome17.Sejvar JJ, Curns AT, Welburg L, et al. Neurocognitive and functional outcomes inpersons rec
Jun 02, 2021 · and Mayo Clinic (HH Sheik Khalifa Bib Zayed Al-Nahyan Named Professorship of Infectious Diseases). ADB is a paid consultant for Abbvie and Flambeau Diagnostics, is a paid member of the DSMB for Corvus Pharmaceuticals, Equilium, and Excision Biotherapeutics, has received . Mayo Clinic Institutional