Transcription
@PraedFoundationTCOMConversations.orgTCOM & Santa Clara CountyCANS 5 : TreatmentPlanningApril D. Fernando, PhD, Policy FellowChapin Hall at the University of Chicago1313 E 60th Street, Chicago, IL 60637 www.chapinhall.org e: afernando@chapinhall.org
Syllabus . 1Tip Sheet. 2Practice Vignette(s) . 3Treatment Planning . 4Trainer Contact Information:April D. Fernando, PhD, Policy FellowChapin Hall at the University of Chicagoafernando@chapinhall.org
@PraedFoundationTCOMConversations.orgMeaningful Use of the CANS: Collaborative Treatment PlanningApril D. Fernando, PhD,Policy Fellow, Chapin Hall at the University of ChicagoDate and Time:June 4, 20199:00 AM – 12:00 PM; 1:00 PM – 4:00 PMLocation:1075 E. Santa Clara St, 2nd FloorSan Jose, CA 95116Course Description:Transformational Collaborative Outcomes Management (TCOM) facilitates the understanding of theneeds and strengths of the person or people served, and brings to bear effective interventions that will helpchange lives. The Child and Adolescent Needs and Strengths (CANS) the means by which TCOMhappens. A person-centered tool that provides valuable information to youth, caregivers and providers, theCANS helps with decision support and planning. The planning process, however, is often neither transparentnor collaborative, and may not always be data-driven. This workshop will provide a refresher on core TCOMconcepts, the fundamentals of teaming, collaborative assessment and consensus building when using theCANS. A framework for collaborative planning rooted in the CANS, TCOM and the values ofyouth/family-centered practice will be revisited and its application within teaming will be discussed. Thepresentation will provide opportunities to explore the development of plan goals that address identifiedCANS items in a manner that is truly collaborative with youth and families.From this workshop, participants will be able to:Learning Goals: Describe the role of TCOM within a teaming process.Describe the steps in collaborative planning and the using needs and strengths to develop a plan.Articulate the process of using the CANS to monitor and adjust plans.Learning Objectives: Describe the consensus-building processArticulate the use of needs and strengths in developing plans for children, youth and families.Describe how to use CANS items to celebrate successes and support transitions.Workshop Schedule:9:00 – 9:30 AM 9:30 – 10:00 AM 10:00 – 10:30 AM 10:30 AM 10:45 – 11:50 AM 11:50 AM – 12:00 PM 1:00 – 1:30 PM Introduction and Welcome1:30 – 2:00 PM The Context: TCOM, Communimetrics and the Journey ThroughCare2:00 – 2:30 PM Teaming and TCOM2:30 PM Break2:45 – 3:50 PM The Steps to Planning from a TCOM Framework3:50 – 4:00 PM Wrap-UpThe John Praed Foundation 550 N Kingsbury, Suite 101, Chicago, IL 60654 e: afernando@chapinhall.org
ons, J.S. (2009). Communimetrics: A communication theory of measurement in human servicesettings. New York, NY: Springer.Lyons, J.S., & Weiner, D.A. (2009). (Eds.) Strategies in Behavioral Healthcare: Assessment, TreatmentPlanning, and Total Clinical Outcomes Management. New York, NY: Civic Research Institute.Meir, S. T. (2003). Bridging Case Conceptualization, Assessment, and Intervention. Thousand Oaks, CA:Sage Publishing.Lyons, J.S. (1999, 2017). Santa Clara County Child and Adolescent Needs and Strengths (Ages 5 ).Chicago, IL: John Praed Foundation.Presenter:April D. Fernando, PhD is a Policy Fellow and the TCOM Workforce Development Lead at Chapin Hall atthe University of Chicago. Dr. Fernando works with non-profit agencies as well as child welfare andbehavioral health care systems in implementing Transformational Collaborative Outcomes Management(TCOM) and utilizing the Child and Adolescent Needs and Strengths (CANS). She developed the CANSCommercially Sexually Exploited version, which is used nationally. A licensed clinical psychologist, Dr.Fernando brings her years of experience as an educator, clinician and mental health administrator to her workwith TCOM and the CANS.The John Praed Foundation 550 N Kingsbury, Suite 101, Chicago, IL 60654 e: afernando@chapinhall.org
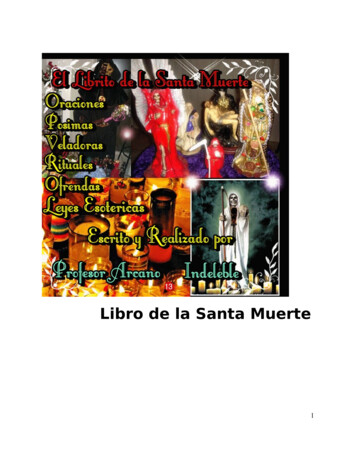
@praedfoundation/PraedFoundationChild and Adolescent Needs and Strengths(CANS) USER TIP SHEETThe C S is designed as a structured assessment strategy for identifying youth andfamily actionable needs and useful strengths. It provides a framework fordeveloping and communicating about a shared vision and uses youth and familyinformation to inform planning, supportBefore rating an item, considerdecisions, and monitor outcomes. Itthe following questions:provides a common language formultidisciplinary settings for consensusIs there any evidence of a need or strength?building.Are you understanding the youth’s behavior withinnormal development given her/his age?Have you considered the youth and family’s culture?Does your approach to assessment and engagementcommunicate respect for the youth and family’sculture?Is the need impacting the youth’s functioning?How urgently is action required on a need? Howuseful is the youth/family strength in achievingtargeted outcomes?Are you focused on describing the need or strength,and not the underlying cause?What services are already in place for the youthand/or family?Guiding Principles1. Items are included because they are relevant forplanning and decision making.2. Item ratings translate into action levels.3. Focus is on the youth’s needs, not interventions orservices that could mask a need.4. Consider culture and development before establishingaction levels.5. It’s about the ‘what,’ not the ‘why.’ Don’t explainaway needs with what you think might be anunderlying cause.Item Rating: Action Levels6. Specific ratings window (30-days) can be over riddenbased on action levels.The majority of the CANS items are rated in the context of what isnormative for the youth’s age and developmental stage.Rating Needs Domains0 No evidence of need; no need for action.Rating Strengths Domains0 Centerpiece strength; central to planning.1History of or possible need; watchful waiting/prevention/additional assessment.1Strength present; useful in planning.2Need is interfering with functioning; action orintervention required.2Identified strength; consider strength building ordevelopment activities.3Need is dangerous or disabling; immediate orintensive action required.3No strength identified; strength creation oridentification may be indicated.For more information on TCOM or CANS, contact support@TCOMTraining.com
(this page intentionally left blank)
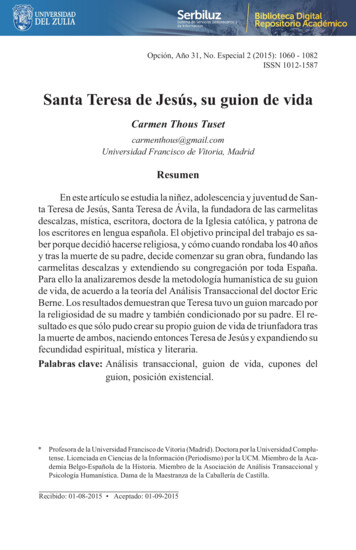
ASSESSING FOR NEEDSNORate this item a '0'.NO/NOT SUREYES@PraedFoundation/PraedFoundationRate this item a '3' ifimmediate action isneeded because it isinterfering withfunctioning at adisabling or dangerouslevel.Rate this item a '2' ifyou will take action.Rate this item a '1' for ahistory of need;watchful waiting, orprevention.Decision of whether or not information represents a NEEDIs thereevidence,suspicion, orhistory of a needin this area?YESIs there clearevidence thatthe need isinterfering withthe individual'sfunctioning?Will you takeaction?NOTE: It is important to develop consensus among all team members inidentifying the youth’s needs and in determining the item’s action level.Join the conversation at www.TCOMConversations.org
Is it astrength thatwill be used inplanning?MAYBEYESJoin the conversation at www.TCOMConversations.orgNOTE: It is important to develop consensus among all team members inidentifying the youth’s strengths and in determining the item’s action level.Is there evidenceof a STRENGTHin this area?Is the strengthuseful andsomething towork with, butthe youthcannot usetoday?NORate this item a '3' for noknown strength. Determineappropriateness foridentification orclassification.Rate this item a '0' if it isa powerful/centerpiecestrength.Rate this item a '1' if it isa useful strength andthere is opportunity tofurther develop.Rate this item a '2' for anidentified strength.Determine appropriatenessfor further development.Decision of whether or not information represents a STRENGTHASSESSING FOR STRENGTHS@PraedFoundation/PraedFoundation
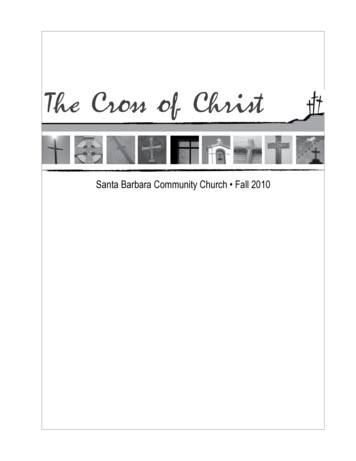
@PraedFoundationTCOMConversations.orgTraining Vignette:MikeMale, 15Mike is a 15 year-old boy who is currently living with his grandparents. He is not in contact with his motherwho has a serious substance dependence disorder. The identity of his father is not known. His last contactwith his mother was more than five years ago. Over the past three months, Mike has grown increasinglyargumentative and disruptive at home and school. He was suspended one day two weeks ago for fighting.This involved heated arguing and swearing at several other youth. In one fight, he was seen pushing the youthwith whom he was arguing. Teachers report that his grades have slipped considerably. He went from being aB/C student to mostly failing his courses this school year. Mike is not in special education – his IQ wasrecently tested to be 96.At home, his grandmother reports that he starts arguments with her, ignores curfew, and sometimes stays outwith friends until 2 or 3 in the morning. There is no evidence that he has engaged in any criminal behavior.Mike’s problems appear to have started after his grandfather had a stroke. His grandfather is better butexperienced partial paralysis that forced him to retire early. His grandmother works at an area grocery store.No other children or adults live in the house, although Mike’s aunt, who has five children, lives in theneighborhood. Mike is reportedly close to his cousins and spends a lot of time at their house. Mike hasexpressed interest in moving in with his aunt but she is unwilling to take on the added responsibility. Hisgrandparents currently feel like they are no longer able to handle Mike’s behavior and are asking about fostercare or residential treatment options. His grandparents report that they do not understand why Mike is soungrateful to them for taking him in. Mike expresses worries about his grandfather’s health and resentmentabout all the restrictions they have tried to place on this behavior.Mike has lived with his grandparents since he was an infant. At that time, child welfare had taken him fromhis mother due to allegations of neglect. She would leave him alone for long periods of time and failed toaddress his basic needs. As an infant, he was significantly underweight. He now is healthy and active. Hisgrandparents are not active in a church and neither they nor Mike have ever attended religious services.Mike reports that he has a girlfriend but has never been sexually active. Mike reports that they have beendating for about 8 weeks. He has a number of male friends at school. His friends have been supportive ofhim when he has had problems. At the assessment, Mike seemed to be a generally sullen and non-responsive.He was dressed in a baggy shirt and jeans, had his headphones on, and was listening music until the assessorasked him to turn it off. He answered questions but did not elaborate even when pressed. He reports nosuicidal or homicidal ideation. When the conversation turned to talking about Mike’s girlfriend, his moodbrightened notably and he smiled and talked openly.[2019]550 N Kingsbury, Suite 101, Chicago, IL 60654 www.PraedFoundation.org e: support@tcomtraining.org
(this page intentionally left blank)
@PraedFoundationTCOMConversations.orgPractice Vignette:EnzoMale, 15Enzo is a 15-year-old boy who is currently in foster care. Enzo is Latino, his mother is Puerto Rican and his father isDominican. Enzo and his two siblings were placed in care six years ago because their parents both were substanceabusers and involved in criminal activity; their parental rights were terminated two years later after they failed to complywith court-ordered drug treatment. Enzo’s older brother is 22 and is living independently; he visits with Enzo at leastonce each week. Enzo’s younger sister was adopted by a previous foster family and Enzo does not have any contactwith her.Until about one month ago, Enzo believed that his biological parents were dead. His older brother told Enzo and hissister this when parental rights were terminated, in an attempt to help the children heal and connect to their fosterparents. During a visit last month, however, Enzo’s brother told him that their parents are alive and that Enzo’s motheris sober and would like to have contact with Enzo. Enzo and his brother are close, and Enzo feels some pressure toresume contact with his mother because of his brother’s wish to reunite their family.Enzo currently lives with pre-adoptive foster parents, Karen and Daniel. He has lived with them since being dischargedfrom a residential treatment center two years ago. Prior to this foster home placement, Enzo was in several differentfoster homes, was admitted to inpatient psychiatric hospitals three times, and ultimately placed in a residential treatmentcenter for stabilization. Enzo’s placements were disrupted by – and his inpatient admissions precipitated by – severeoppositional behaviors, anger control issues, and incidents with foster parents and peers that included physical violence.He did well with his current foster family until recently, however, and was doing well in school, behaving at home, andhad expressed his interest in being adopted by Karen and Daniel, who have long hoped to adopt Enzo.Karen and Daniel both are first-generation Dominican Americans. They express that they care deeply for Enzo, andthat it means a lot to them to be able to adopt a boy who is Dominican. They maintain strong, mutually supportiveconnections with other members of the Dominican community and have tried to teach Enzo about the importance offamily in Dominican culture and about Dominican arts, cooking, and culture. Enzo has shown a great interest in theseissues and regularly attends Dominico-American Society events with them. Up until this month, Enzo reported to histherapist that he strongly identified with Dominican culture and that he was glad he was going to be adopted by aDominican-American family. About two weeks ago, Enzo became angry and postured aggressively toward a peer at oneof the events and Board members gave him a warning about his behavior.After he found out his mother was alive, Enzo began acting out. He has been staying out after school and coming homelate and after the town curfew, refusing to do his homework or chores, being argumentative, and saying that he does notwant to go to community events with his foster parents. On two occasions in the past two weeks, Enzo became soangry in response to being confronted about his homework that he threw his school books across the room. Last week,he told Karen and Daniel that he no longer wants them to adopt him and they should send him back to his mother.Karen and Daniel are very upset and somewhat stressed by Enzo’s statements; they have come to care deeply for Enzoand fear that his mother’s presence in his life will lead to them losing the boy. They are willing to do what it takes tohelp Enzo cope with his reactions but do not feel that he should have regular contact with his mother.Enzo is currently placed in a specialized classroom because of his history of oppositional behaviors and poor peerrelationships in school and a documented learning disability. Enzo was doing average work in this class, and behavingwell with intensive support, until he found out about his mother. This month, he has stopped doing his homework andhis classroom work, is failing all his tests and quizzes, and has been disruptive and disrespectful in class; his teachers areso frustrated with his behavior that they are not open to helping him. Last week, he got into a fight at school and wassuspended; he now says he wants to drop out of school.550 N Kingsbury, Suite 101, Chicago, IL 60654 www.PraedFoundation.org e: support@tcomtraining.com
@PraedFoundationTCOMConversations.orgEnzo has shown a long-term interest in hip hop music. Despite his current stressors, he continues to enjoy hip hop. Hesought out and attends an afterschool program at a local community center where professional musicians work withchildren and help them write and record their own songs. Enzo recently won first place in a competition for lyrics whenhe sang three of his own songs. Enzo continues to write and to rap at home, and says he thinks he may be able tobecome a famous rapper someday.[2018]550 N Kingsbury, Suite 101, Chicago, IL 60654 www.PraedFoundation.org e: support@tcomtraining.com
@PraedFoundationTCOMConversations.orgGuidelines for Planning with a Communimetric ToolOverviewThis guide is intended to provide information on implementing the TCOM framework to treatment planning. Theguide is also intended to support the development of an evidence-based, collaborative planning process with individuals(children, youth and/or adults) their families, and other stakeholders. For care providers in the Behavioral Health Caresystem, the information provides support in meeting Medicaid requirements to justify and ensure the effectiveness ofservices delivered.IntroductionPlanning for personal change is at the core of the Transformational Collaborative Outcomes Management (TCOM)approach. The purpose of TCOM is to facilitate understanding of the needs and strengths of the person or peopleserved and to bring to bear effective interventions that will help change lives. As a decision support approach, TCOMassists in the planning process—whether you call it a treatment plan, care plan, service plan, individual education plan,crisis plan, or plan of care—this plan is informed by relevant information about the person and/or family. A good planis by its very nature individualized. However, that individualization must function within the natural constraints ofprogram structures.The Child and Adolescent Needs and Strengths (CANS) is a tool that helps to operationalize the TCOM approach. TheCANS (as well as other Communimetric tools 1) includes items that reflect the information needed to be effective. Thiscore element, along with the basic structure of the action levels of a communimetric tool, is designed for the CANS toserve as the output of any assessment process to inform the creation of the plan that supports decisions to be maderegarding individuals and/or families.The TCOM Treatment Planning framework uses the CANS as a strategy to develop a collaborative and evidence-basedplan. By focusing on the What (CANS needs and strengths), the Why (shared understanding), the How (linking needand strengths to the shared understanding), the plan is developed with individuals and families, and managed as well asmonitored together to ensure that personal change is achieved.The WhatThe Summary of Needs and Strengths. The basic structure of the item ratings allow you to determine whether ornot to include an item in the plan. Following the completion of the TCOM collaborative assessment process, asummary of the CANS needs and strengths should be available for the care provider, individual and family to review.The summary of needs and strengths generated should list the items that could potentially be included in the plan: Forneeds, any item with a rating of ‘2’ or ‘3’ (referred to as ‘actionable’ needs) should be considered for attention. Anystrength with a rating of a ‘0’ or ‘1’ (referred to as ‘useful’ strengths) should be considered for strength-basedplanning. Strengths with ratings of ‘2’ or ‘3’ should be considered for strength-building activities.Other communimetric tools that are part of the TCOM Suite of Tools include: Adult Needs and Strengths Assessment (ANSA),Family Advocacy and Support Tool (FAST), Crisis Assessment Tool (CAT) or Childhood Severity of Psychiatric Illness tool (CSPI). Thereare also versions of the CANS and ANSA that were developed for specific service sectors and populations of youth and adults.1550 N Kingsbury, Suite 101, Chicago, IL 60654 www.PraedFoundation.org e: support@tcomtraining.com
@PraedFoundationTCOMConversations.orgThe WhyFor some needs there is a very clear relationship between what is actionable and what is recommended. For mostmental health needs, there are evidence-based and promising practices that should be considered when specificactionable needs are identified. For instance a rating of ‘2’ or ‘3’ on Depression would generally suggest that aevidenced-based treatment of depression would be optimal. A number of places provide links between these types ofactionable needs and either specific evidence-based practices or the core components model of evidence-informedpractice (e.g. Practicewise which is sometimes known as the Chorpita model).Risk behaviors also often suggest fairly specific considerations such as formal safety plans, etc. Thus an individualpresenting with a ‘2’ on Depression and a ‘3 ‘on Suicide might be effectively treated with Cognitive Behavior Therapyfor the depression and a specific safety plan for the suicidality.However, oftentimes a person will present with a number of actionable needs. In these circumstances it is necessary toorganize your understanding of the needs (and possibly strengths) to inform the target of treatment. Put bluntly, ifsomeone presents with 15 actionable needs, then it is rather unreasonable to assume you could create a treatment plansimultaneously and individually addressing each of these needs. That would be overwhelming not only to the providerbut also to the child/youth and family. Historically, we have attempted to simplify such situations using strategies suchas picking ‘a primary diagnosis’ or identifying the top three needs. These types of approaches invariably sacrifice anunderstanding of the complexity of a situation to achieve efficiency to the intervention. That is not likely a winningstrategy.One way to organize patterns of needs to inform a more focused treatment plan is to use the actionable needs to create acausal model to explain the individual’s current circumstances. It is often possible to fit together actionable needs into acausal explanation of the individual’s circumstances that guide treatment choice. For example, if a youth presented witha ‘3’ on Adjustment to Trauma, a ‘3’ on Anxiety and a ‘3’ on Self Injurious Behavior, it might be reasonable to proposethat the Trauma led to the Anxiety which led to the Self Injury as an attempt to self regulate the anxiety. Treatment thenwould be focused on the Adjustment to Trauma with the idea that successfully addressing these issues would reduceanxiety and the consequent cutting (or whatever the self injuring behavior might be).In this ‘puzzle’ strategy for using the CANS, it is sometimes useful to conceptualize actionable needs as either pathwayneeds, treatment target needs, or functional outcomes.Background needs (CORE Considerations) are needs that are likely not addressable but shift the pathwaydown which treatment is provided. An intellectual impairment or a significant trauma experience might be apathway need.Treatment target needs are those that would be the focus of intervention.Anticipated outcomes are needs that would be expected to respond as a result of effectively targeting thetreatment needs.For example, ADHD might be a treatment target while School Behavior and Achievement would be the FunctionalOutcomes. In other words, a young boy might have severe ADHD which results in both severe behavioral problems atschool and academic problems. Treating his ADHD as a Treatment Target would be anticipated to have a positiveeffect on both School Behavior and School Achievement.550 N Kingsbury, Suite 101, Chicago, IL 60654 www.PraedFoundation.org e: support@tcomtraining.com
@PraedFoundationTCOMConversations.orgHere is a different pattern of needs placed into this approach:Background NeedsSexual AbuseIntellectualTreatment Target NeedsAnxietyAdjustment to TraumaFunctional Outcome NeedsSchool AttendanceSocial FunctioningSelf injurious behaviorIn the above situation, the history of sexual abuse and low intellectual functioning set the stage for the treatmentapproach (trauma informed but consistent with the individual’s learning style), The treatment target needs are highlevels of Anxiety, problems with Adjustment to Trauma, Both of these needs would have treatment componentsdirectly addressing them. If treatment were successful one would then expect the reduction of needs involvingimproved School Attendance and Social Functioning, and reduced Self Injury.For Strengths, the approach is somewhat different. Strengths can be divided into two classes—strengths to use andstrengths to build. Strengths to use are those that might inform a strength-based approach. For instance, if you aregoing to use a child or youth’s involvement with a religious organization to help address social functioning issues thatwould be a strength to use. A strength to build are when the CANS recognizes that no strength exists (no evidence oridentified or 2 or 3) and the plan is to work with the child or youth to develop a strength in that area. For example, if ayouth has no identified talents or interests then a discovery process might be recommended to identify and develop anarea of interest.[2018]550 N Kingsbury, Suite 101, Chicago, IL 60654 www.PraedFoundation.org e: support@tcomtraining.com
(this page intentionally left blank)
Vignette NameAuthor NameItems NameBehavioral/Emotional NeedsMIKE (15 year‐old)Rating Rationale/JustificationPsychosis (Thought yOppositionalConductAnger ControlSubstance UseAdjustment to Trauma000220202no evidenceno evidenceSome argue sullen and non‐responsive; watchful waiting (1)Expresses worries about his grandfather's health; problems at home and school impacted by anxietyarguing at home; resentful of restrictions and ignores curfew at homeno evidencefighting at schoolno evidenceGF stroke; problems occurred following the stroke; expressed worries about thisLife Domain FunctioningFamily Functioning2 Arguing with grandparents; resentment about restrictions on his behaviorGrandparents feel like they are no longer able to handle Mike's behavior and are looking into foster care or residential2 treatment options2 Fighting with peers at school resulting in suspension; has friends and girlfriend0 no evidence1 fighting with peers; breaking curfew at home ‐‐indirect2 Fighting with peers; suspension3 failing grades0 no evidence0 no evidence0 no evidence1 indirectLiving SituationSocial FunctioningDevelopmental/IntellectualDecision MakingSchool BehaviorSchool AchievementSchool AttendanceMedical/PhysicalSexual DevelopmentSleepRisk BehaviorsSuicide RiskNon-Suicidal Self-Injurious BehaviorOther Self-Harm (Recklessness)Danger to OthersSexual AggressionDelinquent BehaviorRunawayIntentional Misbehavior00010100no evidenceno evidenceno evidencefightingno evidencecurfew violationsno evidenceno evidenceCultural FactorsLanguageTraditions and RitualsCultural Stress0 no evidence0 no evidence0 no evidenceStrengths DomainFamily StrengthsInterpersonalEducational SettingTalents and InterestsSpiritual/ReligiousCultural IdentityCommunity LifeNatural SupportsResiliency112333112Grandparents; aunt and cousinsAble to maintain frienships; romantic relationshipSchool is not adequately addressing Mike's problems.no evidenceno evidence; not a part of the family's cultureno evidencesees aunt and cousins in the neighborhoodfriends at school; girlfriendHas friends, girlfriend, family as supports. Not accessing them at this time.2221020000Mike stays out until 2 or 3am; not able to provide adequate supervisionGPs not that involved in his treatment; beginning to look into having him leave their careMike as ungrateful as the reason for his behaviorSome family resources, but aunt seems reluctant to helpno evidencegrandfather's stroke and resulting paralysisno evidenceno evidenceno evidenceno evidenceCaregiver Resources and NeedsSupervisionInvolvement with CareKnowledgeSocial ResourcesResidential StabilityMedical/PhysicalMental HealthSubstance UseDevelopmentalSafetyPotentially Traumatic/Adv Chldhd ExpersSexual AbusePhysical AbuseEmotional AbuseNeglectMedical TraumaWitness to Family ViolenceWitness to Community/School ViolenceNatural or Manmade DisasterWar/Terrorism AffectedDisruptions in Caregiving/Attachment LossesParental Criminial BehaviorsNoNoNoYesNoNoNoNoNoYesNono evidenceno evidenceno evidenceMom would leave him alone for long periods of time and failed to address his basic needs.no evidenceno evidenceno evidenceno evidenceno evidenceChild welfare had taken him from his mother due to allegations of neglect.no evidence
(this page intentionally left blank)
Vignette Name:Date:Relevant Item GridTrainer:Strengths to BuildTreatment Planning Worksheet -- SAMPLEMIKE (15 year-old)Useful StrengthsTalents and Interests (3)Educational Setting (2)Resiliency (2)Strengths to Build (2’s and 3’s) from Strength Domain for child/youthFamily Strengths (1)Interpersonal (1)Natural Supports (1)CG Social Resources (0)Target Needs – Caregiver(s)Strengths to Use (0’s and 1’s) from Strength Domain for child/youth from the Caregiver Needs and Strengths Domain that constitutestrengths for Caregiver(s)Target Needs – Child/Youth2’s and 3’s fromCaregiver Resources and Needs domainCG Supervision(2)CG Knowledge (2)CG Involvement with Care (2)CG Medical/Physical (2)2’s and 3’s from all Child Domains: Behavioral/Emotional Needs, LifeFunctioning, Risk Behaviors, Cultural Factors, Potentially Traum
Mike is a 15 year-old boy who is currently living with his grandparents. He is not in contact with his mother who has a serious substance dependence disorder. The identity of his father is not known. His last contact with his mother was more than five years ago