Transcription
Big Data& Healthcare
AcknowledgmentsThe Mass Technology Leadership Council is grateful for the leadership and support that Governor DevalPatrick has provided to the region’s big data ecosystem with his initiative. We look forward to working withthe Administration, the Massachusetts eHealth Institute at the Massachusetts Technology Collaborative, andthe Massachusetts Life Sciences Center, along with industry representatives and other government agenciesto implement the key recommendations made in this report.The MassTLC Big Data Community’s initiatives, including this report, would not be possible without thecommitment and engagement of many talented leaders and volunteers in the Mass Technology LeadershipCouncil’s Big Data Cluster. Cluster community leaders include Co-Chairs: Leo Hermacinski, CEO, dSideTechnologies; Marilyn Matz, Co-Founder and CEO, Paradigm4; and Bob Zurek, Senior Vice President ofProduct, Epsilon.We would also like to acknowledge the people responsible for the overall strategy and thought processbehind this big data and healthcare initiative: Richard Dale, COO, Optum Labs; Dmitri Gunn, MIT MediaLab; Pamela Goldberg, CEO, Massachusetts Technology Collaborative; Leo Hermacinski, CEO, dSideTechnologies; Patrick Larkin, Director, the Innovation Institute at the Massachusetts Technology Collaborative;Marilyn Matz, Co-Founder and CEO, Paradigm4; Steven O’Leary, Managing Director, Aeris Partners; DavidPower, President, Power Strategy; Laurance Stuntz, Director, Massachusetts eHealth Institute; SusanWindham Bannister, Ph.D., President and CEO, the Massachusetts Life Sciences Center, and to JaniceMcCallum, Managing Director, Health Content Advisors for her work in writing this report.Thank you to Optum Labs for hosting the big data and healthcare roundtable at their Cambridgeoffice. This report was funded by a grant from the Massachusetts eHealth Institute at the MassachusettsTechnology Collaborative.About the Mass TechnologyLeadership CouncilWith more than 550 member companies, the Mass Technology Leadership Council (MassTLC) is theregion’s leading technology association and the premier network for tech executives, entrepreneurs, investorsand policy leaders. MassTLC’s mission is to accelerate innovation by connecting people from across thetechnology landscape, providing access to industry-leading content and ideas, and offering a platform formember companies to collectively advance their interests. For more information on MassTLCvisit www.masstlc.org1
Table of Contents03PREFACE04Executive Summary06Introduction07TRANSFORMING HEALTHCAREDrivers of Change: Federal and State ProgramsDrivers of Change: Growing Sources of DataChallenge: Connecting Fragmented DataTechnical LimitationsCultural Barriers to AccessPatient Engagement11USING BIG DATA TO IMPROVE HEALTHCARE DELIVERYStrengthen the Evidence BasePersonalize MedicineReduce Costs14SOME EARLY DATA-DRIVEN EXPERIMENTS IN HEALTHCARECareMoreZeoathenahealth/KyruusAmbulatory Practice of the Future1719SUMMARYCONCLUSION & NEXT STEPS2
PrefaceThis big data and healthcare report is part of theMass Technology Leadership Council’s (MassTLC)technology leadership to explore some of the mostwork with the Mass Technology Collaborative’svexing challenges and opportunities of our times.eHealth Institute in support of MassachusettsGovernor Deval Patrick’s ongoing initiatives toidentify and exploit key economic and leadershipopportunities for the Commonwealth.We engaged in this initiative to foster greaterOur Delphi process involved four steps: (1)interview thought leaders representing both bigdata and each of the target industries, (2) surveyparticipants to identify areas of consensus as wellas differences of opinion, (3) provide survey findingscollaboration between sectors; to spotlight andback to the Delphi participants, and (4) explore theenhance the leadership capacity of Massachusetts;opportunities, barriers, and possible public/privateto attract talent, investment, and new business;interventions through an interactive roundtable.and to position our region at the forefront of theOn November 19, 2013, MassTLC, with theBig Data revolution. We have employed a Delphimethodology to gather the leading minds within keyindustries to lend their expertise to help identify bothshort- and long-term opportunities.Our work builds upon our 2012 report, Big Datasupport of the Massachusetts eHealth Institute(MeHI) at MassTech Collaborative, convened aroundtable of big data and healthcare thoughtleaders from industry, academia, and governmentto identify and explore transformative healthcareand Analytics: A Major Market Opportunity forinitiatives that have already overcome data accessMassachusetts, and subsequent big data Delphiconstraints and are primed to leverage innovativeroundtable report, finding, among other themes, thatdata science tools and models.leadership opportunities exist for Massachusettsin capitalizing on its strengths and focusing onactionable business insights.With this, we set out in 2013 to “bump” and3We leveraged our four-decade legacy of data andWe believe the reader will find it instructive toread both the healthcare and life sciences reportstogether as there is increasing convergencebetween data sources produced and used in theseconnect the region’s big data thought leadersindustries and both reports touch on commonwith those in other key strength areas, includingthemes of data quality, metadata, and accesshealthcare, life sciences, and urban infrastructure.to data.
Executive SummaryMassachusetts plays a leading role in advancingbe the enemy of the good, it only gets better byhealthcare reform for the nation and has uniqueexposing it, by having people use it and play aroundresources to build upon in advancing new data-with it.”driven methods to improve healthcare delivery.While we acknowledge the many challenges thatAs digital technology matures in healthcare, theremain, we directed our focus on the data sciencelandscape is quickly changing from an environmentopportunities that are emerging as new sources ofof data scarcity to one of data abundance.data are made more readily available.Naomi Fried: “I think we all agree that big datais going to be transformative in healthcare. TheFollowing some background on the drivers ofchange in healthcare analytics, we review how bigfirst step obviously is to have the data,and I think we’ve made good progress.We’ve digitized a lot of information. Wedata is already leading to fundamentalI think we allagree thathave medical records going in acrossbig data isthe country. The next piece is aroundliquidity, getting it out. I think progress isbeing made there.”Where can big data methods bebest applied to accelerate progress intransforming healthcare delivery? That’sgoing to betransformativein healthcare.improvements in delivering better—andmore personalized — healthcaremore efficiently.A common thread amongst ourthought leaders was related to movingbeyond just funding a series of pilotstudies; but to find a way to establish acontinuously updated learning system.It’s a lofty goal to connect all of thethe essential question we posed to the thoughtdisparate and diverse data relevant to healthcare,leaders that we convened for our big data andespecially when the sources of data are growing athealthcare Delphi initiative.a fast pace. However, rather than trying to “boil theEven with the forward-thinking innovators weassembled, it was difficult to overlook the ongoingchallenges related to gaining access to, andintegrating, disparate data sets, so we devote asection to the technical, cultural, and administrativechallenges that still exist.While many questions were raised aboutmaintaining trust in the quality of the datasets thatare growing in number and size, the assembled dataexperts agreed that the best method for gainingunderstanding of the data is making itmore accessible.Micky Tripathi: “In industry after industry whatwe’ve seen is that it only gets better by using thedata. So to the point about not letting the perfectocean” (a term that came up more than a coupleof times), we chose to carve out an area wherea substantial amount of data is already availableand some baseline assumptions and queries havealready been established, so that we can moveforward on innovating with big data technologies.We present examples of early experiments indata-driven healthcare, based in Massachusetts,along with CareMore, a Wellpoint program. Theseinnovative companies, including athenahealth/Kyruus, Massachusetts General Hospital’sAmbulatory Practice of the Future, and Zeo, offerinsights into how to leverage multiple data sourcesin a collaborative environment to effect positivechange in healthcare delivery.4
Micky TripathiMA eHealthCollaborativeTomHopcroftMassTLCVicky Mahn-DiNicolaXeroxJeff LevinScherzHSPH/HMSDavidJudge*MGHLaurance StuntzMA eHealth InstitutePaul WallaceOptum LabsCharlie SchickIBMJulie YooKyruusRobert NagleInterSystemsMarilyn MatzParadigm4Paul BleicherOptum LabsMara BloomMGHThe Delphi PanelDavid IckeMC10Joseph HendricksonathenahealthChristopher BoutonEntagenThomas HawkinsBlue Cross Blue ShieldDenny BrennanMA Health DataConsortiumRichard DaleOptum LabsDmitri GunnMIT Media LabDave DickinsonOptum LabsNaomi FriedChildren’s Hospital* denotes that individual is no longer with the organization cited at print time.See Appendix A for Panel Member bios.5Markus FromherzXeroxClifford GoldsmithMicrosoft
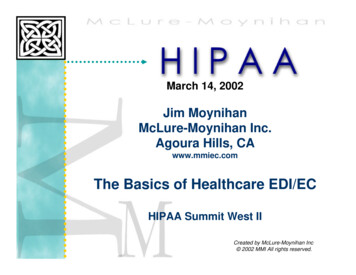
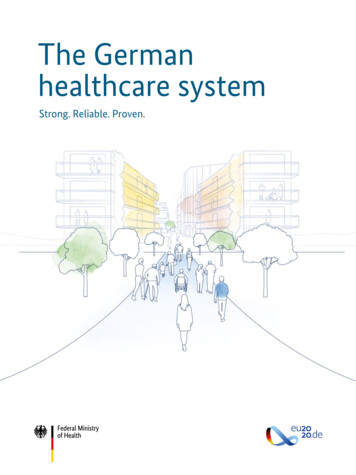
IntroductionCharlie Schick: “The future of healthcaretransformation is going to be data driven.”This report focuses on areas where big datanot only the healthcare providers, but they havebecome the risk managers for the patients.”Secretary Bialecki’s statement helps frame theinvestments are likely to accelerate progresscontents of this report to focus on areas where bigtoward the concurrent goals of 1) providing betterdata can support new models of healthcare delivery.care experiences for patients; 2) improving thehealth of the population served; and 3) loweringper capita costs. These three goals are referred toas the Triple Aim. This Triple Aim1 paradigm (seeFigure 1), which has its origins at the Institute forHealthcare Improvement (IHI) in Cambridge, MA,Figure 1: IHI Triple Aimwas referenced frequently and served as a usefulmodel throughout the discussion.Paul Wallace: “So I think we need to changeour language and recognize that the message ofthe Triple Aim is that you’ve got to do them all atthe same time, which means you really have toreallocate effort. We have to allocate a lot of effort atreconciling the ambiguities around trying to do all ofthose simultaneously, rather than thinking, just pullone lever and have it work out.”PopulationExperienceHealthof CarePer Capita CostThe challenges involved in delivering qualityhealthcare at affordable costs are complex and can’tbe solved in isolation. We need to explore ways toleverage big data science to develop new methodsfor measuring and analyzing outcomes, and to alignthe outcomes analysis with the experience of careand cost objectives.Greg Bialecki: “From the state’s point of view,I think we’d really be interested in focusing on thehealthcare delivery system. I think our biggestinterest is for the practitioners in the healthcaredelivery system and I include the payers inthat. What kind of information do they need inaccountable care2? We’ve got this huge shift andwe’re saying that the healthcare providers now are1 ges/MeasuresResults.aspx Accessed 3/18/14.2 Accountable Care Organization (ACO) definition from CMS: ce-Payment/ACO/.Accessed April 1, 2014.6
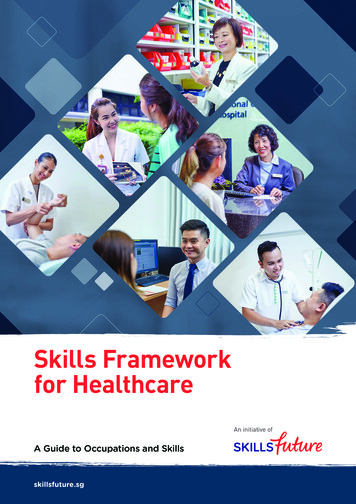
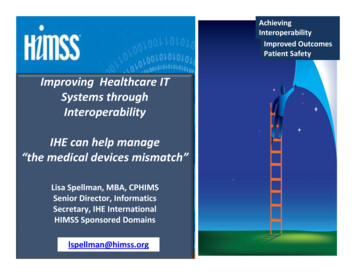
Transforming HealthcareImproving quality in the healthcare delivery systemthe federal Electronic Prescribing and Meaningfulhas been a major objective for policy makers andUse Incentive Programs, which started in 2009 andpractitioners alike. However, early initiatives werecontinue today, the launch of the statewide healthhampered by the lack of reliable data to use forinformation exchange, the Mass HIway, in 2012,measuring quality and outcomes. Consequently,and Massachusetts’ further investment of over 200programs, such as the Consumer Assessment ofmillion in healthcare transformation through theHealthcare Providers and Systems (CAHPS)3, relied2012 Health Reform update, Chapter 224.on survey data to measure and benchmark qualityand performance improvement from theAdoption of electronic health record (EHR)technology has grown rapidly under the Stimulus/patient’s perspective.HITECH Act and the Meaningful Use program withMore recent quality initiatives, such as programsvirtually all acute hospitals in the Commonwealthto reduce hospital-acquired conditions, havenow using EHRs5 and more than 80% of physiciansbenefited from a knowledge base constructed inusing EHRs6. Figure 2 below illustrates the threepart from data that have been reported as part ofstages of Meaningful Use and the associated goalsfederal and state programs.of each stage. Currently, most eligible providers are4working towards Stage 2 of Meaningful Use.Drivers of Change: Federaland State ProgramsMeaningful Use and ePrescribing programsare part of a longstanding shift to value-basedpurchasing (VBP) initiated by the Centers forA series of policy initiatives at the state andfederal level have provided incentives for healthcareproviders to adopt digital infrastructure with theMedicare and Medicaid Services (CMS) nearlyten years ago. CMS understood that an effectiveVBP system required a strong foundation of dataaim of improving the efficiency of healthcaretransactions. Examples include the establishmentof the Massachusetts eHealth Institute in 2008,reporting and sharing upon which new clinicalpractices could be built, and ultimately, outcomescould be measured and compared.Figure 2: Meaningful Use StagesData capturing &sharingStage 1Improved outcomesAdvanced clinicalprocessesStage 2
Our Delphi process involved four steps: (1) interview thought leaders representing both big data and each of the target industries, (2) survey participants to identify areas of consensus as well as differences of opinion, (3) provide survey findings back to the Delphi participants, and (4) explore the opportunities, barriers, and possible public/private interventions through an interactive .