Transcription
Information & Assistance Unit guide 11How to file a petition to reopenIf your disability has gotten worse after a workers’ compensation judge has issued anaward, this form can be used to reopen your case.You should get a medical report from your doctor saying your condition hasworsened, and collect any other facts that support your case.Complete the form, following the attached sample. Be sure to sign and date the form.You have five years from the date of injury to file this petition.If the insurance company won’t voluntarily reopen your case and you are ready for ahearing, fill out a declaration of readiness to proceed (see I&A guide 5) and submit itwith your petition.Send the original to your local WCAB office and copies to all the parties.Submit the following documents with your form filing in the order shown: Document Cover SheetDocument Separator Sheet (for Petition for Reopen)Petition for ReopenVerificationDocument Separator Sheet (for Proof of Service By Mail)Proof of Service By MailKeep copies of your filings for your records.All documents filed with the WCAB must include a document cover sheet anddocument separator sheet. Please see I&A guides 17 and 18 to learn how tocomplete these forms. In addition all forms must be typed or handwritten in blockletters to insure legibility. Additional form instructions can be found on the EAMSOCR handbook athttp://www.dir.ca.gov/dwc/eams/SampleFiles/EAMS OCR%20handbook.pdf.If you need help, call an Information and Assistance (I&A) office, or attend aworkshop for injured workers. The local I&A phone numbers are attached to thisguide. You can get information on a local workshop from the I&A office or on the Webat www.dwc.ca.gov.I&A 11Rev. 06/18
Information & Assistance Unit guide 11If you do not have the name and address of your insurance company to completea form, please link to mins.asp.The information contained in this guide is general in nature and is not intended as a substitute for legaladvice. Changes in the law or the specific facts of your case may result in legal interpretationsdifferent than those present here.When sending documents to a district office, please make sure they are not folded or stapled. Sendthem in a large manila envelope. Please see the EAMS OCR forms handbook for further instructions.I&A 11Rev. 06/18
WORKERS’ COMPENSATION APPEALS BOARD DISTRICT OFFICESANAHEIM, 92806-21311065 North Link, Suite 170Information & Assistance Unit (714) 414-1801SACRAMENTO, 95834-2962160 Promenade Circle, Suite 300Information & Assistance Unit (916) 928-3158BAKERSFIELD, 93301-1929th1800 30 Street, Suite 100Information & Assistance Unit (661) 395-2514SALINAS, 93906-22041880 N Main Street, Suites 100 & 200Information & Assistance (831) 443-3058EUREKA, 95501-0529 * Virtual office *Information & Assistance Unit(707) 441-5723SAN BERNARDINO, 92401-1411464 W Fourth Street, Suite 239Information & Assistance Unit (909) 383-4522FRESNO, 93721-22192550 Mariposa Street, Suite 4078Information & Assistance Unit (559) 445-5355SAN DIEGO, 92108-44247575 Metropolitan Drive, Suite 202Information & Assistance Unit (619) 767-2082LONG BEACH, 90810-18701500 Hughes Way, Suite C203Information & Assistance Unit (424) 450-2565SAN FRANCISCO, 94102-7014nd455 Golden Gate Avenue, 2 FloorInformation & Assistance Unit (415) 703-5020LOS ANGELES, 90013-1105thth320 W 4 Street, 9 FloorInformation & Assistance Unit (213) 576-7389SAN JOSE, 95113-1402100 Paseo de San Antonio, Suite 241Information & Assistance Unit (408) 277-1292MARINA DEL REY, 90292-6902ndrd4720 Lincoln Boulevard, 2 and 3 FloorsInformation & Assistance Unit (310) 482-3820SAN LUIS OBISPO, 93401-87364740 Allene Way, Suite 100Information & Assistance Unit (805) 596-4159OAKLAND, 94612-1499th1515 Clay Street, 6 FloorInformation & Assistance Unit (510) 622-2861SANTA ANA, 92707-77042 MacArthur Place, Suite 600Information & Assistance Unit (714) 942-7576OXNARD, 93030-79121901 N Rice Avenue, Suite 100Information & Assistance Unit (805) 485-3528SANTA BARBARA, 93101-7538 * Satellite office *130 E Ortega StreetInformation & Assistance Unit (805) 568-1390POMONA, 91768-1653732 Corporate Center DriveInformation & Assistance Unit (909) 623-8568SANTA ROSA, 95404-477150 “D” Street, Suite 420Information & Assistance Unit (707) 576-2452REDDING, 96002-0940nd250 Hemsted Drive, 2 Floor, Suite BInformation & Assistance Unit (530) 225-2047STOCKTON, 95202-231431 E Channel Street, Suite 344Information & Assistance Unit (209) 948-7980RIVERSIDE, 92501-33373737 Main Street, Suite 300Information & Assistance Unit (951) 782-4347VAN NUYS, 91401-33706150 Van Nuys Boulevard, Suite 105Information & Assistance Unit (818) 901-5374Rev. 07/21
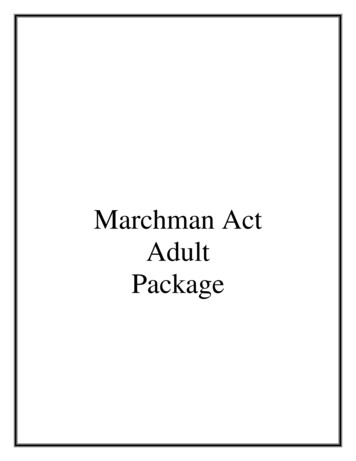
STATE OF CALIFORNIADWC DISTRICT OFFICESAMPLEDOCUMENT COVER SHEETIs this a new case?YesDMore than 15 Companion CasesNoDCompanion Cases ExistDWalkthroughDTODAY'S DATEDate:(MM/DD/YYYY)EAMS CASE NUMBERCase Number 1SSN:DSpecific InjuryDCumulative InjuryDNoDYOUR SOCIALSECURITY NUMBERDATE OF INJURY(End Date: MM/DD/YYYY)(Start Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)IF NEW CASELEAVE BLANKBody Part 1:USE CODE FROMBODY PART CODE LIST -Body Part 3:SEE PAGE 8Body Part 2:Body Part 4:Other Body Parts:Yes WHEN MORE THAN 5 BODY PARTS USE BODYPART NUMBER 700 IN THIS FIELDPlease check unit to be filed on ( check only one box )DADJCompanion CasesCase Number 2IDDEUDSIFDUEFDSpecific InjuryDCumulative InjuryDDINTSAU(Start Date: MM/DD/YYYY)Body Part 3:Body Part 2:Body Part 4:DWC-CA form 10232.1 Rev. 5/2020- Page 1 of 8(End Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)Body Part 1:Other Body Parts:0RSU
District office codes for place of venueLegend ta AnaBakersfieldEureka*FresnoLos AngelesLong BeachMarina del linasSanta Barbara**San BernardinoSan DiegoSan FranciscoSan JoseSan Luis ObispoSanta RosaStocktonVan Nuys* Eureka is a satellite office of Santa Rosa district office.** Santa Barbara is a satellite office of Oxnard district office.Use this document to complete forms,but do not file this document with your forms.DWC‐CA form 10232.1 Rev. 5/2020 – Page 7 of 8
BODY PART CODES 0410411420430440450498DescriptionHead - not specifiedBrainEar - not specifiedEar - externalEar - internal including hearingEye - including optic nerves and visionFace - not specifiedJaw - including chin and mandibleMouth - including lips, tongue, throat and tasteTeethNose - including nasal passages, sinus and smellFace - multiple parts any combination of above partsFace - forehead, cheeks, eyelidsScalpSkullHead - multiple injury any combination of above partsNeckUpper extremities - not specifiedArm - above wrist not specifiedArm - upper arm humerusArm - elbow head of radiusArm - forearm radius and ulnaArm - multiple parts any combination of above partsArm - not specifiedWristHand - not wrist or fingersFingersUpper extremities - multiple parts any combination ofabove partsTrunk - not specifiedAbdomen - including internal organs and groinHerniaBack - including back muscles, spine and spinal cordChest - including ribs, breast bone and internal organs ofthe chestHips - including pelvis, pelvic organs, tailbone, coccyx andbuttocksShoulders - scapula and clavicleTrunk - use for side; multiple parts any combination ofabove parts
onLower extremities - not specifiedLegs - above ankles, not specifiedThigh femurKnee PatellaLower leg tibia and fibulaLeg - multiple parts any combination of above partsLeg - not specifiedAnkle malleolusFoot not ankle or toeToesLower extremities - multiple parts any combination of abovepartsMultiple parts more than five major parts use only in fifthposition of listing of body partsBody system - not specificCirculatory system - heart - other than heart attack, blood,arteries, veins, etc.Circulatory system - Heart attackDigestive system - stomachExcretory system - kidneys, bladder, intestines, etc.Musculo-skeletal system - bones, joints, tendons, muscles,etc.Nervous system - not specifiedNervous system - StressNervous system - Psychiatric/psychRespiratory system - lungs, trachea, etc.Skin dermatitis, etc.Reproductive systemsOther body systemsCOVID-19Unclassified - insufficient information to identify body parts
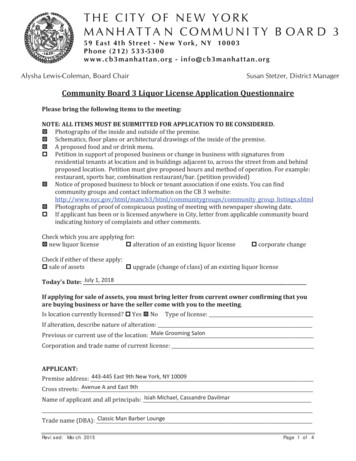
SAMPLEDOCUMENT SEPARATOR SHEETProduct Delivery UnitADJDocument TypeLEGAL DOCSDocument TitlePETITION TO REOPENDocument DateAuthorDATE YOU FILLED OUT THE FORMMM/DD/YYYYYOUR NAMEOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2017 Page 1MM/DD/YYYY
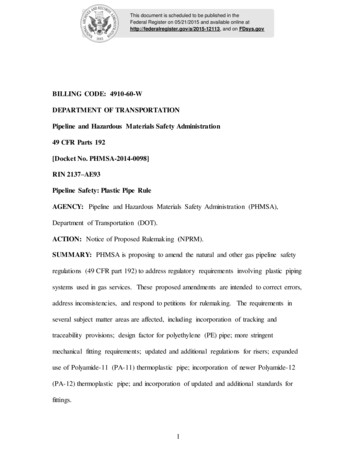
SampleSAMPLEDepartment of Industrial RelationsDivision of Workers' CompensationWORKERS' COMPENSATION APPEALS BOARDSTATE OF CALIFORNIAYOURNAMEYour Namevs.YOUR EMPLOYER ANDYour employer and insurance companyINSURANCE COMPANY)))Applicant, ))))))Defendants )Case No.EAMS/WCAByourWCAB case numberPETITION TO REOPENPetitioner hereby requests that the above-entitled action be reopened for the following reasons:EXPLAIN IN YOUR WORDS WHY YOU FEEL YOUR CASE SHOULD BE REOPENEDExplain in your words why you feel your case should be reopenedDWC/WCAB FORM 42 (REV. 8-85)
SampleVERIFICATIONSTATE OF CALIFORNIAyour countyCounty ofyour nameI, the undersigned, say that I am , a party tothis action. I have read the foregoing Petition to Reopen and know the contents thereof, andthat the same is true of my own knowledge, except as to the maters which are therein statedupon my information or belief, and as to those matters that I believe to be true.I declare under penalty of perjury that the foregoing is true and correct.date mailedyour cityExecuted on at , California.your signaturePetitionerApril 2014
SAMPLEDOCUMENT SEPARATOR SHEETProduct Delivery UnitADJDocument TypeLEGAL DOCSDocument TitlePROOF OF SERVICEDocument DateAuthorDATE YOU FILLED OUT THE FORMMM/DD/YYYYYOUR NAMEOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2017 Page 1MM/DD/YYYY
Proof of Service by MailSAMPLEI declare that:YOUR COUNTYI am (resident of / employed in) the county of ,California.I am over the age of eighteen years, my (business / residence) address is:PUT YOUR HOME ADDRESS HERENAME OF DOCUMENTTODAY'S DATE I served the attachedOn ,on the parties listed below in said case, by placing a true copy thereof enclosed ina sealed envelope with postage thereon fully paid, in the United State mail atCITY WHERE YOU MAILED THISaddressed as follows:1) WORKERS' COMPENSATION APPEALS BOARD: ADDRESS2) INSURANCE COMPANY: NAME, ADDRESS AND CLAIM NUMBER3) DEFENSE ATTORNEY (IF KNOWN): NAME AND ADDRESS4) ALL OTHER PARTIES INVOLVED IN YOUR CASE: NAME AND ADDRESSI declare under penalty of perjury under the laws of the State of California that theforegoing is true and correct, and that this declaration was executed onTODAY'S DATE at ,CITY(date) ,California.PRINT YOUR NAMEType or print nameSIGN YOUR NAMESignature
WORKERS' COMPENSATION APPEALS BOARD DISTRICT OFFICES ANAHEIM, 92806-2131 1065 North Link, Suite 170 Information & Assistance Unit (714) 414-1801 SACRAMENTO, 95834-2962 . VAN NUYS, 91401-3370 . 6150 Van Nuys Boulevard, Suite 105 Information & Assistance Unit (818) 901-5374 . Rev. 07/21.