Transcription
Department of Otolaryngology—Head and Neck SurgeryBest Practice Protocols for Headand Neck Cancer PatientsHow can SLPs best help this population?October 16, 2020Brian PetersonErin LoganSpeech Pathologist IISpeech Pathologist IIUniversity of Iowa Hospitals and ClinicsUniversity of Iowa Hospitals and ClinicsCHANGING MEDICINE.CHANGING LIVES.
Disclosures University of Iowa Hospitals and Clinics–We are staff employees and receive salaries–No personal, professional or financial matters to discloseDepartment of Otolaryngology—Head and Neck Surgery
Course Objectives Learners will:–Explore sample treatment plan for individuals pre, mid, and postradiation /- chemotherapy for HNC–Gain knowledge on evidenced based exercises for individuals receivingtreatment for HNC–Gain information about radiation toxicities (side effects) and what canbe done to manage them–Discuss SLP's role in PEG weaning and chronic dysphagia–Create sample therapy plans and recommendations in real patientcase studiesDepartment of Otolaryngology—Head and Neck Surgery
What makes this population unique? Changing face of HNC Smoking and alcohol remain risky (Dal Maso et al, 2016) HPV now thought to cause 70% of HNC cases! (CDC, 2020) HPV16 remains most common strain (Marur et al, 2010) Silver lining?–HPV cancers respond better to treatment–61% lower risk of death, 62% lower risk of progression (Fakhry etal, 2008)Department of Otolaryngology—Head and Neck Surgery
The UIHC Treatment ApproachInitial EvaluationWeekly or Bi-WeeklyTherapy DuringTreatment4-7 sessionsPost-treatmentTherapyDepartment of Otolaryngology—Head and Neck Surgery
The UIHC Treatment Approach - Evaluation Initial Evaluation– Clinical bedside or instrumental evaluation Which one? Review chart and consider factors like staging, radiation plan, otherhealth history– Education! Provide packet with written version of information presentedSLP's role throughout treatment process (Senchak et al, 2019)Strategies to maximize safety and efficiency of swallowManagement of side effects (radiation toxicities)– Complete EAT10– Initial instruction of prophylactic oropharyngeal exercise program– Provide list of food options for individuals experiencing radiation toxicitiesDepartment of Otolaryngology—Head and Neck Surgery
The UIHC Treatment ApproachInitial EvaluationWeekly or Bi-WeeklyTherapy DuringTreatment4-7 sessionsPost-treatmentTherapyDepartment of Otolaryngology—Head and Neck Surgery
The UIHC Treatment Approach – Therapy DuringTreatment Weekly/Bi-weekly visits during Radiation /- Chemotherapy–Typically meet 5-7 times during treatment for 20-30 minutes–Encourage patients to KEEP SWALLOWING!–Focus on three topics:– Monitor current PO/swallow status, offering suggestions to maximize nutritionand safety– Assess and provide behavioral management recommendations for radiationtoxicities– Reinforce swallowing exercise program completion/adherenceDepartment of Otolaryngology—Head and Neck Surgery
ProphylacticExercises forHNC PatientsDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Swallowing exercise program targets areas of impairmentand/or areas most likely to be affected in RT treatment plan Number of exercises/maneuvers and/or frequency ofexercises/maneuvers recommended may change as patientsprogress through treatment course Focus may shift from eating AND exercise to eating ASexerciseDepartment of Otolaryngology—Head and Neck Surgery
Yeah, but why?! Less PO intake less resistive load on swallow musculature,proactive swallow therapy aims to maximize use of swallowmusculature during RT or CRT (Hutcheson, 2013) Targeting swallowing habilitation vs rehabilitationDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Lingual ROM /- resistance Jaw opening Pharyngeal strengthening Tongue base Laryngeal elevation Laryngeal vestibule closure UES openingDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Lingual Exercises–Lingual ROM Out, back, up, down, left, right, trace around teeth/gums–Lingual ROM against resistance Extend tongue out against tongue depressor/back of spoon Place tongue depressor/back of spoon at labial corner, extendtongue and press against tongue depressor/back of spoon Put fingers on cheek, press tongue inside cheek against fingersDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Jaw Opening Exercises- ( 35 mm or 3 stacked fingers normal)–Jaw opening Open mouth as wide as possible to a point of stretch, butnot pain Manual assistance to maximize opening Stacked tongue depressors TherabiteDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Jaw Opening Exercises- ( 35 mm or 3 stacked fingers normal)–Jaw opening Open mouth as wide as possible to a point of stretch, butnot pain Manual assistance to maximize opening Stacked tongue depressors Therabite– Jaw side-to-side movement– Circular jaw movement ("exaggerated fake chew")Department of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Pharyngeal Strengthening Exercises–Masako "Tongue Hold" Exercise Extend tongue tip out and hold between teeth, gums, or with gauze/paper towel Swallow as many times as possible with tongue extended until you "hit a wall" Tongue Base Exercises–Tongue pull back Leave tongue tip on FOM and pull tongue back as if trying to touch your spine–Gargle–Yawn–Effortful swallowDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Hyolaryngeal Elevation Exercises Mendelsohn Maneuver Place finger on Adam's Apple, feel elevation and descentduring a normal swallow Next, try to hold elevation at its highest point using throatmuscles for 3-5 seconds Finish the swallow–Falsetto Glide on "eee" from low to highest pitch and hold for 2-3secondsDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers UES Opening–Shaker– Lie flat on flat surface (nothing under your head) with shoulders flat– Engage anterior neck musculature to pull your chin toward chest– Part 1: Hold for 60 seconds, rest for 30 seconds and repeat– Part 2: Make controlled repetitive movement 30 timesDepartment of Otolaryngology—Head and Neck Surgery
Exercises/Maneuvers Laryngeal Vestibule Closure–Super-Supraglottic Swallow Take material into your mouth Hold your breath and BEAR DOWN Swallow HARD Cough/throat clear immediately after Swallow againDepartment of Otolaryngology—Head and Neck Surgery
Exercise LogDepartment of Otolaryngology—Head and Neck Surgery
RadiationToxicities
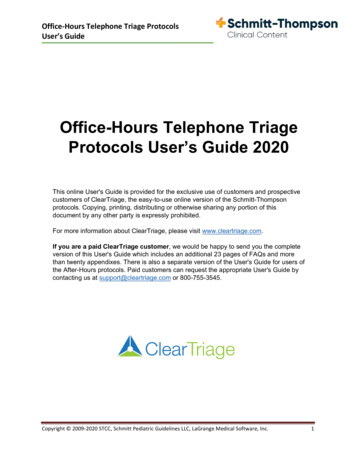
Acute (during treatment and up to3months post) Chronic (6 months post treatmentand longer) Thick saliva/ropey saliva (xerostomia) Dry mouth (xerostomia) DysphagiaDysphagiaChanging taste (dysgeusia)RadiationToxicities Changing taste, sensory changesVoice changes /hoarsenessVoice changes /hoarsenessTrismusTrismusHearing lossHearing lossMucositisDermatitisFatigueSoft tissue edema Painful swallowing (odynophagia)NauseaOsteoradionecrosisCranial Nerve PalsyDental caries (cavities)LymphedemaFibrosisDepartment of Otolaryngology—Head and Neck Surgery
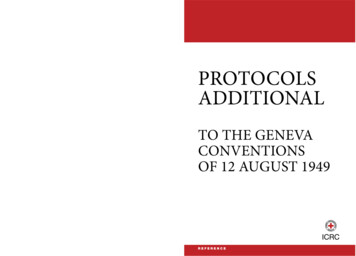
Common Radiation Toxicities (Side Effects)Weeks 1-2Weeks 3-4MILDHIGHVARIABILITYChanges in taste,drier mouth, milddiscomfort, fatigue,redness of skin,inflammation oftissueSide effects intensify,appetite decreases,meal intakedecreases,swallowing maybecome more difficultWeeks 5-7Post-treatmentWORSENINGWORSE THENBETTERIncreased mucositisand pain, increasedpain with swallowing,increased risk ofaspiration, voicechanges, depressionRemains challenging oreven gets worse.Improvements begin 2-3weeks later withdecreasing odynophagia,mucositis, improvingtaste and xerostomiaDepartment of Otolaryngology—Head and Neck Surgery
Odynophagia (mouthpain/sores) Avoid hard, crunchy foods. Creamy, bland foods tend to be best toleratedBaking soda and salt rinse (Marily et al,2003)Good oral cares, using alcohol-freemouthwashes and soft bristled brushesViscous lidocaine, Magic Mouthwash,Pain medications per MDCryotherapy for chemotherapy patients(Daugėlaitė et al, 2019)Honey (Liu et al, 2019)Aloe Vera Juice?Department of Otolaryngology—Head and Neck Surgery
Dry Mouth and/or ThickSaliva (Xerostomia) Increase water intake! Baking soda and salt rinse Sugar-free lozenges Artificial saliva products- Biotene, Xylimelts Avoid caffeine and alcohol Humidifier by bed Add moisture/sauces to food Spritz food with olive oil Good oral cares Suction machine may be needed
Dysgeusia Baking soda and salt rinse Avoid metal silverware andcanned foods Avoid beef if taste is off or bad Avoid pungent or strong spices Pay attention to food/drink temperature Focus on creamy and high-protein foods (yogurt, pudding, cottagecheese, shakes) Keep trying! Taste will varyDepartment of Otolaryngology—Head and Neck Surgery
Diet sheetDepartment of Otolaryngology—Head and Neck Surgery
The UIHC Treatment ApproachInitial EvaluationWeekly or Bi-WeeklyTherapy DuringTreatment4-7 sessionsPost-treatmentTherapyDepartment of Otolaryngology—Head and Neck Surgery
The UIHC Treatment Approach – Post-TreatmentTherapy–Post-treatment therapy–Common meeting points:– 1 month post-radiation completion– 3 months post-radiation completion– 6 months post-radiation completion– 9 months post-radiation completion– 12 months post-radiation completion–OPMS/FEES– Frequently completed at 1, 3 or 6 months post-radiation completion– Swallow function at 6 month predicts long-term function (Logemann, 1998)Department of Otolaryngology—Head and Neck Surgery
RT /- Chemo Dysphagia Management – AfterTreatmentHow do we keep progressing toward patient goals?–Toxicity Status–PO Status–PEG Tube Status–Exercise Status–Lymphedema StatusDepartment of Otolaryngology—Head and Neck Surgery
RT /- Chemo Dysphagia Management – AfterTreatmentHow do we keep progressing toward patient goals?–Toxicity Status Re-rank toxicities and provide management recs Provide education re: longevity of toxicities‒ Odynophagia likely will resolve in the weeks/months following completion of C/RT‒ Dysgeusia may take as long as 18 mo. to resolve and may always be somewhataltered Muted taste overall Changed taste preferences‒ Xerostomia may improve somewhat but will likely be a life-long side effectDepartment of Otolaryngology—Head and Neck Surgery
RT /- Chemo Dysphagia Management – AfterTreatmentHow do we keep progressing toward patient goals?–PO Status Rate intake level with FOIS‒ If not at general diet, what is/are barrier(s)? Re-assess functional status with PO trials Make recommendations for FEES/OPMS as indicated‒ Assess new level of function‒ Biofeedback for recommended strategies/maneuversDepartment of Otolaryngology—Head and Neck Surgery
RT /- Chemo Dysphagia Management – AfterTreatmentHow do we keep progressing toward patient goals?–PEG Tube Status Estimate % of intake via PEG vs PO What are the limiting factors? PEG weaning "plan", including repeat visit with dietician if indicated–Sample PEG weaning plan: Replace 1 can/carton of formula with a calorically equal amount of PO. Continuefor 3-4 days. If well tolerated, then remove a second can/carton. Repeat until allintake is by mouth.Department of Otolaryngology—Head and Neck Surgery
RT /- Chemo Dysphagia Management – AfterTreatmentHow do we keep progressing toward patient goals?–Exercise Status Status of recommended post-treatment home exercise program‒ Continuation of aggressive exercise regimen until initial 1 mo. f/u As diet level increases, aggressive exercises less indicated Once tolerating general diet, will typically switch to "maintenancemode"‒ Typically Masako, Mendelsohn, Effortful, 1 set of 10 reps dailyDepartment of Otolaryngology—Head and Neck Surgery
RT /- Chemo Dysphagia Management – AfterTreatmentHow do we keep progressing toward patient goals?–Lymphedema Status Visual Assessment – external and internal, if available Tactile Assessment May provide some basic, initial massage strategies, however referral to local CLTand/or referral to Tactile Medical next most appropriate step–Important to "get ahead" of the lymphedema as it can be the first stepstoward fibrosisDepartment of Otolaryngology—Head and Neck Surgery
RT /- Chemo Dysphagia Management – AfterTreatment Provide ongoing dysphagia treatment as indicated–Compensatory strategies–Life-long swallowing maintenance program–Expiratory muscle strength training (EMST), as appropriate Particularly in cases of weak cough and/or chronic aspiration Maximize cough strength, potentially indirectly increase pharyngeal swallowstrength (Hutcheson, et al 2018)–Try to give patient best tools to maintain safe PO intake and avoid lateonset RADDepartment of Otolaryngology—Head and Neck Surgery
Late Dysphagia - Hutcheson et al, 2012 Case Series 29 Patients with late dysphagia ( 5 years s/p fin)w/dysphagia symptoms referred for MBS (OPMS)Department of Otolaryngology—Head and Neck Surgery
Late Dysphagia - Hutcheson et al, 2012 Results–All patients showed pharyngeal stasis–79% (23/29 patients) showed silent aspiration–86% developed aspiration PNA and 62% developed recurrent PNAs–No patient demonstrated durable improvement with rehabilitative, nonsurgical treatmentsDepartment of Otolaryngology—Head and Neck Surgery
CaseStudiesWhat Would You Do?
JL Case Study #1 71 y.o. male (70 at time of diagnosis)– L tonsil p16 SCC identified Sept 2019– CT scan showed reactive 2b node (local spread)– Stage I (pT1, pN1, cM0, p16 )– Other: hx of unintentional 30lb weight loss in 2019,COPD, PEG placed in October at outside hospital Initial surgical treatment: Left level Ib, II-IV neck dissection with prep forTORS, January 3, 2019 Left radical tonsillectomy (TORS) and rightsimple tonsillectomy, January 8, 2019Department of Otolaryngology—Head and Neck Surgery
JL Case Study #1 Recommendations:– Radiation: 66 gray in 33 fractions (6.5 weeks)– Chemotherapy: low dose weekly cisplatin paclitaxel Referred to Speech Pathology– OPMS/VFSS completed March 16, 2020– Had been eating 50% by mouth (puree/drinks) and 50% by PEG– Oral mechanism exam remarkable for: mild left deviation of tongue, L Rlingual strength, mildly reduced lateralization, mildly reduced palatalelevation, s/p full mouth tooth extractionOPMS/VFSS ClipDepartment of Otolaryngology—Head and Neck Surgery
JL Case Study #1 OPMS/VFSS Findings:– Oral preparatory phase: Moderate Deficits: difficulty with mastication due to lack of dentition– Oral phase: Normal– Pharyngeal phase: Moderate-Severe Deficits: prolonged transit time, reduced hyoid/laryngeal elevation, laryngeal closure,vallecular stasis, pyriform stasis, reduced pharyngeal contraction and reduced tonguebase to pharyngeal wall contact, in A-P view bolus diverts to left– Cervical-esophageal phase: Mild-moderate Deficits: decreased dilation, impact of osteophytes?– Penetration/Aspiration scale: 3 and 5 with thin and nectar liquids; 7 and 8with thin liquidsDepartment of Otolaryngology—Head and Neck Surgery
JL Case Study #1 - Your Turn What maneuvers could you try?– Right head turn?– Left head turn?– Chin tuck?– Super supraglottic swallow?– Small bites? Bigger bites?– Head extension?– Double swallow?– Intentional cough? What consistencies would you try?– All?– Avoid anything specific?Department of Otolaryngology—Head and Neck Surgery
JL Case Study #1 – What did I try? My goals: KEEP HIM SWALLOWING, DETERMINEAPPROPRIATE DIET RECOMMENDATION DURING CxRT What worked? What didn't?–Not helpful: chin tuck not effective in clearing residuals–Helpful: Left head turn double swallow improved swallow safety, butwas not effective in clearing pharyngeal residue of solids. Smallbites/sips, alternating liquids and solids and multiple swallows werehelpful in reducing pharyngeal residue (i.e., efficiency).Department of Otolaryngology—Head and Neck Surgery
JL Case Study #1 – What would you recommend? What exercises would be helpful?–Anything you would avoid? Would you recommend oral intake? If so, what? Would you recommend any maneuvers?–If so, how could we remind him to use these maneuvers?Department of Otolaryngology—Head and Neck Surgery
JL Case Study #1 – What I recommended Diet:– Runny purees with multiple effortful swallows, thin liquids with LEFT head turn andmultiple swallows– Continue PEG to maintain adequate nutrition and hydration– KEEP SWALLOWING! Exercises:– Initially given a more expansive list of exercises, but list was shortened given lack ofcompliance– Masako Manuever– Effortful Swallow– Mendelsohn Maneuver– Maximal oral cavity opening– Neck stretchesDepartment of Otolaryngology—Head and Neck Surgery
JL Case Study #1 – Treatment During Treatment:–Seen 6x by SLP team, radiation completed April 24, 2020–During the 4th week, onset of odynophagia, dysgeusia and xerostomiasignificantly worsened. Utilized pain medications, Magic Mouthwashand baking soda and salt rinses–PO intake significantly decreased, with goal aiming to attempt 3-5xbites of puree, 2-3x per day–Exercise completion remained poor, focused on completing even 5xrepetitions of exercises as ableDepartment of Otolaryngology—Head and Neck Surgery
JL Case Study #1 – Outcome Post-treatment:–July 2020: Seen 3 months after CxRT completion with continued poor PO intake dueto perceived increased effort required OPMS/VFSS recommended EAT10 score 25–July 2020: OPMS/VFSS completed. Slightly improved. Penetration persists, but noaspiration visualized. Left head turn no longer helpful! Difficulty with pharyngeal clearance due to prominent osteophytes at C5-C6. Recommended to continue Puree and Regular liquids, increasing intake as able.Follow up in 3 months. Message sent to Oto team re: osteophytes.Department of Otolaryngology—Head and Neck Surgery
JL Case Study #1 – Outcome Post-treatment:– September 2020: Seen 5 months after CxRT completion. Patient reports SIGNIFICANT improvement Eating by mouth consistently, including some soft/ground solids. Very anxious to have PEG removed. States he does NOT want any intervention forosteophytes Recommend repeat exam. FEES chosen given GI discomfort after barium. EAT10 score 5– September 2020: FEES completed. Mild pharyngeal retention with solids, which clears with doubleswallows and liquid wash. No penetration/aspiration. Recommend General diet PEG to be removed in 2 weeks!Department of Otolaryngology—Head and Neck Surgery
PH Case Study #2 71 y.o. male (69 at time of diagnosis)–R BOT p16 SCC identified Sept 2018–CT scan showed reactive 2A node, also level 3 adenopathy identified–Classified from Lip and Oral Cavity AJCC- Stage 3 – cT1 cN1 cM0 Initial surgical treatment:–Bilateral neck dissection (BND) levels 2A-4 November 2, 2018 withprep for TORS–TORS on November 6, 2018Department of Otolaryngology—Head and Neck Surgery
PH Case Study #2 After TORS, pathologically re-staged from HPV-MediatedOropharyngeal Cancer AJCC– Stage 1 (pT1 pN1 cM0)–Pathology showed positive lateral margin Re-excision of glossotonsillar fold via TORS on 11/20/2019–Frozen margins negative 33 Fx of RT to tumor bed and bilateral neck commencedJanuary 3, 2019Department of Otolaryngology—Head and Neck Surgery
PH Case Study #2 Initial SLP evaluation 2 weeks into treatment (12/33 fxcompleted)–Oral mechanism exam unremarkable–Mild (1/10) odynophagia, "taste gone", increasing xerostomia–Full PO diet- avoiding hard/crunchy foods, 1 Boost/day–Clinical bedside suggested oral phases WNL, mildly reducedhyolaryngeal elevation Intermittent cough with thin liquidsDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Your Turn What diet recommendation? What exercises? Other recommendations or considerations?Department of Otolaryngology—Head and Neck Surgery
PH Case Study #2 – What I recommended Diet: General Diet/Thin liquids–OPMS/VFSS if cough appeared to worsen Exercises: MasakoMendelsohnEffortful SwallowPitch Glide ShakerNeck StretchesLingual ROMSuper-SupraglotticSwallowDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 – Outcome During Treatment:–Seen 5x by SLP team, radiation completed February 19, 2019–Dysgeusia and xerostomia continued to worsen throughout treatment–Minimal solid food at completion, mostly liquids/shakes–Completed 2-3 reps of each exercise per day Post-treatment:–RT Toxicities improving at 1 mo RTC, introducing more solids as tasteallows, intermittent cough w/thins observed. Recent chest CTconcerning for aspiration; OPMS/VFSS recommendedDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Outcome Post-treatment:–OPMS/VFSS Completed 5/8/2019 Findings Thickened epiglottis w/ reduced movement & reduced pharyngeal contraction resulted inreduced laryngeal closure and pharyngeal residueOverall inefficient swallow, increased residue for thicker consistenciesPenetration/aspiration scale- 7&8 with thin and nectar thick liquidsCough/swallow & Super-supraglottic swallow appeared to reduce (but not eliminate) pen/asp Recommendations Education about high risk of chronic aspirationGeneral diet/thin liquidsCough/re-swallow after every 2-3 bites/sipsEffortful swallow with every bite/sipContinue aggressive swallowing exercise program, pursue local dysphagia txDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Outcome Post-treatment: 8/29/19–General Diet/Thin liquids but NOTusing strategies–PT for shoulder pain–Local dysphagia therapy–Initiating lymphedema treatment Significant anatomical changes related to RT Concern for interarytenoid scarring/reduced glotticopeningDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Outcome Post-treatment: 9/16/19 OPMS/VFSS–Home diet: general diet/thin liquids- adding extra sauces, etc Results largely the same as previous except:–R head turn appeared to significantly reduce pen/asp–Cough/Swallow not effective at this time as it was leading toregurgitation from esophagusDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Outcome Post-treatment: 11/11/19 Clinic appt–Home diet: general diet/thin liquids- adding extra sauces, etc, not usingany recommended strategies Overall edema appeared to haveimproved slightly Glottic opening improved slightly Still significant abnormalityDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Outcome Post-treatment: 2/14/20 OPMS/VFSS–Home diet: general diet/thin liquids- adding extra sauces, etc, not usingany recommended strategies–Discharged from local dysphagia therapy Results largely the same as previous except:–R head turn did NOT reduce pen/asp–Super-supraglottic swallow reduced, but did not eliminate, pen/aspDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Outcome Post-treatment: 2/14/20 OPMS/VFSS Recommendations:–Continue current diet–Utilize super-supraglottic swallow–Consider regular follow-up with pulmonologist to monitor lung function–Consider use of expiratory muscle strength trainer (e.g., EMST150)–Continue maintenance frequency of Masako, Mendelsohn, effortfulswallowDepartment of Otolaryngology—Head and Neck Surgery
PH Case Study #2 - Outcome Post-treatment: 6/3/20 OPMS/VFSS– Home diet: General diet/thin liquids, not utilizing recommended strategies– EMST150 introduced, home program recommended Post-treatment: 10/7/20– Home diet: General diet/thin liquids, not utilizing recommended strategies,significant coughing with water intermittently– Discontinued EMST150 due to ear popping and intermittent nasalregurgitation– Recommend trying to implement super supraglottic swallow again.– Discussion about consideration of nectar thick fluids initiated as alternative*Department of Otolaryngology—Head and Neck Surgery
PH Case Study #3Department of Otolaryngology—Head and Neck Surgery
RM Case Study #3 68 y.o male (67 at diagnosis)–cT3N0 epiglottic mass identified 12/6/2019 Initial OPMS/VFSS 12/16/2019***Recommendations: General diet/thin liquidsDepartment of Otolaryngology—Head and Neck Surgery
RM Case Study #3 Admitted 1/02/2020 for hemoptysis– Received tracheostomy 1/9/2020 due to airway concerns– Repeat OPMS/VFSS performed 1/15/2020 ***Recommendations Mechanical Soft diet/thin liquids PEG placement for nutritional support during RT Digital occlusion or PMV with PODepartment of Otolaryngology—Head and Neck Surgery
RM Case Study #3 - Your Turn Diet recommendation appropriate? Why/Why not? What exercises? Other recommendations or considerations?Department of Otolaryngology—Head and Neck Surgery
RM Case Study #3 – What we recommended Exercises: MasakoMendelsohnEffortful SwallowPitch Glide ShakerNeck StretchesLingual ROMSuper-SupraglotticSwallowDepartment of Otolaryngology—Head and Neck Surgery
RM Case Study #3 – Outcome During Treatment:–Seen 7x by SLP team, radiation completed March 2020–Odynophagia worsened during final week of CRT–Mild Dysgeusia throughout–Xerostomia worsened during final week of CRT–Tolerance for PO significantly improved throughout treatment–Adherence to exercises improved throughout treatmentDepartment of Otolaryngology—Head and Neck Surgery
RM Case Study #3 – Outcome Post-treatment:–4 mo RTC (7/8/2020): Odynophagia and dysgeusia resolved, xerostomia improving No complaints/observations of dysphagia, consistencies only limited dueto edentulism–Decannulated by ENT 9/23/2020–Repeat OPMS/VFSS 10/2/2020 *** Recommendations: General Diet/Thin liquidsDepartment of Otolaryngology—Head and Neck Surgery
Questions? Comments?
Department of Otolaryngology—Head and Neck eduCHANGING MEDICINE.CHANGING LIVES.
Department of Otolaryngology —Head and Neck Surgery. Brian Peterson. Speech Pathologist II University of Iowa Hospitals and Clinics. Erin Logan. Speech Pathologist II. . Good oral cares, usi