Transcription
Quick guideApril 2021Qualityimprovementmade simpleWhat everyoneshould know abouthealth care qualityimprovement
Written by Bryan Jones, Esther Kwong andWill WarburtonAcknowledgementsThe authors would like to thank Joanna Bircher,Nick Black, Billy Boland, Mary Dixon-Woods,Tom Downes, Rosie Graham, Nigel Hart,Annie Laverty, Penny Pereira, Amar Shah,Iain Smith and Mirek Skrypak for their helpfulsuggestions and comments. We would also liketo acknowledge the authors of the previous 2013edition of this guide, which has been one of theHealth Foundation’s most popular and widelyused publications.When referencing this publication please usethe following URL:https://doi.org/10.37829/HF-2021-I05Third edition published April 2021.Second edition initially published in August 2013.The design of the guide was then updatedin 2016 to reflect the Health Foundation’srevised branding.Quality improvement made simpleis published by the Health Foundation,8 Salisbury Square, London EC4Y 8APISBN: 978-1-911615-56-9 2021 The Health Foundation
Contents1.Introduction2. What is quality and how can itbe improved?263.Underlying principles134.Approaches and methods265. Key questions for planning anddelivering quality improvement326.52Where can I find out more?References591
Introduction1
Why does qualityimprovement matter?Every health care system is built on a complexnetwork of care processes and pathways. The qualityof the care delivered by the system depends to a largeextent on how well this network functions, andhow well the people who provide and manage carework together.The overall aim is simple: to provide high-qualitycare to patients and improve the health of ourpopulation. Yet, as every patient and professionalcan testify, for every process or pathway that workswell, there is another that causes delay, wasted effort,frustration or even harm.Quality improvement is about giving the peopleclosest to issues affecting care quality the time,permission, skills and resources they need to solvethem. It involves a systematic and coordinatedapproach to solving a problem using specificmethods and tools with the aim of bringing about ameasurable improvement.Done well, quality improvement can deliversustained improvements not only in the quality,experience, productivity and outcomes of care, butalso in the lives of the people working in healthIntroduction3
care. For example, it can be used to improve patientaccess to their GP, streamline the management ofhospital outpatient clinics, reduce falls in care homes,or tackle variations between providers in the wayprocesses and activities are delivered.An understanding of quality improvement istherefore important for anyone who delivers ormanages care, as well as for people using care servicesand wondering how they could be improved.Through quality improvement there is the potentialto create a health care service capable of ensuring ‘noneedless deaths; no needless pain or suffering; nohelplessness in those served or serving; no unwantedwaiting; no waste; and no one left out’.1What is this guide about?This guide offers an explanation of some popularquality improvement approaches and methodscurrently used in health care and their underlyingprinciples. It also describes the factors that can helpto make sure these approaches and methods improvequality of care processes, pathways and services.4Quality improvement made simple
There are other methods and interventions thatcan improve quality of care, such as education,regulation, incentives and legal action, but these areoutside the scope of this guide.Who is this guide for?This guide is written for a general audience and willbe most useful to those new to the field of qualityimprovement, or those wanting to be remindedof the key points. It is aimed primarily at peopleeither working in or receiving health care, but is alsorelevant to social care and other public and thirdsector services, such as housing and education.Introduction5
What is qualityand how can itbe improved?2
What is quality?Within health care, there is no universally accepteddefinition of ‘quality’. However, the majority ofhealth care systems around the world have made acommitment to the people using and funding theirservices to monitor and continuously improve thequality of care they provide.In England, the NHS is ‘organising itself around asingle definition of quality’2: care that is effective, safeand provides as positive an experience as possibleby being caring, responsive and person-centred.This definition also states that care should also bewell-led, sustainable and equitable, achieved throughproviders and commissioners working togetherand in partnership with, and for, local people andcommunities (see Box 1). Health care systems acrossthe UK are also looking at the environmental impactof the services they provide as part of their efforts toimprove care quality.What is quality and how can it be improved?7
Box 1: The dimensions of qualityFor people who use servicesSafe Avoiding harm to people from care that isintended to help them.Effective Providing services based on evidence thatproduce a clear benefit.Experience Caring. Staff involve and treat people withcompassion, dignity and respect. Responsive and person-centred. Servicesrespond to people’s needs and choices andenable them to be equal partners in theirown care.For those providing servicesWell-led They are open and collaborate internallyand externally and are committed to learning andimprovement.Sustainable They use their resources responsibly andefficiently, providing fair access to all, and accordingto need of their populations.Equitable They provide care that does not vary inquality because of a person’s characteristics.8Quality improvement made simple
It is important that health care organisationsconsider all these dimensions when setting theirpriorities for improvement. Often the dimensionsare complementary and work together. However,there can sometimes be tensions between them thatwill need to be balanced. It is therefore necessaryto consider all stakeholders’ views and to worktogether to identify improvement priorities for anorganisation or local health care system.How can we improve quality?A long-term, integrated whole-system approachis needed to ensure sustained improvements inhealth care quality. Several factors (also discussedin Sections 3 and 5) are required to drive andembed improvements in a health care organisationor system.3–8Leadership and governance Establishing effective leadership forimprovement. Creating governance arrangements andprocesses to identify quality issues thatrequire investigation and improvement.What is quality and how can it be improved?9
Adopting a consistent, aligned and systematicapproach to improving quality. Developing systems to identify andimplement new evidence-basedinterventions, innovations and technologies,with the ability to adapt these to local context.Improvement culture, behaviours and skills Building improvement skills and knowledgeat every level, from the top tiers oforganisations, such as the boards of acutetrusts or primary care networks, through tofront-line staff. Recognising the importance of creatinga workplace culture that is conducive toimprovement. Giving everyone a voice and bringing staff,patients and service users together to improveand redesign the way that care is provided. Flattening hierarchies and ensuring thatall staff have the time, space, permission,encouragement and skills to collaborate onplanning and delivering improvement.10Quality improvement made simple
External environment Policy and regulatory bodies supportingefforts to develop whole-system approachesto improvement. Government ensuring that health and careservices are appropriately resourced to deliveran agreed standard of quality.What does qualityimprovement involve?Quality improvement draws on a wide variety ofapproaches and methods, although many shareunderlying principles, including: identifying the quality issue understanding the problem from a range ofperspectives, with a particular emphasis onusing and interpreting data developing a theory of change identifying and testing potential solutions;using data to measure the impact of eachtest and gradually refining the solution tothe problemWhat is quality and how can it be improved?11
implementing the solution and ensuringthat the intervention is sustained as part ofstandard practice.The successful implementation of the interventionwill depend on the context of the system or theorganisation making the change and requires carefulconsideration. It is important to create the rightconditions for improvement and these include thebacking of senior leaders, supportive and engagedcolleagues and patients, and access to appropriateresources and skills.12Quality improvement made simple
Underlying principles3
When participating in an improvement interventionfor the first time, it is not necessary to be an expertin quality improvement approaches and methods.However, before starting it is important tounderstand the core underlying principles that arecommon to most approaches and methods currentlybeing used in health care.Understanding the problemBefore thinking about how to tackle an improvementproblem, it is important to understand how andwhy the problem has arisen. Taking the time todo so, preferably by using a variety of data and incollaboration with a range of staff and patients, willhelp to avoid the risk of tackling the symptoms of theproblem instead of its root cause.One tool that can be used to identify the causesof the problem is a ‘cause and effect’ or ‘fishbone’diagram, which is designed to enable teams toidentify all potential causes, not just those that aremost obvious.9 After identifying the most likelycauses, teams can use a range of tools to investigatethem further, such as patient interviews, surveys andprocess mapping.14Quality improvement made simple
Process mapping is a tool used to chart each stepof a process. It is used to map the pathway orjourney through part, or all, of a patient’s healthcare journey and its supporting processes. Processmapping is especially useful as a tool to engage staffin understanding how the different steps fit together,which steps add value to the process, and where theremay be waste or delays. Mapping patient journeysinvolving multiple providers is also importantto identify any quality problems that occur at theinterfaces between teams and organisations.Designing improvementIt is important to allow enough time to design animprovement intervention and plan its delivery.Developing a specific aim and clear, measurabletargets is essential. Another key step is to alignthe aim of the intervention with wider service,organisational or system goals. This can help toattract support and resources from leaders andmanagers for a smooth implementation.It is also important to consider any challenges thatwill need to be addressed for the intervention toachieve its aims. A driver diagram10 is a useful wayof capturing these key issues and identifying theactivities required to tackle them. A logic model,11Underlying principles15
which sets out a theory of change about howan intervention is supposed to work, is anotherhelpful tool.When identifying an intervention, it is useful tolook at how other teams have addressed similarimprovement challenges. As well as providinginsights about what has and has not worked in othercontexts, it can help to avoid the risk of ‘reinventingthe wheel’ by repeating work that has already beencarried out elsewhere.Data and measurementfor improvementMeasurement and gathering data are vital elementsof any attempt to improve performance or qualityand are needed to assess the impact against setobjectives.12 When trying to assess the impactof a change to a complex system, a combinationof measures is often used, such as process andoutcomes measures. Measuring for improvementaims to identify the changes that occur while theintervention is being tested so that the interventioncan be refined over time in response to these data.16Quality improvement made simple
To measure change it is important to capturea baseline and then carry out measurement atregular intervals to gauge whether the impact ofthe intervention represents an improvement ordeterioration compared to the expected level ofperformance variation.It is also important to measure ‘what would havebeen’ without the intervention, bearing in mindany potential external causes of change seen inmeasurement. This can be done using statisticalprocess control (SPC), a method that examines thedifference between natural variation (commoncause variation) and variation that can be controlled(special cause variation). SPC uses control charts thatdisplay boundaries (control limits) for acceptablevariation in a process.Improving reliabilityA key focus of quality improvement is to improvethe reliability of the system and clinical processes.Ensuring reliability mitigates against waste anddefects in the system and reduces error and harm.Analysis of high reliability organisations, manyof which can be found in industries that havedeveloped and sustained high levels of safety, such ascommercial aviation and nuclear power industries,Underlying principles17
has identified a number of common attributes andbehaviours. These include a culture of ‘collectivemindfulness’ in which staff routinely look for andreport minor safety problems and share a willingnessto invest time and resources in identifying andlearning from errors.13In health care, systematic quality improvementapproaches such as Lean (see Section 4) have beenused to: redesign system and clinical pathways create more standardised working procedures develop error-free processes that deliver highquality, consistent care and use resourcesefficiently.Other health care organisations have taken aproactive approach to safety by developing thecapacity to detect and assess system-level weaknesses(hazards and their associated risks) and introducinginterventions to address them (risk controls).14Demand, capacity and flowSome backlogs and delays in health care servicesare attributable to resource shortages or increasesin demand. A case in point is the backlog of18Quality improvement made simple
appointments and procedures created by theCOVID-19 pandemic. However, not all delaysare the result of capacity problems. It may be thatthe capacity is in the wrong place or is providedat the wrong time. To understand whether thereis a capacity shortfall in a service, it is necessaryto measure the demand (the number of patientsrequiring access to the service) and the flow (howand when a need for a service is met).For a process improvement to be made, there needsto be a detailed understanding of the variation andrelationship between demand, capacity and flow.For example, demand is often relatively stable andflow can be predicted in terms of peaks and troughs.In this case, it may be the variation in the capacityavailable that causes the problem (for example, howwork plans are scheduled, staff sickness, and plannedor unplanned leave).The relational aspectsof improvementWhen planning, designing and testing animprovement intervention it is important to focusnot just on the technical aspects of improvement,such as how to apply quality improvement methodsUnderlying principles19
and tools and to measure change, but also on therelational aspects of improvement. The way in whichthe team of people leading the intervention worktogether and how they communicate with otherswhose support they need, is likely to have a profoundinfluence on the success of the intervention. Theserelational issues are discussed in the remaining partof this section.Involving and engaging staffEvidence about successful quality improvementindicates that the method or approach used is notthe sole predictor of success, but rather it is theway in which the change is introduced.15 Factorsthat contribute to this include leadership, effectivecommunication,16 staff engagement and patientparticipation, as well as training and education.Engaging the people closest to the issue beingaddressed is especially important, but it can bechallenging. For example, many clinicians will bekeen to improve the quality of the service they offerand may already have done so through methodssuch as clinical audit, peer review and adoptionof best practice. However, they may be unfamiliarwith quality improvement approaches. For this20Quality improvement made simple
reason, capability building and facilitated supportare key elements of building clinical commitment toimprovement. Other important aspects include: involving the clinical team early on whensetting aspirations and goals ensuring senior clinical involvement andpeer influence obtaining credible endorsement – forexample, from the royal colleges involving clinical networks acrossorganisational boundaries providing evidence that the change has beensuccessful elsewhere embedding an understanding of qualityimprovement into training and education ofhealth care professionals.Clinicians are more likely to engage with the processif the motivation and reasons focus on improvingthe quality of patient care rather than on cost-cuttingmeasures.Nonetheless, it is important to ensure that allrelevant staff are engaged, not just clinicians.Managers, for example, can help to ensure thatUnderlying principles21
improvement is embedded into standard practice17and non-clinical staff, who are often the first pointof contact for patients, play a key role in improvingcare. Breaking down traditional hierarchies for thismultidisciplinary approach is essential to ensure thatall perspectives and ideas are considered.Co-producing improvementAt its best, quality improvement in health care isbuilt on an equal partnership between staff, patients,carers and the wider public. These partnerships arepart of a desire to move away from a staff-drivenapproach to improving care, in which patients aresometimes invited to participate, to a model wherestaff and patients make decisions that relate directlyto the patient’s care together.18Underpinning these partnerships is a sharedpurpose, which is informed by discussions on whatmatters most to patients19 and where they thinkimprovement efforts should be focused.20 Trust,openness and an ability to listen respectfully are keyto the success of these discussions.21 A willingness toconfront any power imbalances among participants,making it difficult for some participants to contributeequally, is also important.2222Quality improvement made simple
Creating such an environment is not alwaysstraightforward: patients may need support andtraining to make the transition to being ‘makersand shapers’23 of services, while professionals mayneed guidance on addressing certain issues, such asunconscious bias.It is important that organisations invest resourcesinto patient and public involvement in improvementand build up the necessary skills and knowledge tomaximise the time, expertise and commitment ofpatients, carers and the wider public.Building effective teamsHow improvement team members relate to eachother and work together has a critical bearing on thesuccess of the intervention. Treating each other withrespect and courtesy, listening carefully to the viewsof others and valuing their ideas, regardless of theirhierarchical position, are all behaviours that can helpthe team to work together more effectively.24Equally important are a willingness to learntogether and a sense of humility, founded on anawareness that no single person has the skills andexperience to solve a problem on their own. AnyUnderlying principles23
team disagreements should be resolved throughopen discussion, rather than by personal orpositional power.25Other vital attributes are the ability to ask questionsclearly and frequently, and to share knowledge andthoughts in a focused and timely fashion. These‘teaming’ skills26 help team participants to interacteffectively and efficiently.CollaborationCollaboration is an essential component of effectivelearning and improvement. Working collaborativelyand outside of traditional organisational boundariesoften provides the basis for understanding andaddressing improvement challenges. Networksand partnerships such as clinical audit networks,academic health science networks, primary carenetworks, the Q community (see Section 6)or other similar groups enable the sharing ofexperiences, knowledge and expertise within localhealth systems.Collaboration also provides opportunities forscaling up of techniques, learning and discussionand can drive continued developments in qualityimprovement.27 Health care quality improvement24Quality improvement made simple
strategies developed through collaborative networkscan be shared and adopted at regional or nationallevels and therefore have a wider uptake than thosedeveloped locally. This raises the standard of qualityand consistency of care across a broader landscape.28Underlying principles25
Approachesand methods4
Many of today’s quality improvement approaches andmethods were originally developed in industry and havebeen adapted for use in other sectors, such as health care.These industrial approaches have been used extensivelywithin health care for the past 30 years to improve specificcare processes and pathways, but their use has only beenembedded throughout a few large health care providerorganisations (see Section 5). Perhaps because of this, theevidence base for their effectiveness is relatively limited,although it is expanding with the increasing levels ofresearch into the implementation and impact of qualityimprovement interventions.The roots of many quality improvement approachesand methods can be traced back to the thinking aboutproduction quality control that emerged in the early1920s. During the 1940s and 1950s, quality improvementtechniques were further developed in Japan, pioneeredthere by the American experts W Edwards Deming,Joseph Juran and the Japanese expert Kaoru Ishikawa. Morerecently, Don Berwick has become known for his work inthe US, leading the pioneering work of the Institute forHealthcare Improvement (see Section 6). Several qualityimprovement approaches and methods draw from the workof these pioneers.Approaches and methods27
This section describes some of the most popularquality improvement approaches and methods. Theevidence has not yet evolved to the point where oneapproach can be recommended above another. Thechoice of approach or method is likely to dependto some extent on the nature of the problem beingaddressed and its context. Whatever approach ormethod is used, discipline is important, particularlyin terms of fidelity to the underlying principlesdescribed in Section 3.29,30Model for improvementThis is an approach to continuous improvementwhere changes are tested in small cycles that involveplanning, doing, studying, acting (PDSA), beforereturning to planning, and so on.31,32 These cycles arelinked with three key questions. ‘What are we trying to accomplish?’ ‘How will we know that a change is animprovement?’ ‘What changes can we make that will resultin improvement?’28Quality improvement made simple
Each cycle starts with hunches, theories and ideasand helps them evolve into knowledge that caninform action and, ultimately, produce positiveoutcomes. To measure the impact of each change,tools such as control charts are used (see Section 3).LeanThis approach has its origins in Japan’s car industry.It is a quality management philosophy based ontwo core values – to make customer value flow andrespect for people.33 In health care, Lean emphasisesthe patient’s central position to all activities and aimsto eliminate or reduce activities that do not add valueto the patient. This is achieved by applying Lean’soperational principles, which involve five steps forcontinuous improvement.1.Defining what is value-adding to patients.2.Mapping value streams (pathways thatdeliver care).3.Making value streams flow by removingwaste, delay and duplication from them.Approaches and methods29
4.Allowing patients to ‘pull’ value, such asresources and staff, towards them, so thattheir care meets their needs.5.Pursuing perfection as an ongoing goal.Clinical microsystemsThese are small groups of people who work togetherregularly to provide care to a specific group ofpatients.34–36 This approach is based on the principlethat the quality, safety and person-centredness of anentire health care system is largely determined bywhat happens in its constituent microsystems.A systematic approach has been developed toimprove microsystems focused on the 5Ps:patients, people, patterns, processes and purpose.Assessing the 5Ps helps to identify opportunities forimprovement, which are then addressed using themodel for improvement approach.Experience-based co-designThis is an approach that was designed in the UK –for and with the NHS. It aims to improve patients’experience of services, through patients and staffworking in partnership to design services or30Quality improvement made simple
pathways.37,38 Data are gathered through in-depthinterviews, observations and group discussionsand analysed to identify ‘touch points’ – aspects ofthe service that are emotionally significant. Staff areshown an edited film of patients’ views about theirexperiences, before staff and patients come togetherin small groups to develop service improvements.Approaches and methods31
Key questionsfor planning anddelivering qualityimprovement5
Q.A.What are the challenges to delivering qualityimprovement?In a review of 14 quality improvementprogramme evaluations funded by theHealth Foundation, 10 key challengeswere consistently identified from theprogrammes.39 These were:1.convincing peers that there is a problem2.convincing peers that the solutionchosen is the right one3.getting data collection and monitoringsystems right4.excess ambitions and ‘projectness’ –treating the intervention as a discrete,time-limited project, rather than assomething that will be sustained as partof standard practice5.the organisational context, culture andcapacities6.tribalism and lack of staff engagement7.leadershipKey questions for planning and delivering quality improvement33
8.balancing carrots and sticks – harnessingcommitment through incentives andpotential sanctions9.securing sustainability10. considering the side effects of change.However, the review also showed that if you takethe time to get an intervention’s theory of change,measurement and stakeholder engagement right, thiswill deliver the enthusiasm, momentum and resultsthat characterise improvement at its best.Q.A.34Can quality improvement have unintendedconsequences?Quality improvement does not always workand can have the unintended consequenceof diverting resource and attention withoutproducing benefit. Sometimes, change in onearea can cause a negative effect in another, forexample, improved early discharge might leadto increased readmission. In other instances,the overall impact of a quality improvementeffort may be negative. Leaders need toanticipate and monitor for these potentialunintended consequences using a set ofQuality improvement made simple
balancing measures and may need to makedecisions about scheduling or sequencingof initiatives.The scale of a quality improvementintervention, and the extent to which itis coordinated with other improvementefforts, also matters.40 An isolated small-scaleintervention to solve a problem in a specificteam or service may end up duplicatingwork carried out elsewhere or, by adopting asolution that varies from standard practice, itcould create a potential safety risk.Quality improvement is likely to be moreeffective if it is undertaken as a healthcare organisation or system-wide effort.Improvements to care processes andpathways need to be considered holistically,rather than as disconnected interventions,and then approached as a long-term,sustained change effort. An integrated,system-level approach also allows a broadrange of skills and expertise to be deployed tosolve improvement challenges.Key questions for planning and delivering quality improvement35
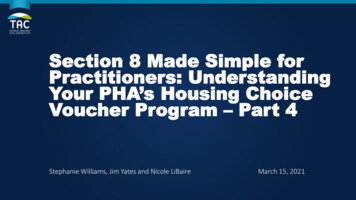
Q.A.What skills do improvers need?Quality improvement requires bothtechnical and relational skills.41,42 As wellas understanding how to plan, implement,measure and refine improvementinterventions using recognised methods,such as PDSA cycles, improvers need to beable, among other things, to describe theirintervention effectively and convince othersto work with them. Negotiation skills,the ability to read people and situationseffectively and work well in a team are vital togetting an intervention up and running.Practical skills, such as the capacity to managetime effectively, identify the right priorities,and keep a project delivery plan on schedule,are also essential. Equally important arelearning skills, particularly the ability toreflect, both individually and as a group,on the lessons learned from each step of anintervention – and to use these learnings torefine the improvement approach. Successfulimprovers have often developed certain‘improvement habits’, which help them to36Quality improvement made simple
get their ideas off the ground and ensure thattheir intervention is sustained.43 These habitsare summarised in Figure 1.Figure 1: The habits of improversQuestioningORESOMMCAU N I C ATCRETeamplayingCIA LIOAT I V I T YCriticalthinkingNComfortablewith conflictOptimisticIEN C ERGINCFacilitativeSILLECO-PTHALDNKAcceptingof changeINFLUENUNICAT IOMMNCOCING HUDEOANHIT EMS RNEmpatheticREProblem findingCalculatedrisk takingToleratinguncertaintyGeneratingideasSource: The habits of an improver: Thinking about learning forimprovement in health care. The Health Foundation; 2015.Key questions for planning and deliverin
Quality improvement made simple ISPUBLISHEDBYTHE(EALTH&OUNDATION 3ALISBURY3QUARE ,ONDON%# 9 !0 ISBN: 978-1-911615-56-9 4HE(EALTH&OUNDATION Written by Bryan Jones, Esther Kwong and Will Warburton Acknowledgements The authors would like to thank Joanna Bircher, Nick B