Transcription
eTELEMED 2016 : The Eighth International Conference on eHealth, Telemedicine, and Social Medicine (with DIGITAL HEALTHY LIVING 2016 / MATH 2016)Distributed Case Management in the Public Health AreaOctavian Purcarea, Philip Cummings, Doina Patrubani, Cristian TaslitchiEuropean Commission- DG Employment, Social Affairs & InclusionBrussels, BelgiumE-mails: octavian.purcarea@ec.europa.eu, phil@vmns.co.uk,dpatrubani@gmail.com, cristian.taslitchi@gmail.comAbstract – The free movement and mobility of citizens is afundamental principle of European Union (EU). Currently, thedata exchanges between social security institutions, includinghealthcare institutions are mostly paper-based. As aconsequence, the process is time consuming, open to error andlengthen the resolution time for the citizens. Efficient andeffective administrative cooperation between the institutions is,as a consequence, critical. Therefore, EU regulations triggeredthe European Exchange of Social Security Information(EESSI) project for the European Commission (EC) to providethe common secure framework that will facilitate electronicexchanges between relevant institutions. The previous attemptsof implementing a similar system failed mostly because theclerks are accustomed to work with paper documents and thecomplex paperless solutions were perceived by the nontechnical end-users as a major chance. The clerks need asystem able to handle a partial snapshot of the European case,developed around their current social, communication andprofessional context, able to manage operational processes and,at the same time, to provide an efficient decision support. Thepresent article describes the EESSI response to the maintechnical challenges encountered: the decomposition ofbusiness processes in order to provide a distributed casemanagement solution, composition of business processes inorder to provide standard functions across all case types,formalization of EESSI Business Messaging Protocol (BMP) inorder to provide semantic and syntactic interoperability andcase management visualization.Keywords-Public health data visualization; guidelines; timeline;case management; Business Process Modelling Notation(BPMN).I.INTRODUCTIONOrganisations have always been using the case paradigmto review and resolve various workflows like investigations,service requests and more. Typically, there are documentsand artefacts associated with a case that are reviewed byauthorised people in order to reach a resolution and close thecase.The case management model can be applied to diverseprocesses across a wide spectrum of industries andgovernment agencies. The normative practice that leads toresolving and closing the case used to be encapsulated inprocess and procedure handbooks, as well as “stored” in theclerks’ community experience and best practice knowledgewealth.The next wave of case management, after the paperbased one and often in parallel with it, was workflows thatsprang from last-generation software.Copyright (c) IARIA, 2016.ISBN: 978-1-61208-470-1In many industries, and most particularly in thehealthcare one, many organisations still find themselvesmired in IT systems that support only limited, if any,coordination across programs. Dating back to the 1980s,organisations were tethered to a legacy of large,disconnected transfer systems that took years to build, wereoutdated at implementation, and could not interoperate withone another. In the past, categorical funding requirementseffectively dictated separate infrastructures.New coordinated models ask healthcare organisations towork together and help connect people to services moreefficiently. In the past several years, as technology hasrapidly evolved, policymakers have begun to endorse theoperating models that support a vision of distributed dynamiccase management. These architectural guidelines recognizethe value of a service-oriented approach to IT, in whichtechnology components can be reused across organisationsand programs that have similar business processes. By usingdynamic case management applications, agencies can reducethe cost and complexity of both acquiring and supportingbusiness applications.Across the health care industry, information systemshave much to offer in managing costs and in improving thequality of care. In addition to the embedded role ofinformation technology in clinical and diagnosticsequipment, the systems are uniquely positioned to capture,store, process, and communicate timely information todecision makers for better coordination of healthcare at boththe individual and population levels.At the most general level, a striking feature of thehealthcare industry is the level of diversity that characterizespatients (e.g., physical traits and medical history),professional disciplines (e.g., doctors, nurses, administrators,and insurers), treatment options, healthcare deliveryprocesses, and interests of various stakeholder groups(patients, providers, payers and regulators).The healthcare delivery setting is characterized by atension between the need for orderly routines and the needfor sensitivity to variation in local conditions. As such, thecurrent market offering in healthcare in its diverseorganizational and regulatory settings covers severalorientations, among which:- Clinical Information Systems (CISs), which convert themedical data in relevant information about the patient’shealth status. The current CISs' market covers most ofthe healthcare provider operational needs in regard toclinical services with some degree of support for pointof care clinical decisions. The Graphical User Interfacefor documenting clinical cases is centred usually on202
eTELEMED 2016 : The Eighth International Conference on eHealth, Telemedicine, and Social Medicine (with DIGITAL HEALTHY LIVING 2016 / MATH 2016)--patient and patient banner in order to help the medicalpersonnel to easily identify the current patient clinicalcontext. This ensures a comprehensive standard-basedapproach in regards to CISs functionalities, which isregulated by the world’s leading medical informaticsorganizations: HL7 EHRS [1], CCHIT [2], Eurorec [3],etc. In this context, in order to analyse the current stateof the art, we need to structure the existing knowledge inthree domains: clinical pathway visualization, relevantmedical data visualization (medical and administrative)and the combination of these two - medical data inclinical context.Clinical pathway visualization should be consideredfrom two points of view: from the point of view ofclinical pathway encoder or designer, and from the pointof view of the one who is executing the patient currentclinical pathway requested actions. Projects/solutionslike Protégé [4], Tallis Toolset [5], GUIDE [6], GLARE[7], VisiGuide [8], AsbruView [9], etc., are suitable forencoding and/or execution of a clinical pathway, butwith limited adoption by the healthcare providers.Not necessary in relation with the clinical context,projects like Graphical Summary of Patient Status [10],Time Lines and LifeLines [11], PatternFinder [12],KNAVE and KNAVE-II [13], VISITORS [14], VIEVISU [15], Interactive Parallel Bar Charts (IPBC) [16],Gravi [17], and others moved in the direction ofvisualizing the medical relevant data.There are also very few combined approaches ofmedical data in clinical context: Guideline OverviewTool (GOT) [18], Midgaard [19], CareVis [20], NHSCommon User Interface [21], Visual-D [22], but most ofthem failed to be widely adopted.Patient Case Management Software, such as FAMCare Human Service [23] by Global VisionTechnologies, ClientTrack [24] by ClientTrack, Ahshay[25] by DataCare (the latter focusing on compensationindustry better management of medical treatment andbilling), Allscripts Care Management [26] by Allscripts,Penelope [27] by Athena Software, PracticePal [28] byPracticePal, etc. Such software are customised for thehealthcare industry and cover all or a specific mix offeatures like: Activity Tracking, Assessment Notes,Billing & Invoicing, Calendar Management, CandidateIdentification, Case List Management, Medical HistoryRecords, Patient Records, Referral Management,Treatment Planning, etc.Dynamic Case Management generic applications,which need customisation to match healthcare industryspecific requirements and context. Some of the mostsignificant software providers are: Pegasystems withPega Dynamic Case Management [29], Be Informedwith Be Informed Business Process Platform [30], KanaSoftware with Kana Enterprise [31], IBM with IBMCase Manager [32], Isis Papyrus with Papyrus Platform[33] (including Framework Solution for ACM), Appianwith Appian BPM Suite [34], OpenText with OpenTextCordys [35], OpenText BPM Everywhere [36],OpenText Process Intelligence [37], OpenText CordysCopyright (c) IARIA, 2016.ISBN: 978-1-61208-470-1and Process Component Library [38], EMC with EMCDocumentum xCP [39], Kofax with Kofax TotalAgility[40], Whitestein Technologies with Living SystemsProcess Suite [41], DST Systems with AWD10 [42],Oracle with Oracle BPM Suite 12c [43], and HylandSoftware with OnBase [44].The applications listed are characterised by variousdegrees of strong design time case managementcombined with strong runtime case management supportuse cases. There are two variations of Dynamic CaseManagement generic applications, variations describedbelow.Strong design time case management – capability thatassumes that 90% or more of what the user will do isdeveloped, tested, and deployed prior to user gettingstarted. Case workers have less flexibility, e.g., addingnew tasks or involving other users, and the overallprocess flow is well defined and more repeatable. Theseuse cases tend to be more production oriented; ons.Strong runtime case management support – use caseswhere work is highly variable. The way in which thecase unfolds over time is far less predictable. The caseview is altered by user actions and system events, withusers who are able to add tasks, processes andparticipants on the fly at the point of need.The requirements that we had to meet for the EESSIproject were focused on cross-European Member Statecooperation between social security institutions through anelectronic platform capable of supporting the current andfuture ability of all social security institutions to connect andfulfil their legal obligations of social security coordinationthrough electronic exchange. Subsequent to market offeranalysis, it was determined that the optimal approach was forthe solution to be designed and developed in-house. Thechallenges and the way responses were elaborated to meetthem are described in the next sections.The paper structure, section by section, is presentedbelow: Section II describes the business area that we arefocusing on, public health and social security data exchange,Section III describes the system principles and high levelarchitecture, Section IV describes the main challenges in theproject implementation, Section V presents the response tothe previously described challenges, Section VI refer to theproject adoption, Section VII brings up the conclusions andfuture work and Appendix 1 depicts the system mainfeatures.II.PUBLIC HEALTH DATA EXCHANGE IN THE CONTEXTOF EESSIBetter cooperation between social security institutions isa necessity in an increasingly mobile society in order for EUcitizens to exercise their right to free movement and securetheir social security rights.The EU provides common rules to protect social securityrights of citizens when moving within Europe. The Europeanrules of coordination make sure that social security203
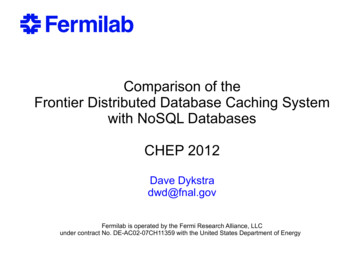
eTELEMED 2016 : The Eighth International Conference on eHealth, Telemedicine, and Social Medicine (with DIGITAL HEALTHY LIVING 2016 / MATH 2016)institutions of the EU plus Iceland, Norway, Liechtensteinand Switzerland, all communicate with each other to ensuresocial security rights are addressed correctly.Currently, these data exchanges between the socialsecurity institutions are mostly paper-based and as aconsequence are time consuming, open to error and lengthenthe resolution time for the citizens, partly due to the methodof exchange.Efficient and effective administrative cooperationbetween the institutions is therefore critical and as aconsequence the revisions of the European rules ofcoordination that came into force on May 1st, 2010 stated that"The transmission of data between the institutions or theliaison bodies shall be carried out by electronic means eitherdirectly or indirectly through the access points under acommon secure framework that can guarantee theconfidentiality and protection of exchanges of data."[45].Therefore, the aforementioned requirement of the EUregulations triggered the EESSI project for the EC to providethe common secure framework that will facilitate electronicexchanges between relevant institutions.The overall vision for the EESSI project is to deliver anelectronic platform that will support the current and futureability of all social security institutions to connect and fulfiltheir legal obligations of social security coordination throughelectronic exchange.The EESSI platform has to enable secure exchanges forall relevant business messages that guarantee confidentiality,integrity and availability, and to have a sufficient level ofvalidation. It should ensure wherever possible the rightmessage is sent to the correct recipient on the first occasionat a time that is suitable to all institutions and contributes tothe optimization of social security coordination.EESSI is a cross-sectorial platform with competences inthe area of public health. The main EESSI use cases in thearea of public health are the following:- Entitlement for short or long term healthcare relatedbenefits;- Validation of the person’s right to healthcare relatedbenefits during his/hers temporary stays in anotherMember State;- Establishing the reimbursement rates for healthcareservices;- Cost reimbursement based and fixed amountsreimbursement or healthcare services;- Certificate the incapacity of work and costreimbursement for incapacity of work;- Request for medical examinations or administrativechecks, etc.III.PRINCIPLES AND HIGH LEVEL ARCHITECTUREFigure 1 below, provides a high level view of theconceptual architecture. This section will provide anexplanation of the application domains in the conceptualarchitecture.Copyright (c) IARIA, 2016.ISBN: 978-1-61208-470-1Figure 1. Conceptual architecture diagramThe diagram depicts the conceptual principles on how theinter-connection is achieved:- A data exchange network interconnecting nationaladministrations;- National institutions are linked via national networksto the EESSI Access Points;-AP establishes the border between the national andinternational domains of EESSI end-to-end network.The APs are the gateways that enforce the statelessmessaging protocol; they check that the structure andthe semantic of the EESSI business messages arecorrect. A stateless protocol is a communicationsprotocol that treats each request as an independenttransaction that is unrelated to any previous requestso that the communication consists of independentpairs of request and response. A stateless protocoldoes not require the server to retain sessioninformation or status about each communicationspartner for the duration of multiple requests. Incontrast, a protocol, which requires keeping of theinternal state on the server is known as a statefulprotocol.The main principle in building the EESSI platform is“smart endpoints and dumb pipes” [46] [59], which meansthat in most of the cases, when a National Applicationreceives a request, it will apply the logic as appropriate andwill produce a response and the AP will perform a minimalstateless validation. The diagram depicts the twofundamental domains of the EESSI network:- The International Domain that hosts components,which are common to all participant countries. It isitself divided in two sub-domains: the CentralService Node (CSN) – designating the componentsthat will be hosted centrally (e.g., hosted by EC) andthe AP – a domain that holds components commonto all countries, developed centrally and assumed tobe hosted within each participant country. Thecomponents under the CSN and the APs, connectedelectronically as one system environment, constitutethe EESSI Platform, a secure, reliable, pan-Europeandata exchange platform;204
eTELEMED 2016 : The Eighth International Conference on eHealth, Telemedicine, and Social Medicine (with DIGITAL HEALTHY LIVING 2016 / MATH 2016)-The National Domain that hosts national specificelements of the network can also be divided in twosub-domains: the National Application (NA) andNational Gateways (NG).The NG are the National components thatspecifically integrate NA with the internationaldomain and the Institutions’ Domain – where theNA of the social security institutions resides.The NAs are the actual “client”; being themselvesdirect instruments of the “end-users”, the clerks.For a faster adoption of the EESSI platform and in orderto help the Member States (MS) to provide better services forthe citizens, the EC decided to provide an open sourceDistributed Case Management Solution called ReferenceImplementation for National Application (RINA). RINAconsists in a collection of infrastructure and communicationservices, foundation, repository and publishing services,business, integration and user interface services, which willprovide for clerks and their organizations, the tools toimplement the EESSI data exchange protocol based onStructured Electronic Documents (SED).IV.CHALLENGESThe main challenges are generated by the fact that EESSIis a peer-to-peer network where the International Domain ofthe platform, especially the Apps, are just the enablers of thecommunication between NAs, completely transparent fromthe business perspective.Formalization of EESSI vision started about 10 yearsago, and part of the project challenges at that time are stillpresent in the nowadays industry:- Formalization of EESSI Business MessagingProtocol in order to provide semantic and syntacticinteroperability.One of the main outcomes of EESSI is theinteroperability standard. The magnitude of theproject is emphasized by the following facts: multisectorial data-exchange, around 110 businesses usecases (BUC) with at least two application rolesinvolved, and around 320 business documents/SEDs.- Decomposition of business processes in order toprovide a distributed case management solution andcomposition of business processes in order toprovide standard functions across all case types.All the EESSI business processes/case types areforeseen to be distributed and they involve from theapplicative software perspective multiple applicationroles (e.g., case owner, counterparty, liaison body,etc.). Being a distributed system, the decoupling ofthe application roles in EESSI needs to be aligned tothe EC guidelines in terms of messaging, moreprecisely, web services and ebMS3 [47] - AS4profile [48]. Most of the Business ProcessManagement Systems [49] (BPMS) are able todecompose the processes but they are not nativelyable to decouple the application roles through webservices. The composition of business processes inorder to provide standard functions across all casetypes is available in the BPMS tools build on top ofCopyright (c) IARIA, 2016.ISBN: 978-1-61208-470-1-Business Process Modelling Notation (BPMN) [50][2] but the complexity and the multitude of theadministrative processes in EESSI makes BPMN asit is difficult to use.Case visualization and case visualization indistributed environment.It is obvious that the level of adoption of ing in EESSI is quite limited and the mainbarrier in adopting it comes from the fact thatimplementation does not take into account the enduser practices and their context.The clerks are accustomed to work with paperdocuments and previous attempts to create adistributed paperle
[33] (including Framework Solution for ACM), Appian with Appian BPM Suite [34], OpenText with OpenText Cordys [35], OpenText BPM Everywhere [36], OpenText Process Intelligence [37], OpenText Cordys and Process Component Library [38], EMC with EMC Documentum xCP [39], Kofax with Kofax Total